





Abstract
Aims The significance of mild residual descending aortic narrowing in post-coarctectomy patients is not known. The aim of our study was to investigate the influence of mild residual descending aortic narrowing on blood pressure and vascular damage in patients after repair of aortic coarctation.
Methods and results In 107 consecutive post-coarctectomy patients, magnetic resonance imaging, ambulatory blood pressure monitoring, and B-mode ultrasound of the carotid arteries were performed. A significant residual aortic narrowing was defined as: (i) a resting blood pressure gradient ≥30 mmHg with hypertension or exercise-induced hypertension (European Society of Cardiology guidelines); and/or (ii) a site of repair/diaphragmatic aorta ratio <0.7. Thirty-four patients (32%) had a significant residual aortic narrowing and were excluded from the analysis. Of the remaining 73 patients (43 male) with no or only mild residual descending aortic narrowing, median age was 29.8 years (range 17.1–52.5 years), mean age at repair 8.1 years (range 0.02–37.3 years), mean arm/leg gradient 2±12 mmHg, and mean common carotid intima--media thickness 0.612±0.118 mm. Thirty-three (45%) of these patients had hypertension. In multivariable regression analysis the site of repair/diaphragmatic aorta ratio was a strong and independent predictor of mean daytime systolic blood pressure (P<0.001) and common carotid intima--media thickness (P=0.027).
Conclusion Mild residual descending aortic narrowing in post-coarctectomy patients is independently associated with mean daytime blood pressure and carotid intima--media thickness. Our data suggest that a threshold for re-intervention of residual aortic narrowing lower than posed in current guidelines may be desirable to improve long-term outcome in these patients. However, further research on such aggressive interventional approaches is needed.
for the editorial comment on this article (doi:10.1093/eurheartj/ehi006)
Introduction
The definition of re-coarctation is variable and dependent on which diagnostic test is used. A significant aortic coarctation or re-coarctation is defined as ‘a peak pull-back gradient of more than 20 mmHg across the coarctation site at angiography in the presence of right arm hypertension’ and considered an indication for intervention by an international expert committee.1 Nowadays invasive diagnostics have been largely replaced by non-invasive imaging modalities, and therefore the most recent guidelines define significant (re)coarctation as ‘resting or exercise-induced hypertension and a resting arm/leg blood pressure gradient ≥30 mmHg’.2 However, patients with mild residual gradients not considered sufficient (based on these guidelines) to warrant intervention, may still have (mildly) elevated blood pressures, which may expose them to increased cardiovascular risk.3,4 To date, there are no data indicating that a further reduction of the gradient below any particular threshold will have clinical benefit.3 The aim of our study was to investigate the relationship of mild residual descending aortic narrowing with blood pressure and carotid intima--media thickness. Significant associations might indicate that further reduction of even mild residual aortic narrowing in patients after repair of aortic coarctation could be indicated to prevent additional organ damage.
Methods
Study design
From 2001 until 2002, 107 consecutive adult post-coarctectomy patients (70 male) participated in this observational study. The protocol was approved by our institutional review committee and informed consent was obtained from all participants. Medical records were reviewed for clinical history. Risk factors for atherosclerosis were assessed. Patients underwent 24 h ambulatory blood pressure monitoring, B-mode ultrasonography of the carotid arteries, exercise testing, and magnetic resonance imaging (MRI). Ambulatory blood pressure monitoring was used because it has been shown to be superior to conventionally measured blood pressure as predictor of cardiovascular events.5,6 B-mode ultrasound imaging of the carotid arteries can describe status and changes in intima--media thickness (IMT). It is a non-invasive measure and nowadays considered a validated and reproducible endpoint for atherosclerosis.7–9
Residual aortic narrowing was considered more than mild when at least one of the following criteria were met: resting or exercise-induced hypertension and a resting blood pressure gradient ≥30 mmHg between right arm and leg,2 or transverse aortic arch/diaphragmatic aorta ratio <0.7 or site of repair/diaphragmatic aorta ratio <0.7 at MRI.
Study protocol
Ambulatory blood pressure monitoring
An automatic ambulatory blood pressure monitor (Spacelabs 90207, SpaceLabs Inc., WA, USA) was placed on the right arm in all patients. Ambulatory blood pressure readings were only accepted when at least 85% of the measurements were successful. In accordance with The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7 report),10 patients were considered hypertensive when mean daytime systolic blood pressure was ≥135 mmHg and/or diastolic blood pressure was ≥85 mmHg.
B-mode ultrasonography of the carotid arteries
B-mode ultrasound images of the arterial far wall segments of the right and left common carotid artery, carotid bulb, and internal carotid artery were acquired according to a standardized protocol.11 All measurements were performed by one well trained and experienced sonographer. We used an Acuson 128XP ultrasound instrument (Acuson, Mountainview, CA, USA) equipped with an L7 5–10 MHz linear array transducer and Extended Frequency (EF) software. Readers blinded to all clinical information analysed the images. The mean IMTs of the common carotid artery, carotid bulb, and internal carotid artery were defined as the mean IMT of the near and far wall on both the left and right sides.
Exercise testing
Blood pressures were measured using an aneroid sphygmomanometer (Speidel and Keller Maxistabil 3, Welch Allyn, Jungingen, Germany). Supine systolic blood pressures in the right arm and leg were measured. Arm/leg ratio was calculated. All patients underwent a maximal, symptom limited, standardized treadmill exercise test following the Bruce protocol. Blood pressure was measured at regular intervals of 3 min by conventional sphygmomanometry. Exercise-induced hypertension was defined as normal ambulatory blood pressures and maximal exercise systolic blood pressure ≥200 mmHg.12,13 Exercise systolic blood pressure has been shown to be a strong independent predictor of mean daytime systolic blood pressure.14
Magnetic resonance imaging
Study subjects were placed supine in a 1.5 Tesla MRI scanner with high power gradients (Vision, Siemens, Erlangen, Germany). Magnetic resonance angiography was performed to visualize the thoracic and as much as possible of the abdominal aorta. Using multiple-image plane reconstruction (MPR) on-screen, the largest diameters of the narrowest part of the aortic arch, the descending aorta at the site of repair, and the descending aorta at the level of the diaphragm were measured. Both the transverse aortic arch/diaphragmatic aorta and the site of repair/diaphragmatic aorta ratios were determined. Aortic aneurysm was defined as a ratio of the descending aorta at the site of repair to the diaphragmatic aorta ≥1.5.15
Statistical analysis
Data are presented as mean±SD. Comparisons of continuous variables between groups were made by two-tailed, unpaired Student's t-tests. When comparing frequencies, we applied the χ2 test. Stepwise regression analyses were used to identify independent predictors of mean daytime systolic blood pressure and common carotid IMT in patients with no or only mild residual aortic narrowing. To assess the assumed linearity, scatterplots were inspected between dependent variables and all continuous predictors. To account for the inflation of the type I error due to multiple testing, we calculated adjusted P-values using the false discovery rate introduced by Benjami and Hochberg16 for multiple comparisons. All variables significantly associated with mean daytime systolic blood pressure and common carotid IMT in the univariate analysis were included in the multivariable regression model. The criterion for entry of variables was set at 0.05 and removal at 0.10. Histograms were plotted to check normality of the residuals of the regression models. Variables included in this analysis were body mass index (BMI), age, age at repair, gender, known sustained hypertension in patient's history (dichotomous), mean daytime systolic blood pressure, maximal exercise systolic blood pressure, cholesterol and smoking (for regression of IMT), arm/ankle blood pressure difference, and ratios of the aortic arch or site of repair to diaphragmatic aorta. We investigated the stability of the stepwise selection process of the regression models with a bootstrap procedure.17 The stepwise selection was performed in 1000 bootstrap samples, and for each predictor we counted how many times they were selected in the model; predictors that were selected in more than 50% were retained in the final regression models. All statistical tests were two-sided and differences were considered statistically significant at P<0.05. Data analysis was performed using the SPSS statistical package (10.01 for Windows, SPSS Inc., Chicago, IL, USA).
Results
Subjects
Of the 107 subjects, 34 patients (27 male) had a residual aortic narrowing which was more than mild and were therefore excluded from the analysis. Seventeen of these patients met the criteria of the European Society of Cardiology (ESC) guidelines. The other 17 patients were excluded because of a site of repair (or aortic arch)/diaphragmatic aorta ratio <0.7 at MRI. So, 73 patients had no or only mild residual aortic narrowing and were included in this study. Three patients had an aortic aneurysm. Eight patients (11%) were operated before the age of 1 year. Repair was performed by resection and end-to-end anastomosis in 52 patients (71%), patch angioplasty in 11 patients (15%), subclavian flap angioplasty in seven patients (10%), and graft interposition in three patients (4%). A ventricular septal defect was closed in six patients, ligation and resection of a patent arterial duct in seven patients, and resection of a subvalvular aortic stenosis in six patients. Three patients (two after end-to-end anastomosis, one after patch angioplasty) had undergone repeat surgery because of recoarctation. Three patients (one after end-to-end anastomosis, two after patch angioplasty) had been reoperated because of paracoarctation aneurysms. In five patients, aortic valve replacement had been performed because of aortic stenosis and/or regurgitation (two mechanical valves, one Bentall procedure and two Ross procedures).
Test results
Test results are shown in Table 1. Of the 73 subjects, 33 patients (45%) were hypertensive based on their clinical history and/or results of the ambulatory blood pressure monitoring. Nine of these patients were known to have hypertension and were on anti-hypertensive medication. Five of the 40 patients, normotensive at ambulatory blood pressure monitoring, had exercise-induced hypertension. Adequate imaging of the thoracic and abdominal aorta was obtained in all patients.
Predictors of ambulatory blood pressure and carotid IMT
Common carotid IMT was increased in all patient groups compared with the normal values given by Denarie et al.18 The variables associated with mean daytime systolic blood pressure and common carotid IMT in univariate analysis, were compared in the 73 patients with no or minimal residual aortic narrowing using multivariable stepwise regression analysis (Tables 2 and 3). BMI (P=0.001), maximal exercise systolic blood pressure (P<0.001), and the site of repair/diaphragmatic aorta ratio (P<0.001) were independently associated with mean daytime systolic blood pressure. The selection of BMI, maximal exercise systolic blood pressure, and the site of repair/diaphragmatic aorta ratio appeared to be stable because they were selected in 79.2, 95.2, and 94.9%, of the 1000 bootstrap samples, whereas age, age at repair, and hypertension based on patient's history were selected in only 20.0, 10.4, and 23.0%, respectively. Age (P<0.001), and the site of repair/diaphragmatic aorta ratio (P=0.027) were independent predictors of common carotid IMT. The selection of age, and the site of repair/diaphragmatic aorta ratio appeared to be stable because they were selected in 91.2 and 56.3% of the 1000 bootstrap samples, whereas age at repair, hypertension based on patient's history, mean daytime systolic blood pressure, smoking, and BMI were selected in only 23.7, 22.8, 13.7, 22.3, and 6.8%, respectively. When patients with an aortic aneurysm were excluded (N=3), age (P<0.001) and the site of repair/diaphragmatic aorta ratio (P=0.036) still had independent predictive value for common carotid IMT.
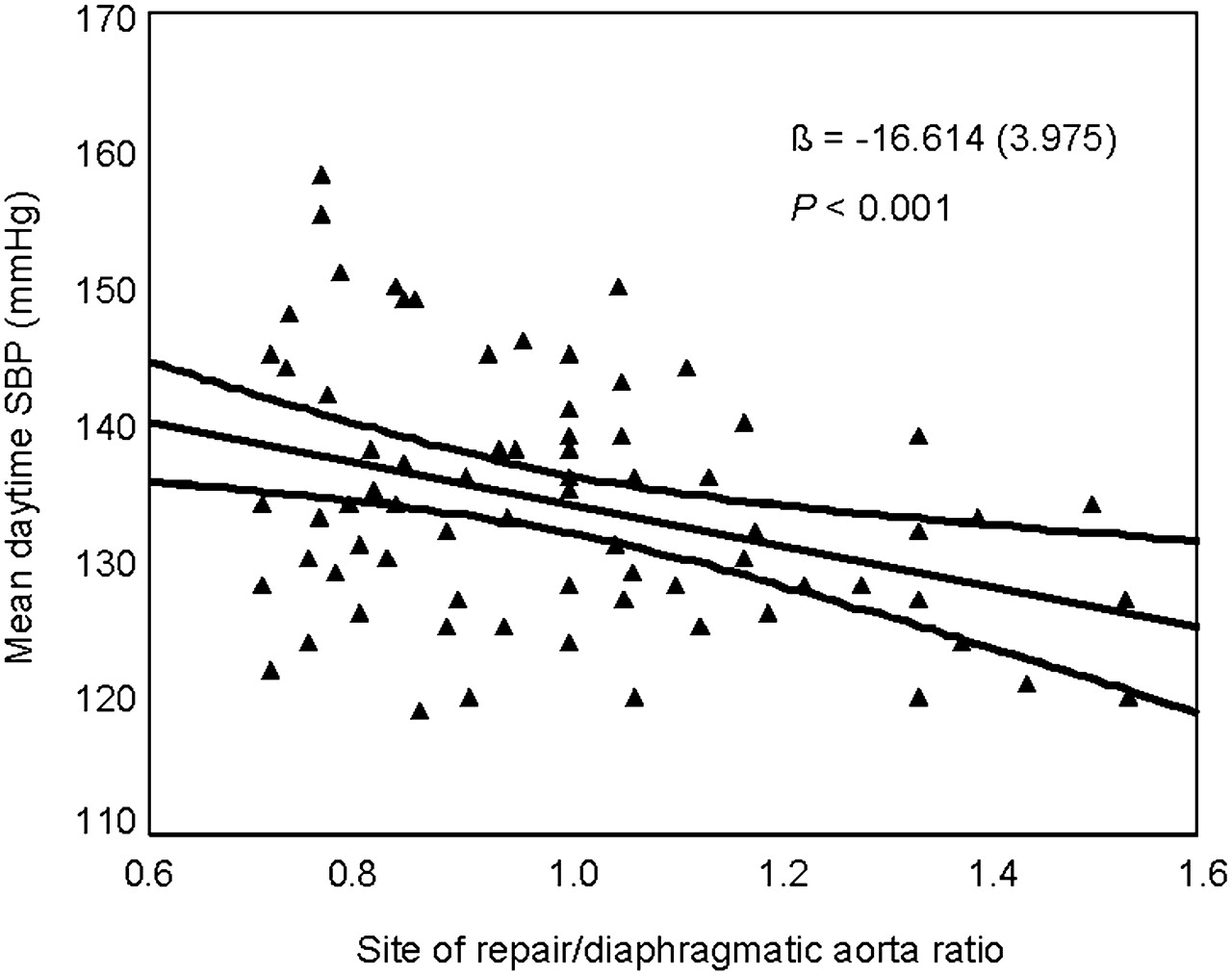
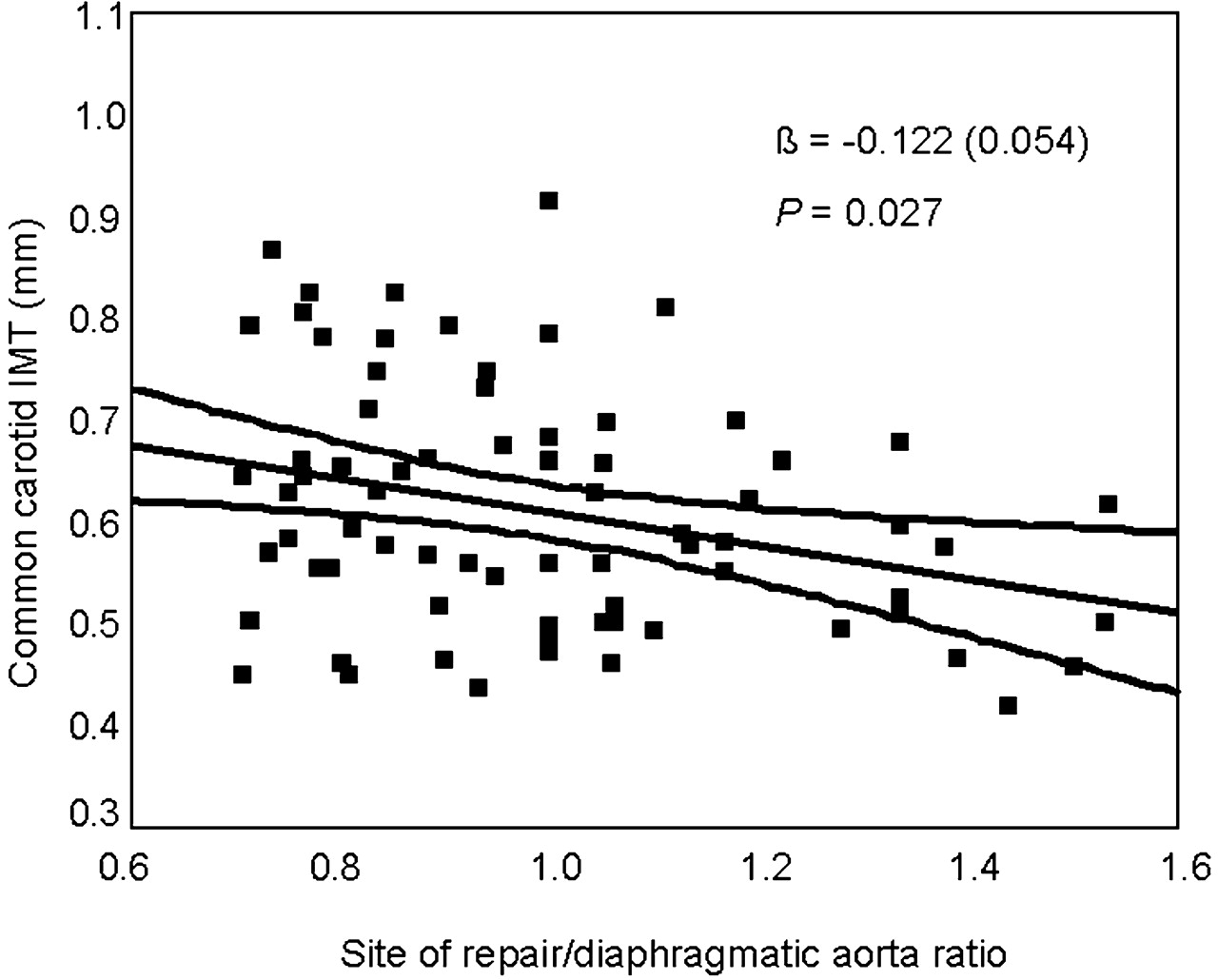
Figure 1 shows the relation between common carotid IMT and the site of repair/diaphragmatic aorta ratio in the 73 patients with no or only mild residual aortic narrowing. When corrected for significant confounders in multivariable analysis the relation was still significant [β=−0.122 (standard error 0.054), P=0.027]. Figure 2 shows the relation between mean daytime systolic blood pressure and the site of repair/diaphragmatic aorta ratio in these 73 patients. When corrected for significant confounders in multivariable analysis the relation was highly significant.
Discussion
Our study is the first to report the predictive value of mild residual descending aortic narrowing for blood pressure and vascular damage in patients after repair of aortic coarctation. The site of repair/diaphragmatic aorta ratio was independently associated with mean daytime systolic blood pressure and common carotid IMT.
The prevalence of re-coarctation after surgical repair of aortic coarctation is highly dependent on the age at repair, type of repair, and the definition used. In the past, most authors considered residual aortic gradients lower than 20 mmHg at catheterization to be satisfactory endpoints for treatment and non-intervention.1,19–21 But, nowadays routine catheterization for the post-operative assessment of patients after repair of aortic coarctation is rarely performed and has been replaced by non-invasive (imaging) modalities. Doppler echocardiography and especially MRI and blood pressure measurements in right arm and leg are often used in the post-operative assessment of post-coarctectomy patients.22 Arm/leg blood pressure gradients correlate with invasive haemodynamic findings and reflect the severity of narrowing in aortic coarctation. However, the definition of significant residual aortic gradient using non-invasive blood pressure measurements, as posed in current guidelines of the ESC,2 is based on consensus and not on clear clinical endpoints.
The results of our study show that in post-coarctectomy patients with no or only mild residual aortic narrowing mean daytime systolic blood pressure and carotid IMT are independently associated with site of repair/diaphragmatic aorta ratio as assessed by MRI. These novel and important findings suggest that, in patients who are considered successfully repaired based on current guidelines, mild residual aortic narrowing may be of prognostic significance and may contribute to raised blood pressure and concomitant vascular damage.
Prognosis of aortic coarctation patients is reduced even after successful repair. Coronary artery disease is, in 25–37% of the cases, the most common cause of late death, and late hypertension is largely held responsible for this premature coronary atherosclerosis.23,24 The cause of late systemic hypertension in patients after repair of aortic coarctation has been extensively investigated. The pathological mechanism thought to be involved is abnormal structure and function of the pre-coarctation arterial conduits. More collagen and less smooth muscle mass is present in the aortic arch leading to diminished arterial wall compliance and increased rigidity.25–28 Reduced baroreceptor sensitivity, residual aortic arch gradients (re-coarctation and/or hypoplastic aortic arch) may also be contributing factors.29–32 It is well known that both survival and the prevalence of hypertension of post-coarctectomy patients are greatly affected by age at operation and early repair of aortic coarctation is advocated.23,24,33,34 Nowadays, correction is recommended as soon as the diagnosis is made in order to reduce the risk of persistent or future sustained hypertension. However, despite early repair, some element of late hypertension is inevitable and will remain a major concern. Abnormal structural and functional properties of the proximal aorta and arteries have been found even in patients with successful repair in early infancy suggesting that the vascular abnormalities found in aortic coarctation patients cannot solely be attributed to the damaging effects of (preoperative) arterial blood pressure.35,36 Several authors have suggested that an innate and probably fixed abnormal structure and function of the pre-coarctation vessels exposes the proximal arterial tree to a harmful haemodynamic environment (i.e. raised blood pressure).37,38 Blood pressure functions both as cause and effect: increased blood pressure contributes to increased arterial stiffness, whereas arterial stiffness, in turn, increases systolic blood pressure.39,40 It seems likely that these developmental abnormalities and the damaging effects of pre- and post-operative hypertension in patients with aortic coarctation interact and explain the vascular abnormalities found in these patients.
Obviously, the aim of initial repair of aortic coarctation is complete relief of the obstruction. The results of our study suggest that even mild residual aortic narrowing may be related to adverse outcomes in patients who are presently considered successfully repaired based on current guidelines. Although the innate abnormalities of the arterial wall will remain unchanged and will continue to expose patients to a high risk of cardiovascular complications, additional harmful effects of increased blood pressure on the arterial wall might be prevented by a more aggressive approach towards mild residual aortic narrowing in these patients.
Rosenthal4 already suggested that, especially in view of the very good efficacy and safety profile of transcatheter techniques (i.e. stenting), the definition of successful treatment of aortic coarctation may need to be revised. Most patients with mild residual aortic narrowing will be suitable candidates for transcatheter treatment, which can be performed with very low morbidity. Especially in the full-grown patient, stent placement seems a particularly attractive option, resulting in an almost complete relief of the gradient in>95% of the patients.3,41 However, long-term follow-up of post-coarctectomy patients with mild residual aortic narrowing is needed before changing current treatment recommendations. Furthermore, the risks and benefits of intervention for mild, residual aortic narrowing in patients after repair of aortic coarctation is unclear and further research on such an aggressive approach is needed.
Conclusion
In post-coarctectomy patients, mild residual descending aortic narrowing is associated with mean daytime systolic blood pressure and carotid IMT. Mild residual aortic narrowing may therefore be of prognostic significance. Our data suggest that a threshold for re-intervention of residual aortic narrowing lower than presently stated in current guidelines may be indicated to improve long-term outcome in these patients. A prospective randomized trial is needed to confirm this hypothesis.
Figure 1. Relation of common carotid IMT and site of repair/diaphragm-atic aorta ratio in 73 post-coarctectomy patients corrected for age (calculated at mean age).
Figure 2. Relation of mean daytime systolic blood pressure (SBP) and site of repair/diaphragmatic aorta ratio in 73 post-coarctectomy patients corrected for BMI and maximal exercise systolic blood pressure (calculated at mean BMI and mean maximal exercise systolic blood pressure).
Characteristics and results in 73 patients with no, or only mild, residual aortic narrowing
| N=73 | |
|---|---|
| Gender (male/female) | 43/30 |
| Age (years, range) | 29.8 (17.1–52.5) |
| Age at repair (years, range) | 8.1 (0.02–37.3) |
| BMI (kg/m2) | 23.4 (3.3) |
| Blood pressures | |
| Mean daytime SBP (mmHg) | 134 (10) |
| Mean daytime DBP (mmHg) | 77 (9) |
| Nocturnal dip (%) | 13 (5) |
| Arm/leg pressure gradient (mmHg) | 2 (12) |
| Maximal exercise SBP (mmHg) | 186 (25) |
| Risk factors for CVD | |
| Cholesterol (mmol/L) | 4.0 (2.1) |
| LDL-cholesterol (mmol/L) | 2.3 (1.4) |
| Triglycerides (mmol/L) | 0.85 (0.63) |
| History of smoking (yes/no) | 21/52 |
| B-mode ultrasound of carotid arteries | |
| IMT common carotid artery (mm) | 0.61 (0.12) |
| IMT carotid bulb (mm) | 0.71 (0.15) |
| IMT internal carotid artery (mm) | 0.53 (0.12) |
| Magnetic resonance imaging | |
| Diameter aortic arch (mm) | 18 (3) |
| Diameter aorta site of repair (mm) | 18 (5) |
| Diameter aorta diaphragm (mm) | 18 (3) |
| Ratio aortic arch/diaphragm (mm) | 0.97 (0.14) |
| Ratio site of repair/diaphragm | 0.99 (0.22) |
| N=73 | |
|---|---|
| Gender (male/female) | 43/30 |
| Age (years, range) | 29.8 (17.1–52.5) |
| Age at repair (years, range) | 8.1 (0.02–37.3) |
| BMI (kg/m2) | 23.4 (3.3) |
| Blood pressures | |
| Mean daytime SBP (mmHg) | 134 (10) |
| Mean daytime DBP (mmHg) | 77 (9) |
| Nocturnal dip (%) | 13 (5) |
| Arm/leg pressure gradient (mmHg) | 2 (12) |
| Maximal exercise SBP (mmHg) | 186 (25) |
| Risk factors for CVD | |
| Cholesterol (mmol/L) | 4.0 (2.1) |
| LDL-cholesterol (mmol/L) | 2.3 (1.4) |
| Triglycerides (mmol/L) | 0.85 (0.63) |
| History of smoking (yes/no) | 21/52 |
| B-mode ultrasound of carotid arteries | |
| IMT common carotid artery (mm) | 0.61 (0.12) |
| IMT carotid bulb (mm) | 0.71 (0.15) |
| IMT internal carotid artery (mm) | 0.53 (0.12) |
| Magnetic resonance imaging | |
| Diameter aortic arch (mm) | 18 (3) |
| Diameter aorta site of repair (mm) | 18 (5) |
| Diameter aorta diaphragm (mm) | 18 (3) |
| Ratio aortic arch/diaphragm (mm) | 0.97 (0.14) |
| Ratio site of repair/diaphragm | 0.99 (0.22) |
Values are mean±SD. SBP, systolic blood pressure; DBP, diastolic blood pressure; CVD, cardiovascular disease.
Characteristics and results in 73 patients with no, or only mild, residual aortic narrowing
| N=73 | |
|---|---|
| Gender (male/female) | 43/30 |
| Age (years, range) | 29.8 (17.1–52.5) |
| Age at repair (years, range) | 8.1 (0.02–37.3) |
| BMI (kg/m2) | 23.4 (3.3) |
| Blood pressures | |
| Mean daytime SBP (mmHg) | 134 (10) |
| Mean daytime DBP (mmHg) | 77 (9) |
| Nocturnal dip (%) | 13 (5) |
| Arm/leg pressure gradient (mmHg) | 2 (12) |
| Maximal exercise SBP (mmHg) | 186 (25) |
| Risk factors for CVD | |
| Cholesterol (mmol/L) | 4.0 (2.1) |
| LDL-cholesterol (mmol/L) | 2.3 (1.4) |
| Triglycerides (mmol/L) | 0.85 (0.63) |
| History of smoking (yes/no) | 21/52 |
| B-mode ultrasound of carotid arteries | |
| IMT common carotid artery (mm) | 0.61 (0.12) |
| IMT carotid bulb (mm) | 0.71 (0.15) |
| IMT internal carotid artery (mm) | 0.53 (0.12) |
| Magnetic resonance imaging | |
| Diameter aortic arch (mm) | 18 (3) |
| Diameter aorta site of repair (mm) | 18 (5) |
| Diameter aorta diaphragm (mm) | 18 (3) |
| Ratio aortic arch/diaphragm (mm) | 0.97 (0.14) |
| Ratio site of repair/diaphragm | 0.99 (0.22) |
| N=73 | |
|---|---|
| Gender (male/female) | 43/30 |
| Age (years, range) | 29.8 (17.1–52.5) |
| Age at repair (years, range) | 8.1 (0.02–37.3) |
| BMI (kg/m2) | 23.4 (3.3) |
| Blood pressures | |
| Mean daytime SBP (mmHg) | 134 (10) |
| Mean daytime DBP (mmHg) | 77 (9) |
| Nocturnal dip (%) | 13 (5) |
| Arm/leg pressure gradient (mmHg) | 2 (12) |
| Maximal exercise SBP (mmHg) | 186 (25) |
| Risk factors for CVD | |
| Cholesterol (mmol/L) | 4.0 (2.1) |
| LDL-cholesterol (mmol/L) | 2.3 (1.4) |
| Triglycerides (mmol/L) | 0.85 (0.63) |
| History of smoking (yes/no) | 21/52 |
| B-mode ultrasound of carotid arteries | |
| IMT common carotid artery (mm) | 0.61 (0.12) |
| IMT carotid bulb (mm) | 0.71 (0.15) |
| IMT internal carotid artery (mm) | 0.53 (0.12) |
| Magnetic resonance imaging | |
| Diameter aortic arch (mm) | 18 (3) |
| Diameter aorta site of repair (mm) | 18 (5) |
| Diameter aorta diaphragm (mm) | 18 (3) |
| Ratio aortic arch/diaphragm (mm) | 0.97 (0.14) |
| Ratio site of repair/diaphragm | 0.99 (0.22) |
Values are mean±SD. SBP, systolic blood pressure; DBP, diastolic blood pressure; CVD, cardiovascular disease.
Univariate and stepwise multivariable regression analyses of mean daytime systolic blood pressure in 73 post-coarctectomy patients with no, or mild, residual aortic stenosis
| Explanatory variable | Univariate B (SE) | Stepwise multivariable B (SE) | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.881 (0.324) | 0.892 (0.261) | 0.001 |
| Age (years) | 0.322 (0.119) | ||
| Age at repair (years) | 0.303 (0.170) | ||
| Gender | 1.780 (2.280) | ||
| Hypertension historya (yes/no) | 8.639 (3.270) | ||
| Max exercise SBP (mmHg) | 0.172 (0.041) | 0.176 (0.035) | <0.001 |
| Arm/ankle difference (mmHg) | −0.037 (0.097) | ||
| Ratio arch/diaphragm | −5.039 (8.251) | ||
| Ratio anastomosis/diaphragm | −14.967 (4.873) | −16.614 (3.975) | <0.001 |
| Constant | 97.199 (9.425) |
| Explanatory variable | Univariate B (SE) | Stepwise multivariable B (SE) | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.881 (0.324) | 0.892 (0.261) | 0.001 |
| Age (years) | 0.322 (0.119) | ||
| Age at repair (years) | 0.303 (0.170) | ||
| Gender | 1.780 (2.280) | ||
| Hypertension historya (yes/no) | 8.639 (3.270) | ||
| Max exercise SBP (mmHg) | 0.172 (0.041) | 0.176 (0.035) | <0.001 |
| Arm/ankle difference (mmHg) | −0.037 (0.097) | ||
| Ratio arch/diaphragm | −5.039 (8.251) | ||
| Ratio anastomosis/diaphragm | −14.967 (4.873) | −16.614 (3.975) | <0.001 |
| Constant | 97.199 (9.425) |
The criterion for entry of variables in the stepwise multivariable regression analysis was set at 0.05 and removal at 0.10. The adjusted R2 of the stepwise multivariable regression model was 0.407.
B, regression coefficient; SE, standard error; Max, maximal; SBP, systolic blood pressure.
aHypertension based on patient's history.
Univariate and stepwise multivariable regression analyses of mean daytime systolic blood pressure in 73 post-coarctectomy patients with no, or mild, residual aortic stenosis
| Explanatory variable | Univariate B (SE) | Stepwise multivariable B (SE) | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.881 (0.324) | 0.892 (0.261) | 0.001 |
| Age (years) | 0.322 (0.119) | ||
| Age at repair (years) | 0.303 (0.170) | ||
| Gender | 1.780 (2.280) | ||
| Hypertension historya (yes/no) | 8.639 (3.270) | ||
| Max exercise SBP (mmHg) | 0.172 (0.041) | 0.176 (0.035) | <0.001 |
| Arm/ankle difference (mmHg) | −0.037 (0.097) | ||
| Ratio arch/diaphragm | −5.039 (8.251) | ||
| Ratio anastomosis/diaphragm | −14.967 (4.873) | −16.614 (3.975) | <0.001 |
| Constant | 97.199 (9.425) |
| Explanatory variable | Univariate B (SE) | Stepwise multivariable B (SE) | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.881 (0.324) | 0.892 (0.261) | 0.001 |
| Age (years) | 0.322 (0.119) | ||
| Age at repair (years) | 0.303 (0.170) | ||
| Gender | 1.780 (2.280) | ||
| Hypertension historya (yes/no) | 8.639 (3.270) | ||
| Max exercise SBP (mmHg) | 0.172 (0.041) | 0.176 (0.035) | <0.001 |
| Arm/ankle difference (mmHg) | −0.037 (0.097) | ||
| Ratio arch/diaphragm | −5.039 (8.251) | ||
| Ratio anastomosis/diaphragm | −14.967 (4.873) | −16.614 (3.975) | <0.001 |
| Constant | 97.199 (9.425) |
The criterion for entry of variables in the stepwise multivariable regression analysis was set at 0.05 and removal at 0.10. The adjusted R2 of the stepwise multivariable regression model was 0.407.
B, regression coefficient; SE, standard error; Max, maximal; SBP, systolic blood pressure.
aHypertension based on patient's history.
Univariate and stepwise multivariable regression analyses of common carotid IMT in 73 post-coarctectomy patients with no, or mild, residual aortic stenosis
| Explanatory variable | Univariate B (SE) | Stepwise multivariable B (SE) | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.0057 (0.004) | ||
| Age (years) | 0.0069 (0.001) | 0.0064 (0.001) | <0.001 |
| Age at repair (years) | 0.0063 (0.002) | ||
| Gender | 0.0049 (0.028) | ||
| Hypertension historya (yes/no) | 0.1230 (0.040) | ||
| Mean daytime SBP day (mmHg) | 0.0039 (0.001) | ||
| Max exercise SBP (mmHg) | 0.0007 (0.001) | ||
| Cholesterol (mmol/L) | 0.0012 (0.007) | ||
| Smoking (yes/no) | 0.0500 (0.030) | ||
| Arm/ankle difference (mmHg) | 0.0014 (0.001) | ||
| Ratio arch/diaphragm | −0.2002 (0.102) | ||
| Ratio anastomosis/diaphragm | −0.1660 (0.061) | −0.122 (0.054) | 0.027 |
| Constant | 0.543 (0.072) |
| Explanatory variable | Univariate B (SE) | Stepwise multivariable B (SE) | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.0057 (0.004) | ||
| Age (years) | 0.0069 (0.001) | 0.0064 (0.001) | <0.001 |
| Age at repair (years) | 0.0063 (0.002) | ||
| Gender | 0.0049 (0.028) | ||
| Hypertension historya (yes/no) | 0.1230 (0.040) | ||
| Mean daytime SBP day (mmHg) | 0.0039 (0.001) | ||
| Max exercise SBP (mmHg) | 0.0007 (0.001) | ||
| Cholesterol (mmol/L) | 0.0012 (0.007) | ||
| Smoking (yes/no) | 0.0500 (0.030) | ||
| Arm/ankle difference (mmHg) | 0.0014 (0.001) | ||
| Ratio arch/diaphragm | −0.2002 (0.102) | ||
| Ratio anastomosis/diaphragm | −0.1660 (0.061) | −0.122 (0.054) | 0.027 |
| Constant | 0.543 (0.072) |
The criterion for entry of variables in the stepwise multivariable regression analysis was set at 0.05 and removal at 0.10. The adjusted R2 of the stepwise multivariable regression model was 0.306.
B, regression co-efficient; SE, standard error; SBP, systolic blood pressure; Max, maximal.
aHypertension based on patient's history.
Univariate and stepwise multivariable regression analyses of common carotid IMT in 73 post-coarctectomy patients with no, or mild, residual aortic stenosis
| Explanatory variable | Univariate B (SE) | Stepwise multivariable B (SE) | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.0057 (0.004) | ||
| Age (years) | 0.0069 (0.001) | 0.0064 (0.001) | <0.001 |
| Age at repair (years) | 0.0063 (0.002) | ||
| Gender | 0.0049 (0.028) | ||
| Hypertension historya (yes/no) | 0.1230 (0.040) | ||
| Mean daytime SBP day (mmHg) | 0.0039 (0.001) | ||
| Max exercise SBP (mmHg) | 0.0007 (0.001) | ||
| Cholesterol (mmol/L) | 0.0012 (0.007) | ||
| Smoking (yes/no) | 0.0500 (0.030) | ||
| Arm/ankle difference (mmHg) | 0.0014 (0.001) | ||
| Ratio arch/diaphragm | −0.2002 (0.102) | ||
| Ratio anastomosis/diaphragm | −0.1660 (0.061) | −0.122 (0.054) | 0.027 |
| Constant | 0.543 (0.072) |
| Explanatory variable | Univariate B (SE) | Stepwise multivariable B (SE) | P-value |
|---|---|---|---|
| BMI (kg/m2) | 0.0057 (0.004) | ||
| Age (years) | 0.0069 (0.001) | 0.0064 (0.001) | <0.001 |
| Age at repair (years) | 0.0063 (0.002) | ||
| Gender | 0.0049 (0.028) | ||
| Hypertension historya (yes/no) | 0.1230 (0.040) | ||
| Mean daytime SBP day (mmHg) | 0.0039 (0.001) | ||
| Max exercise SBP (mmHg) | 0.0007 (0.001) | ||
| Cholesterol (mmol/L) | 0.0012 (0.007) | ||
| Smoking (yes/no) | 0.0500 (0.030) | ||
| Arm/ankle difference (mmHg) | 0.0014 (0.001) | ||
| Ratio arch/diaphragm | −0.2002 (0.102) | ||
| Ratio anastomosis/diaphragm | −0.1660 (0.061) | −0.122 (0.054) | 0.027 |
| Constant | 0.543 (0.072) |
The criterion for entry of variables in the stepwise multivariable regression analysis was set at 0.05 and removal at 0.10. The adjusted R2 of the stepwise multivariable regression model was 0.306.
B, regression co-efficient; SE, standard error; SBP, systolic blood pressure; Max, maximal.
aHypertension based on patient's history.
References
Therrien J, Warnes C, Daliento L et al. Canadian Cardiovascular Society Consensus Conference 2001 update: recommendations for the management of adults with congenital heart disease part III.
TheTask Force of the management of grown up congenital heart disease of the European Society of Cardiology. Management of grown up congenital heart disease.
Rosenthal E. Stent implantation for aortic coarctation: the treatment of choice in adults?
Staessen JA, Beilin L, Parati G et al. Task force IV: Clinical use of ambulatory blood pressure monitoring. Participants of the 1999 Consensus Conference on Blood Pressure Monitoring.
Staessen JA, Thijs L, Fagard RH et al. for the Systolic Hypertension in Europe Trial Investigators. Predicting cardiovascular risk using conventional and ambulatory blood pressure in older patients with systolic hypertension.
Kanters SD, Algra A, van Leeuwen MS et al. Reproducibility of in vivo carotid intima-media thickness measurements: a review.
Bots ML, Grobbee DE. Intima-media thickness as a surrogate marker for generalised atherosclerosis.
Bots ML, Dijk JM, Oren A et al. Carotid intima-media thickness, arterial stiffness and risk of cardiovascular disease: current evidence.
National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report.
Van Dam MJ, De Groot E, Clee SM et al. Association between increased arterial-wall thickness and impairment in ABCA1-driven cholesterol efflux: an observational study.
Kjeldsen SE, Mundal R, Sandvik L et al. Supine and exercise systolic blood pressure predict cardiovascular death in middle-aged men.
Vriend JW, van Montfrans GA, Romkes HH et al. Relation between exercise-induced hypertension and sustained hypertension in adult patients after successful repair of aortic coarctation.
Bogaert J, Gewillig M, Rademakers F et al. Transverse arch hypoplasia predisposes to aneurysm formation at the repair site after patch angioplasty for coarctation of the aorta.
Benjami Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing.
Sauerbrei W, Schumacher M. A bootstrap resampling procedure for model building: application to the Cox regression model.
Denarie N, Gariepy J, Chironi G et al. Distribution of ultrasonographically-assessed dimensions of common carotid arteries in healthy adults of both sexes.
Shaddy RE, Boucek MM, Sturtevant JE et al. Comparison of angioplasty and surgery for unoperated coarctation of the aorta.
Siblini G, Rao PS, Nouri S et al. Long-term follow-up results of balloon angioplasty of postoperative aortic recoarctation.
Fawzy ME, Sivanandam V, Galal O et al. One- to ten-year follow-up results of balloon angioplasty of native coarctation of the aorta in adolescents and adults.
Therrien J, Thorne SA, Wright A et al. Repaired coarctation: a “cost-effective” approach to identify complications in adults.
Toro-Salazar OH, Steinberger J, Thomas W et al. Long-term follow-up of patients after coarctation of the aorta repair.
Cohen M, Fuster V, Steele PM et al. Coarctation of the aorta. Long-term follow-up and prediction of outcome after surgical correction.
Sehested J, Baandrup U, Mikkelsen E. Different reactivity and structure of the prestenotic and poststenotic aorta in human coarctation.
Gidding SS, Rocchini AP, Moorehead C et al. Increased forearm vascular reactivity in patients with hypertension after repair of aortic coarctation.
Gardiner HM, Celermajer DS, Sorensen KE et al. Arterial reactivity is significantly impaired in normotensive young adults after successful repair of aortic coarctation in childhood.
De Divitiis M, Pilla C, Kattenhorn M et al. Vascular dysfunction after repair of coarctation of the aorta. Impact of early surgery.
Guenthard J, Zumsteg U, Wyler F. Arm-leg pressure gradients on late follow-up after coarctation repair. Possible causes and implications.
Beekman RH, Katz BP, Moorehead-Steffens C et al. Altered baro-receptor function in children with systolic hypertension after coarctation repair.
Simsolo R, Grunfeld B, Gimenez M et al. Long-term systemic hypertension in children after successful repair of coarctation of the aorta.
Weber HS, Cyran SE, Grzeszczak M et al. Discrepancies in aortic growth explain aortic arch gradients during exercise.
Brouwer RMHJ, Erasmus M, Ebels T et al. Influence of age on survival, late hypertension, and recoarctation in elective aortic coarctation repair. Including long-term results after elective aortic coarctation repair with a follow-up from 25 to 44 years.
Daniels SR. Repair of coarctation of the aorta and hypertension: does age matter?
de Divitiis M, Pilla C, Kattenhorn M et al. Ambulatory blood pressure, left ventricular mass, and conduit artery function late after successful repair of aortic coarctation.
Niwa K, Perloff JK, Bhuta SM et al. Structural abnormalities of great arterial walls in congenital heart disease: light and electron microscopic analyses.
Warnes CA. Bicuspid aortic valve and coarctation: two villains part of a diffuse problem.
Franklin SS, Gustin W IV, Wong ND et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study.
Ghiadoni L, Taddei S, Virdis A et al. Endothelial function and common carotid artery wall thickening in patients with essential hypertension.


{kind=link}
{kind=link}
{kind=link}
{kind=link}