
Abstract
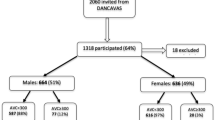
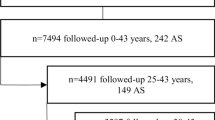
To disclose risk factors of incident aortic stenosis (AS) and progression of established AS. A prospective cohort study. The Tromsø Study, a population based health survey. Over a 14 years span we performed three repeated echocardiographic examinations (1994, 2001 and 2008) of a random sample of initially 3,243 participants. Data from the only hospital serving this population were included in the follow up. Throughout the study 132 participants were diagnosed with incident AS, defined as mean aortic valve gradient ≥15 mmHg. Cox proportional hazards regression disclosed age (HR 1.11, 95 %CI 1.08–1.14), systolic blood pressure (BP) (HR 1.01, 95 % CI 1.00–1.02), active smoking (HR 1.71, 95 % CI 1.09–2.67), and waist circumference (HR 1.02, 95 % CI 1.00–1.03) as independent predictors of incident AS. Analysis of risk factors for progression of AS disclosed a higher mean aortic gradient at first measurement (p = 0.015), weight (p = 0.015), a low haemoglobin (Hgb) (p = 0.030) and high density lipoprotein (HDL) (p = 0.032) as significant independent predictors. Age, systolic BP, smoking and waist circumference were independent predictors of incident AS, whereas cholesterol was not. Mean aortic gradient at first measurement, weight, an elevated HDL and low Hgb increase the progression rate of the disease. Our data indicate that calcific aortic valve disease is a distinct pathophysiological process, with age, smoking and “wear and tear” of the valve being major contributors to the disease development.

Similar content being viewed by others

References
Freeman RV, Otto CM. Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation. 2005;111(24):3316–26.
Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005–11.
Stewart BF, Siscovick D, Lind BK, et al. Clinical factors associated with calcific aortic valve disease. cardiovascular health study. J Am Coll Cardiol. 1997;29(3):630–4.
Lindroos M, Kupari M, Heikkila J, Tilvis R. Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. J Am Coll Cardiol. 1993;21(5):1220–5.
Eveborn GW, Schirmer H, Heggelund G, Lunde P, Rasmussen K. The evolving epidemiology of valvular aortic stenosis. The Tromso study. Heart. 2012;. doi:10.1136/heartjnl-2012-302265.
Kurtz CE, Otto CM. Aortic stenosis: clinical aspects of diagnosis and management, with 10 illustrative case reports from a 25-year experience. Medicine. 2010;89(6):349–79. doi:10.1097/MD.0b013e3181fe5648.
Chan KL. Is aortic stenosis a preventable disease? J Am Coll Cardiol. 2003;42(4):593–9.
Jacobsen BK, Eggen AE, Mathiesen EB, Wilsgaard T, Njolstad I. Cohort profile: the Tromso study. Int J Epidemiol. 2011;. doi:10.1093/ije/dyr049.
Ix JH, Shlipak MG, Katz R, et al. Kidney function and aortic valve and mitral annular calcification in the Multi-Ethnic Study of Atherosclerosis (MESA). Am J Kidney Dis. 2007;50(3):412–20. doi:10.1053/j.ajkd.2007.05.020.
Katz R, Wong ND, Kronmal R, et al. Features of the metabolic syndrome and diabetes mellitus as predictors of aortic valve calcification in the multi-ethnic study of atherosclerosis. Circulation. 2006;113(17):2113–9.
Stritzke J, Linsel-Nitschke P, Markus MR, et al. Association between degenerative aortic valve disease and long-term exposure to cardiovascular risk factors: results of the longitudinal population-based KORA/MONICA survey. Eur Heart J. 2009;30(16):2044–53. doi:10.1093/eurheartj/ehp287.
Perkovic V, Hunt D, Griffin SV, du Plessis M, Becker GJ. Accelerated progression of calcific aortic stenosis in dialysis patients. Nephron Clin Prac. 2003;94(2):c40–5. doi:10.1159/000071280.
Bahler RC, Desser DR, Finkelhor RS, Brener SJ, Youssefi M. Factors leading to progression of valvular aortic stenosis. Am J Cardiol. 1999;84(9):1044–8.
Palta S, Pai AM, Gill KS, Pai RG. New insights into the progression of aortic stenosis: implications for secondary prevention. Circulation. 2000;101(21):2497–502.
Rosenhek R, Binder T, Porenta G, et al. Predictors of outcome in severe, asymptomatic aortic stenosis. N Engl J Med. 2000;343(9):611–7. doi:10.1056/nejm200008313430903.
Nassimiha D, Aronow WS, Ahn C, Goldman ME. Association of coronary risk factors with progression of valvular aortic stenosis in older persons. Am J Cardiol. 2001;87(11):1313–4.
Yamamoto K, Yamamoto H, Yoshida K, et al. Prognostic factors for progression of early- and late-stage calcific aortic valve disease in Japanese: the Japanese Aortic Stenosis Study (JASS) Retrospective Analysis. Hypertens Res. 2010;33(3):269–74. doi:10.1038/hr.2009.225.
Rossebo AB, Pedersen TR, Boman K, et al. Intensive lipid lowering with simvastatin and ezetimibe in aortic stenosis. N Engl J Med. 2008;359(13):1343–56.
Cowell SJ, Newby DE, Prescott RJ, et al. A randomized trial of intensive lipid-lowering therapy in calcific aortic stenosis. N Engl J Med. 2005;352(23):2389–97. doi:10.1056/NEJMoa043876.
Rosenhek R, Rader F, Loho N, et al. Statins but not angiotensin-converting enzyme inhibitors delay progression of aortic stenosis. Circulation. 2004;110(10):1291–5. doi:10.1161/01.CIR.0000140723.15274.53.
Antonini-Canterin F, Hirsu M, Popescu BA, et al. Stage-related effect of statin treatment on the progression of aortic valve sclerosis and stenosis. Am J Cardiol. 2008;102(6):738–42. doi:10.1016/j.amjcard.2008.04.056.
Kamstrup PR, Tybjaerg-Hansen A, Nordestgaard BG. Elevated lipoprotein(a) and risk of aortic valve stenosis in the general population. J Am Coll Cardiol. 2014;63(5):470–7. doi:10.1016/j.jacc.2013.09.038.
Thanassoulis G, Campbell CY, Owens DS, et al. Genetic associations with valvular calcification and aortic stenosis. N Engl J Med. 2013;368(6):503–12. doi:10.1056/NEJMoa1109034.
Otto CM, Kuusisto J, Reichenbach DD, Gown AM, O’Brien KD. Characterization of the early lesion of ‘degenerative’ valvular aortic stenosis. Histological and immunohistochemical studies. Circulation. 1994;90(2):844–53.
Hermans H, Herijgers P, Holvoet P, et al. Statins for calcific aortic valve stenosis: into oblivion after SALTIRE and SEAS? An extensive review from bench to bedside. Curre Probl Cardiol. 2010;35(6):284–306. doi:10.1016/j.cpcardiol.2010.02.002.
Otto CM, Burwash IG, Legget ME, et al. Prospective study of asymptomatic valvular aortic stenosis. clinical, echocardiographic, and exercise predictors of outcome. Circulation. 1997;95(9):2262–70.
Yetkin E, Waltenberger J. Molecular and cellular mechanisms of aortic stenosis. Int J Cardiol. 2009;135(1):4–13. doi:10.1016/j.ijcard.2009.03.108.
Ortlepp JR, Hoffmann R, Ohme F, Lauscher J, Bleckmann F, Hanrath P. The vitamin D receptor genotype predisposes to the development of calcific aortic valve stenosis. Heart. 2001;85(6):635–8.
Dweck MR, Khaw HJ, Sng GK, et al. Aortic stenosis, atherosclerosis, and skeletal bone: is there a common link with calcification and inflammation? Eur Heart J. 2013;34(21):1567–74. doi:10.1093/eurheartj/eht034.
Roberts WC, Ko JM. Frequency by decades of unicuspid, bicuspid, and tricuspid aortic valves in adults having isolated aortic valve replacement for aortic stenosis, with or without associated aortic regurgitation. Circulation. 2005;111(7):920–5. doi:10.1161/01.cir.0000155623.48408.c5.
Acknowledgments
Tom Wilsgård for statistical support. This study was supported by the Northern Norway Regional Health Authorities (PhD Grant Number SFP-727-08).
Conflict of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Eveborn, G.W., Schirmer, H., Lunde, P. et al. Assessment of risk factors for developing incident aortic stenosis: the Tromsø Study. Eur J Epidemiol 29, 567–575 (2014). https://doi.org/10.1007/s10654-014-9936-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-014-9936-x