
Summary
Dihydropyridine calcium antagonists are established second line treatment for angina uncontrolled by β-adrenergic blockers. Amlodipine is a recently introduced, dihydropyridine with a long half life. In a double blind, placebo controlled, cross over trial we assessed the efficacy and safety of amlodipine in 20 patients with persistent angina despite treatment with atenolol. 17 male patients (mean age 58 y) completed the study. Two patients were withdrawn during placebo because of worsening angina and one withdrew whilst on amlodipine because of palpitations.
Compared with baseline, amlodipine prolonged exercise time to S-T segment depression by a median of 12.5%; significantly more than was found with placebo (median 0%). The improvement in exercise time and time to angina also tended to be greater for amlodipine than placebo. GTN consumption, at a median of 1.3/week, was significantly less with amlodipine than placebo (2.8). Attacks of angina were also reduced.
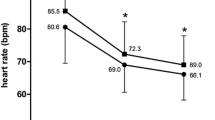
Standing systolic and diastolic blood pressures and sitting systolic blood pressure were lower with amlodipine than placebo. Heart rate did not change. There was no change in cardiac output (measured by doppler aortovelography) when amlodipine was added to atenolol. Holter monitor measurements of 24 h maximum and minimum heart rate, heart rate variation and extrasystole counts were the same for amlodipine and placebo.
In conclusion, amlodipine is effective in patients with angina inadequately controlled by atenolol alone, and does not interfer with cardiac rhythm or function.
Similar content being viewed by others


References
Akhras F, Jackson G (1991) Efficacy of nifedipine and isosorbide mononitrate in combination with atenolol in stable angina. Lancet 338: 1036–1039
Anonymous (1991) Calcium antagonist caution (editorial). Lancet 337: 885–886
Crawford MH (1987) The role of triple therapy in patients with chronic stable angina pectoris. Circ 75: V122-V127
Cocco G, Alfiero R (1991) A double-blind dose-response study of amlodipine in patients with stable angina pectoris. Eur Heart J 12: 169–174
Dargie HJ (1988) Beta blockers and calcium antagonists in angina pectoris. The potential role of combination therapy. Drugs 35 [Suppl 4]: 44–50
Distante A, Moscarelli E, Rovai D, L'Abbate A (1980) Monitoring of changes in cardiac output by transcutaneous aortovelography, a non-invasive Doppler technique: comparison with thermodilution. J Nucl Med Sci 24: 171–175
Hawley SK, Channer KS (1992) Relative effects of fat, carbohydrate and protein containing liquid diets on cardiac output in healthy adult subjects. Clin Sci 83: 483–487
Henry PD (1980) Comparative pharmacology of calcium antagonists: nifedipine, verapamil and diltiazem. Am J Cardiol 46: 1047–1058
Huntsman LL, Stewart DK, Barnes SR, Franklin SB, Colocorsis JS, Hessel EA (1983) Non-invasive doppler determination of cardiac output in man: clinical validation. Circ 67: 593–602
Klein W, Mitrovic V, Neuss M, Schlepper M, Cocco G, Prager G, Fitsche P, Meisner W (1991) A 6 week double-blind comparison of amlodipine in patients with stable exertional angina pectoris receiving concomitant beta-blocker therapy. J Cardiovasc Pharmacol 17 [Suppl 1]: S50-S52
Leon MB, Rosing DR, Bonow RO, Epstein SE (1985) Combination therapy with calcium-channel blockers and beta blockers for chronic stable angina. Am J Cardiol 55: 69B-80B
Murdoch D, Heel RC (1991) Amlodipine. A review of it's pharmacodynamic and pharmacokinetic properties, and therapeutic use in cardiovascular disease. Drugs 3: 478–505
Opie LH (1987) Calcium ions, drug actions and the heart. In: Denborough MA (ed) The role of calcium in drug action, Pergamon Press, Oxford New York
Osterloh I (1989) The safety of amlodipine. Am Heart J 118: 1114–1120
Packer M, Nicod P, Khandheria BR, Costello DL, Wesserman AG, Konstam MA, Weiss RJ, Moyer RR, Pinsky DJ, Abitton MH, Sovhrada JF (1991) Randomized multicenter double blind placebo controlled evaluation of amlodipine in patients with mild to moderate heart failure. J Am Coll Cardiol 17 [Suppl 1]: 274A
Pfisterer M, Muller-Brand J, Burkard F (1982) Combined acebutalol-nifedipine therapy in patients with chronic coronary artery disease: Additional improvement in ischaemia induced left ventricular dysfunction. Am J Cardiol 49: 1259–1266
Reed JV, Wickham EA (1988) Practical experience of minimisation in clinical trials. Pharmaceut Med 3: 349–359
Reicher-Reiss H, Barasch E (1991) Calcium antagonists in patients with heart failure. Drugs 42: 343–364
Singh S, Doherty J, Udhoji V, Smith K, Gorwit J, Bekheit S, Marker S, Stein W, Fellippo JS, Hedran P, Chen Y, Taylor C (1989) Amlodipine versus nadolol in patients with stable angina pectors. Am Heart J 118: 1137–1138
Temkin LP (1989) High dose monotherapy and combination therapy with calcium channel blockers for angina. Am J Med 86 [Suppl 1A]: 23–27
Taves DR (1974) Minimisation: A new method of assigning patients to treatment and control groups. Clin Pharmacol Therapy 15: 443–453
Winniford MD, Markham RV, Firth BG, Nicole P, Hills LD (1982) Haemodynamic and electrophysiologic effects of verapamil and nifedipine in patients on propranolol. Am J Cardiol 50: 704–710
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Woodmansey, P.A., Stewart, A.G., Morice, A.H. et al. Amlodipine in patients with angina uncontrolled by atenolol. Eur J Clin Pharmacol 45, 107–111 (1993). https://doi.org/10.1007/BF00315489
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00315489