Article Text

Abstract
Objective To assess the relationship between 6-min walk test (6MWT) distance and variables of cardiopulmonary exercise testing (CPET) in children with pulmonary arterial hypertension (PAH).
Design Retrospective study.
Setting Tertiary hospital.
Patients Children with PAH.
Interventions CPETs and 6MWTs.
Main outcome measures Correlations between variables of CPET and 6MWT distance.
Results 41 exercise studies were included: 15 in children with idiopathic PAH (mean age 13.0±3.0 years; 9 female), 18 in children with PAH associated with congenital heart disease (age 14.8±2.8 years; 7 female) and 8 in children with Eisenmenger syndrome (age 11.8±2.9 years; 4 female). All underwent a CPET and 6MWT. Peak oxygen consumption (pVO2) and 6MWT distance were reduced to 31.5±12.2% and 47.7±16.7% of the predicted value, respectively (p<0.0001 for both). pVO2 and oxygen consumption at anaerobic threshold showed correlation with 6MWT distance (r=0.49; p=0.001 and r=0.40, p=0.01, respectively), while an inverse correlation was found between measures of ventilatory efficiency (eg, VE/VCO2) at anaerobic threshold and 6MWT distance (r=−0.43; p=0.005). There was a significant linear relationship between pVO2 and 6MWT up to a distance of 300 m, with the 6MWT distance accounting for 71% of the variation in pVO2 but there was hardly any association when the 6MWT distance was >300 m.
Conclusions The 6MWT reflects maximal exercise capacity in patients with a 6MWT distance below 300 m. A CPET should therefore be considered as a complimentary test in children with an exercise tolerance above this threshold. These findings may have implications for assessing response to drug therapy and for consideration as an end point in future PAH trials.
Statistics from Altmetric.com
The 6-min walk test (6MWT) is the distance a person can walk at a constant, uninterrupted, unhurried pace in 6 min. It represents a simple and cost-effective method of assessing exercise capacity and is used routinely to assess patients with cardiovascular or pulmonary disease.1 It has been demonstrated to be an independent predictor of morbidity and mortality in adult patients with heart failure, pulmonary disease and idiopathic pulmonary hypertension.2,–,4 At many centres it is used for longitudinal assessment of patients with chronic disease, especially to monitor response to treatment and to guide therapy.5
What is already known on this topic
▶ Patients with pulmonary arterial hypertension (PAH) have markedly depressed exercise capacity.
▶ In adults, both, 6-min walk test (6MWT) distance and peak oxygen consumption (pVO2) predict outcome.
What this study adds
▶ Performing 6MWT and cardiopulmonary exercise testing (CPET) in children with PAH is feasible and safe.
▶ 6MWT reflects maximal exercise capacity in PAH children with a 6MWT distance of less than 300 m or a pVO2 of less than 20 ml/kg/min, while it represents submaximal effort in less impaired children. This study provides guidance on when a CPET should be considered as a complimentary test in children with PAH.
Cardiopulmonary exercise testing (CPET) with metabolic monitoring is regarded by many to be the gold-standard modality to assess exercise capacity.6 Unlike the 6MWT, CPET represents a maximal exercise test and provides additional measures of exercise tolerance and disease severity such as peak oxygen consumption (pVO2), oxygen consumption at anaerobic threshold (VO2AT) and ventilatory efficiency (VE/VCO2). Despite its apparent advantages and the fact that pVO2 predicts prognosis in adult patients with pulmonary arterial hypertension (PAH),7 the use of CPET as an end point for prospective clinical trials in patients with pulmonary hypertension is problematic. The alleged disadvantages of CPET as compared to the 6MWT in this setting have been discussed in detail elsewhere.8
A recent study has demonstrated that CPET can be performed safely in paediatric patients with pulmonary hypertension;9 however, little is known about correlations between 6MWT distance and variables of CPET in children with PAH.
Patients and methods
Forty-one consecutive exercise studies were included in this analysis (patients' mean age±SD 13.5±3.0 years, table 1): 15 exercise tests in children with idiopathic PAH (IPAH) (mean age 13.0±3.0 years; 9 female), 18 in children with PAH associated with congenital heart disease (mean age 14.8±2.8 years; 7 female; unrepaired heart defects n=3, postrepair PAH 15) and 8 in children with the Eisenmenger syndrome (mean age 11.8±2.9 years; 4 female). Of those with IPAH, 35% were on monotherapy and 65% were on combination therapy. Children with congenital heart disease (without the Eisenmenger syndrome) were treated with bosentan monotherapy (40%) or combination therapy (30%). Of those with the Eisenmenger syndrome, four children were on either bosentan or sildenafil monotherapy and one other received both drugs. The patients included in the current study were consecutive children with PAH seen in our centre who were deemed developmentally able and willing to perform a CPET and a 6MWT. All children underwent both tests without complications. CPET was performed on a mechanically braked bicycle ergometer (Ergoline 900, Germany) with respiratory gas exchange analysis (Medgraphics, St Paul, Minnesota, USA). A ramp protocol comprising an initial period of loadless cycling to permit equilibration was used. A period of active recovery (slow cycling under minimal friction load) was commenced after maximal exertion. Heart rate, blood pressure and oxygen saturation were monitored in all children for the duration of the test. Peak oxygen uptake (pVO2) and anaerobic threshold were derived from respiratory gas analysis during maximal exercise testing. Anaerobic threshold was determined by use of the modified V-slope method. Peak heart rate, blood pressure and workload achieved were recorded. Predicted values for peak oxygen uptake were calculated according to published data for healthy children.10
Patient demographics and baseline clinical parameters
The 6MWT was conducted using a lap of 30–50 m in length on flat, hard ground, according to the American Thoracic Society guidelines.11 The total distance walked in 6 min was measured. Oxygen saturation and heart rate were measured before the start of the walk, after every minute during the test and during the recovery period at 1 and 3 min. A portable pulse oxymeter (Pulsox-3iA, Minolta, Milton Keynes, UK) attached to the child's wrist and a finger was used to assess the transcutaneous oxygen saturation. All children received the same instructions before undertaking the walk test. The children were asked to walk up and down the measured lap at their best pace but not to run or race. Predicted values for 6MWT distance in boys and girls were calculated based on gender, age and height according to published data for healthy Caucasian children and adolescents.12 The study was approved by the local ethics committee. All patients underwent exercise testing as part of their clinical follow-up and provided informed consent before exercise testing.
Statistical analysis
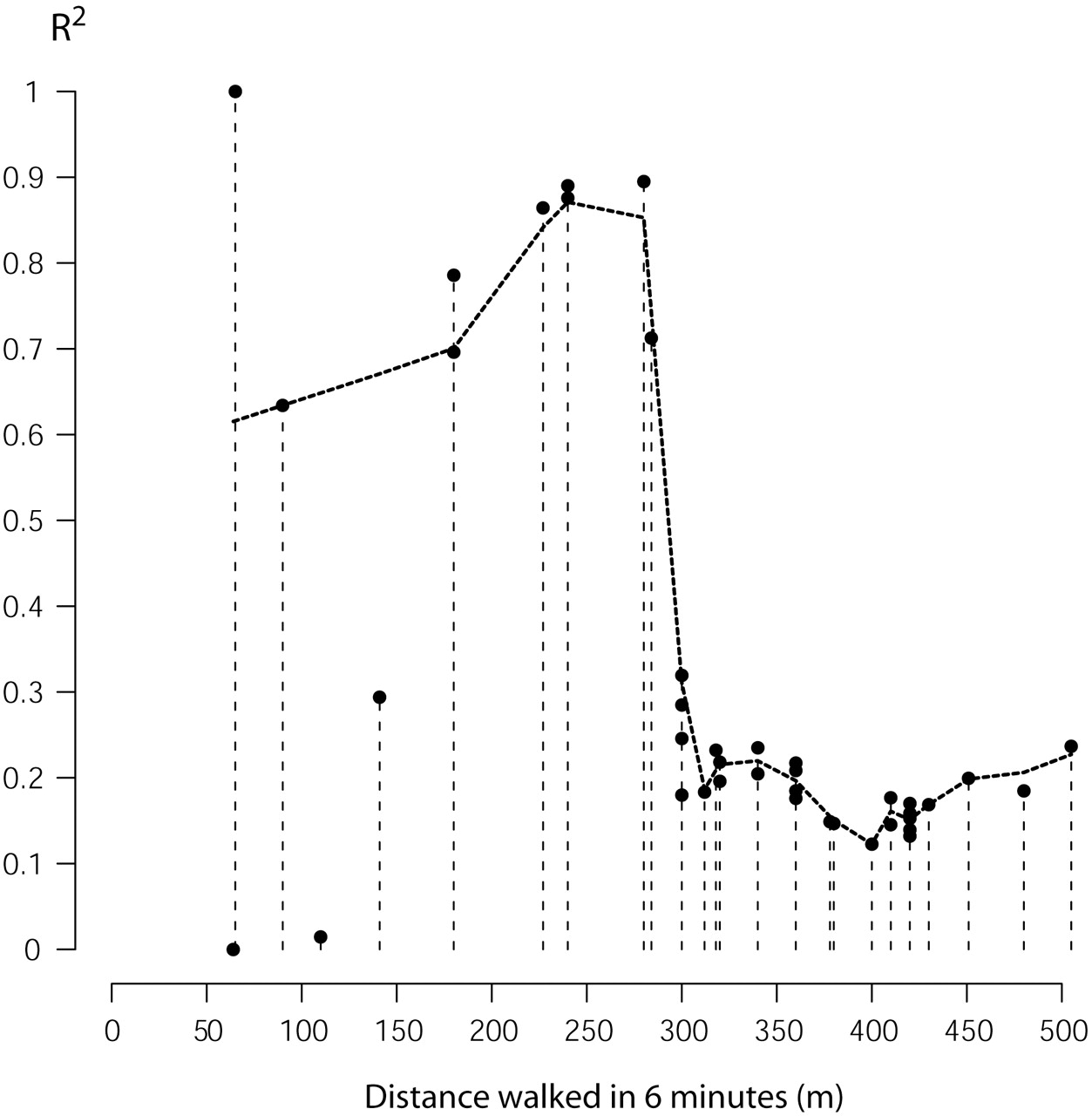
Unless stated otherwise all values are presented as mean±SD and comparisons between groups were made using unpaired Student's t test after ascertaining that variables were normally distribution as indicated by the D'Agostino–Pearson test. Relationships between variables of 6MWT and CPET were studied using Pearson's correlation coefficient (after testing for normal distribution). To explore the relationship between variables of 6MWT distance and CPET in scatterplots the locally weighted scatterplot smoother (Lowess) technique using a local linear polynomial fit to provide a smooth line describing the association between 6MWT distance and pVO2 was used.13 14 In addition, a parametric model using fractional polynomials was fitted to the data using Generalized Additive Models for Location Scale and Shape in R as described by Rigby and Stasinopoulos.15 To describe the change in heart rate and oxygen saturation during 6MWT a linear mixed effects model with higher-than-linear (a+x+x3/2) terms to describe the observed shapes and to take into account the repeated measurements structure of the data was fitted using the NLME package in R.16 To study the optimal cut-off value for 6MWT distance in predicting pVO2, we calculated R2-values for the linear correlation between 6MWT distance and pVO2 for a subset of 6MWT distances (lowest value to increasing cut-off) and plotted the R2-values for different cut-off values of 6MWT distance.
Statistical analyses were performed using the MedCalc V.11.1.1.0 (MedCalc Software) and R (V.2.10.1) statistical package.17
Results
Reduced exercise capacity in children with PAH
Children with pulmonary hypertension had a reduced exercise capacity as judged by CPET and 6MWT. pVO2 was reduced to 31.5±12.2% of the predicted value (p<0.0001) (figure 1). The 6MWT distance was also reduced to 47.7±16.7% of the predicted value (p<0.0001). In fact, none of the studied children achieved 80% of the 6MWT value predicted for healthy children. Interestingly, no significant difference in 6MWT distance could be found between children in WHO class 2 or 3 (325±109 vs 304±132 m, respectively; p=0.67). Nor was there a significant difference in pVO2 between WHO class 2 or 3 (22.5±6.5 vs 20.5±6.4 ml/kg/min in WHO class 2 and 3, respectively; p=0.39). These observations illustrate the limitations of assessing exercise tolerance based on patients' subjective physical capacity. The 6MWT distance was lowest in the Eisenmenger population (255±132 m; 39.2±21.1% of the predicted 6MWT distance) compared to patients with IPAH (332±110 m; 50.2±16.0% of the predicted 6MWT distance) and PAH associated with congenital heart disease (336±102 m, 49.4±14.7% of the predicted 6MWT distance) but the differences were not statistically significant.

Predicted and measured values for 6-min walk test distance and peak oxygen consumption in children with pulmonary arterial hypertension. Markers indicate 95% CI for the mean. Comparisons between groups were performed using Mann–Whitney tests. Reference values were calculated according to published data.10 12
Similarly, patients with the Eisenmenger syndrome (16.8±5.8 ml/kg/min) had a significantly lower value for pVO2 compared to patients with PAH associated with congenital heart disease (23.3±6.7 ml/kg/min, p=0.03) and the mean value was lower, although not statistically significant, than in those with IPAH (20.2±5.6 ml/kg/min, p=0.12). The percentage of predicted pVO2 was also lower in the Eisenmenger group (24.3±9.7%) compared to patients with either PAH associated with congenital heart disease (33.6±12.2%, p=0.07) or IPAH (32.8±12.6 %, p=0.12).
Correlations between variables of CPET and 6MWT
Both pVO2 and oxygen consumption at anaerobic threshold (VO2AT) showed correlation with the 6MWT distance (r=0.49; p=0.001 and r=0.40, p=0.01, respectively), and an inverse correlation was found between VE/VCO2 at anaerobic threshold and the 6MWT distance (r=−0.43; p=0.005).
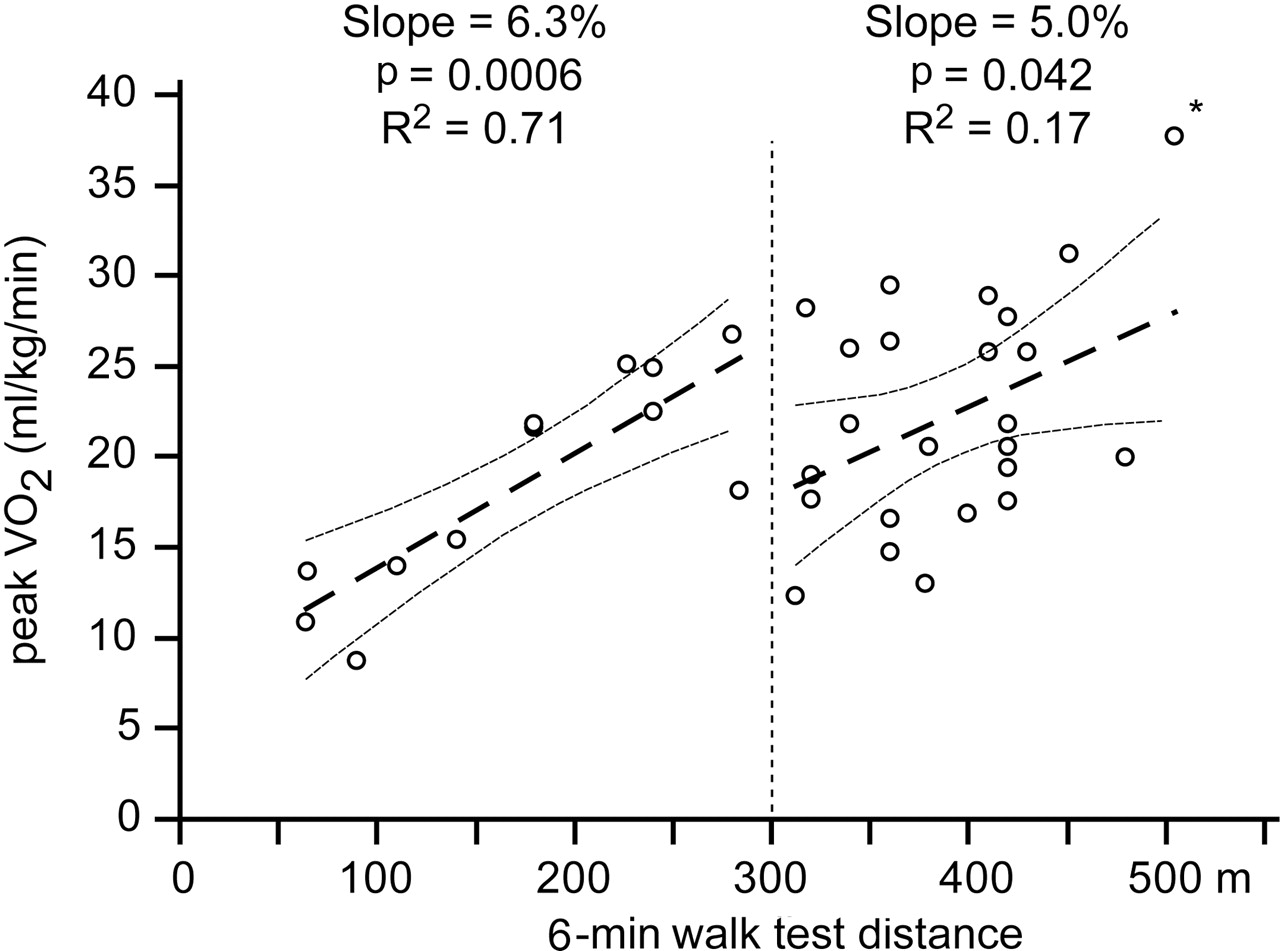
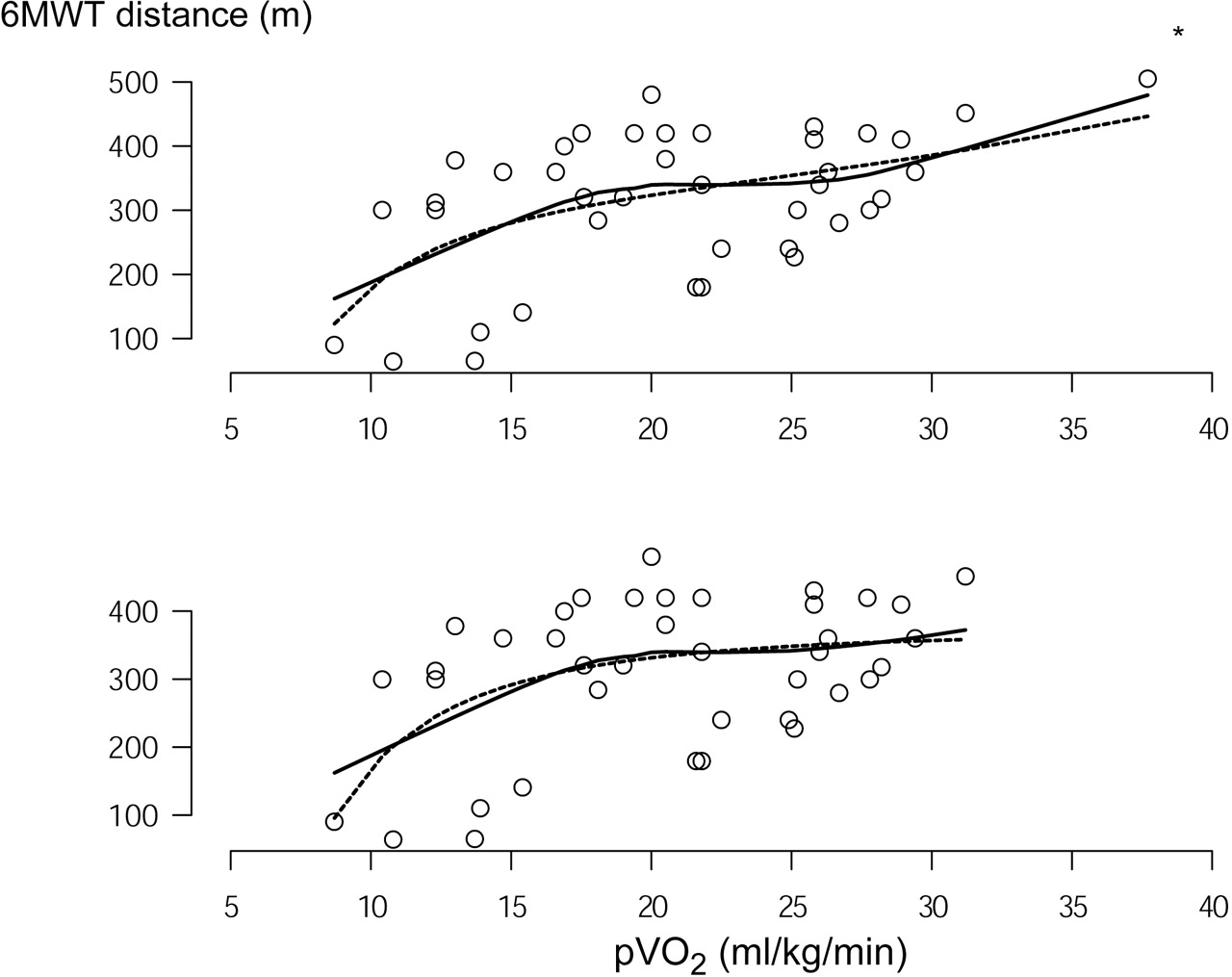
However, when the relationship between the 6MWT distance and pVO2 was investigated further using locally weighted polynomial regression (lowess), it became apparent that a linear correlation between 6MWT distance and pVO2 existed only at low levels of exercise capacity. As illustrated in figure 2, there appeared to be a close to linear association between 6MWT distance and pVO2 up to a 6MWT distance of approximately 300 m or pVO2 of 20 ml/kg/min, respectively. Visually, there appeared to be a ‘ceiling-effect’ of 6MWT distance for higher values of pVO2.

Locally weighted polynomial regression (lowess—solid line) with and without exclusion of an outlier (*) showing a close to linear association between 6-min walk test (6MWT) distance and peak oxygen consumption (pVO2) up to a 6MWT distance of approximately 300 m or pVO2 of 20 ml/kg/min with a plateau phenomenon thereafter. In addition, a parametric model using fractional polynomials was fitted to the data (dotted line) using Generalized Additive Models for Location Scale and Shape in R as described by Rigby and Stasinopoulos.15
Based on visual inspection of the relationship between pVO2 and 6MWT, as well as based on R2 maximisation (figure 3) a cut-off value of 300 m was chosen to further investigate the relationship between pVO2 and 6MWT below and above this value. This cut-off value is in agreement with data published in adult heart failure patients, dividing patients into those with maximal and submaximal exercise and identifying patients with adverse outcomes.18 Using this cut-off value confirmed a significant relationship between pVO2 and 6MWT distance up to a distance of 300 m, indicating that the 6MWT distance accounted for 71% of the variation in pVO2 when the 6MWT distance was <300 m, while there was hardly any association between 6MWT distance and pVO2 at higher levels of 6MWT distance (figure 4). In fact, when one apparent outlier (the child with the highest combination of 6MWT distance and pVO2 and the highest residual value on correlation analysis—marked with * in figures 2 and 4) was excluded, no significant association between 6MWT distance and pVO2 was found for patients with a 6MWT distance >300 m (p=0.30).

Plot of calculated R2-values for the linear correlation between 6-min walk test (6MWT) distance and peak oxygen consumption (pVO2) for a subset of 6MWT distances (lowest value to increasing cut-off) against different cut-off values of 6MWT distance. The plot supports the notion that there is a relevant reduction in the percentage of the variation in pVO2 explained by 6MWT distance around a cut-off value of 300 m, which is in agreement with the impression on visual inspection of the data. The dotted lines represents the result of a locally weighted polynomial regression (lowess).
Linear regression comparing the association between 6-min walk test (6MWT) distance and peak oxygen consumption for patients with a 6MWT distance below and above 300 m separately.
Similar differences were found for VO2AT (p=0.046 [R2=0.34] for 6MWT distance <300 m and p=0.20 [R2=0.07] for 6MWT distance >300 m) and for VE/VCO2 at anaerobic threshold (p=0.02 [R2=0.41] for 6MWT distance <300 m and p=0.90 [R2<0.01] for 6MWT distance >300 m).
Does 6MWT represent a maximal exercise test in patients with PAH?
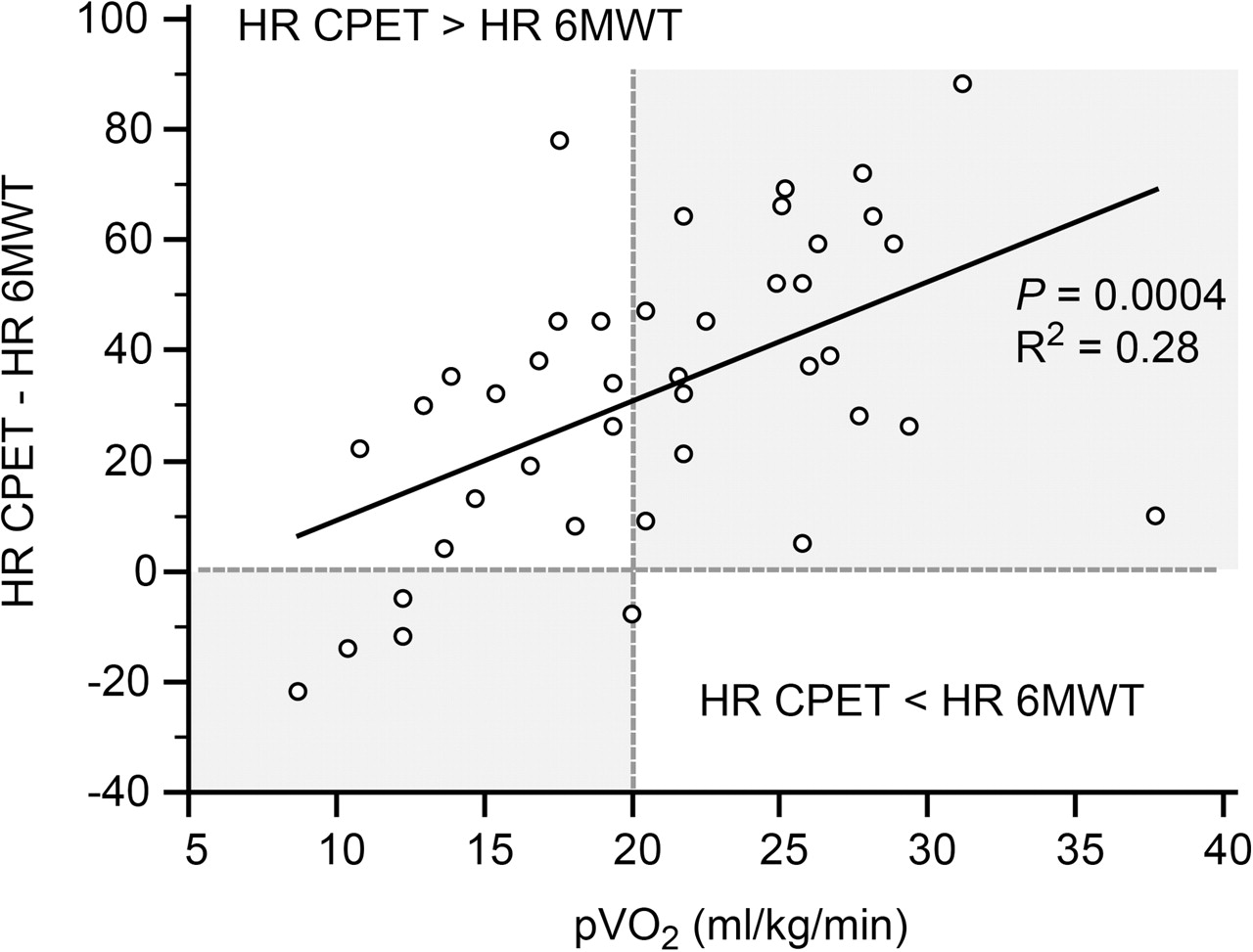
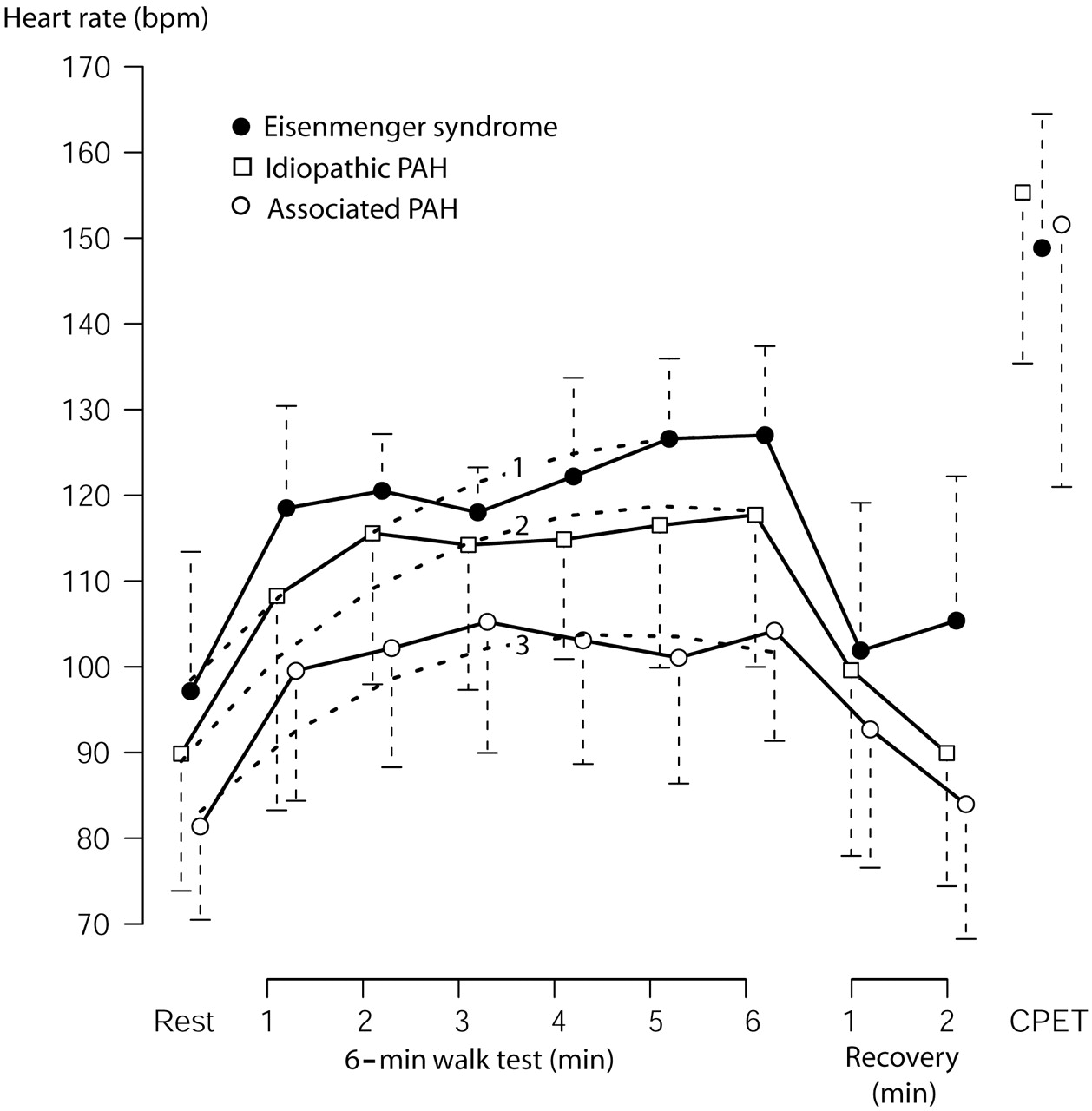
To further investigate whether the 6MWT distance represents a measure of maximal exercise capacity in children with PAH, we compared maximal heart rate during CPET and 6MWT. As illustrated in figure 5, maximal heart rate during CPET was significantly higher in the entire patient cohort (152±24 vs 120±17/min; p<0.0001), and in all three individual patient subgroups (p value between 0.0002 and 0.01) compared to maximal heart rate during 6MWT, supporting the notion that 6MWT represents a submaximal exercise test. Furthermore, within the Eisenmenger population the minimal oxygen saturation recorded during exercise testing was lower during CPET compared to 6MWT, although there was little difference in minimal oxygen saturation between the two tests in children with IPAH and other congenital heart disease associated with pulmonary hypertension (figure 6). To further investigate the relationship between maximal heart rate during CPET and 6MWT, we calculated the difference between these two variables for each individual patient. Correlating pVO2 with the heart rate difference between CPET and 6MWT revealed a close correlation between these variables as shown in figure 5 (p=0.0004; r=0.53). While some patients with a pVO2<20 ml/kg/min had a similar or even lower maximal heart rate during CPET compared to 6MWT, all children with a pVO2>20 ml/kg/min exhibited higher maximal heart rates during CPET compared to 6MWT, which is consistent with the notion that the 6MWT distance represents a maximal exercise test in sick children while it is a marker of submaximal exercise capacity in less compromised patients (figure 7).
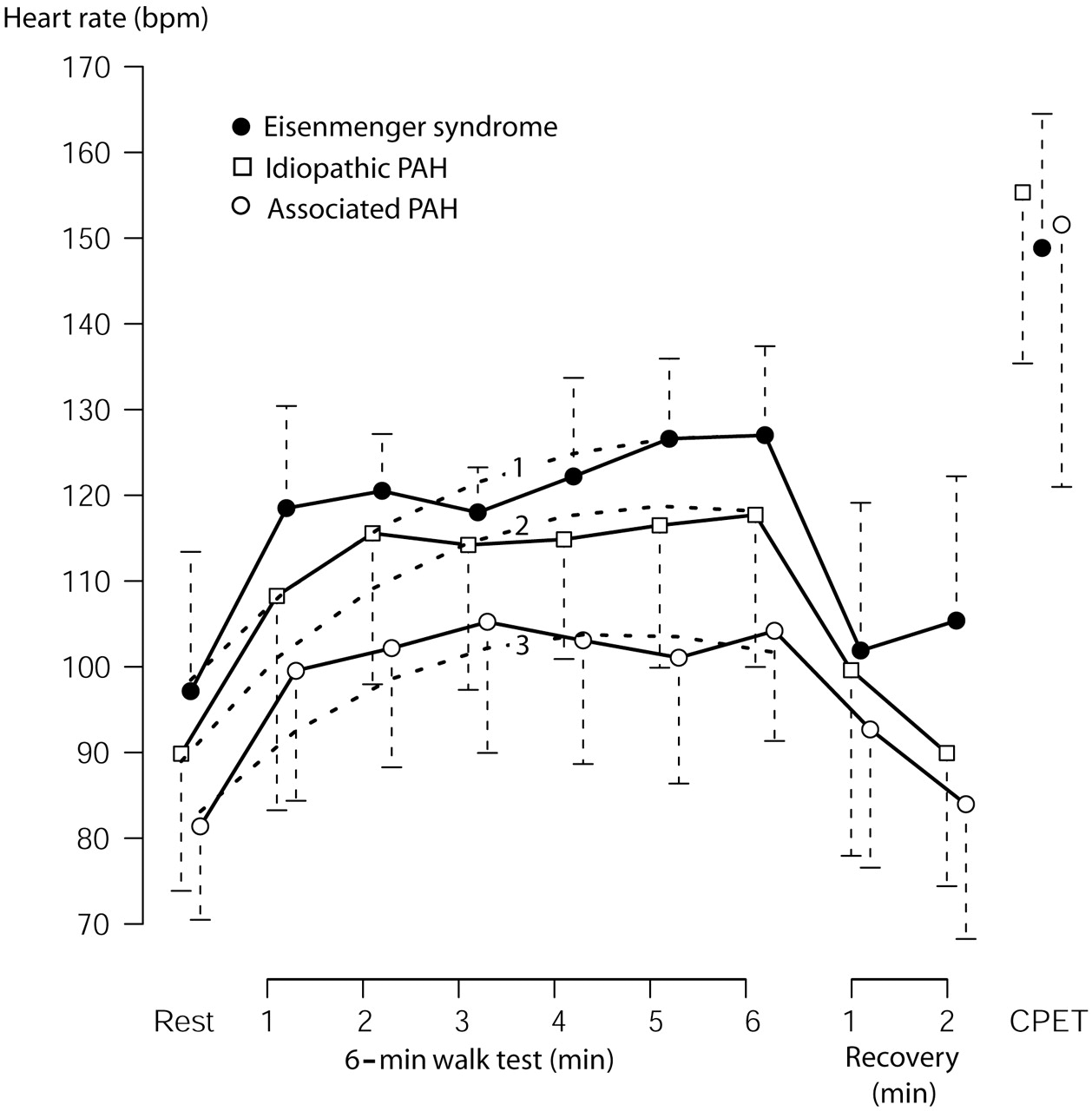
Heart rate (HR) profile during 6-min walk test (6MWT) and maximal HR during cardiopulmonary exercise testing (CPET) in children with idiopathic pulmonary arterial hypertension (PAH), pulmonary hypertension associated with congenital heart disease (‘Associated PAH’) and Eisenmenger syndrome. Symbols and error bars indicate mean±SD. To describe the change in heart rate during 6MWT, a linear mixed effects model with higher-than-linear (a+x+x3/2) terms to account for the observed shapes and the repeated measurements structure of the data was fitted using the NLME package in R (dotted lines)16: curve 1: HR=95.7+15.8*t–4.3*t1.5, p<0.002 for all coefficients; curve 2: HR=87.3+17.9*t–5.2*t1.5, p<0.0001 for all coefficients; curve 3: HR=79.2+15.9*t–4.9*t1.5, p<0.0001 for all coefficients. t=time in minutes.

Transcutaneous oxygen saturation (SO2) in children with idiopathic pulmonary arterial hypertension (PAH), pulmonary hypertension associated with congenital heart disease (‘Associated PAH’) and the Eisenmenger syndrome during the 6-min walk test (6MWT) and cardiopulmonary exercise testing (CPET). Note that minimal transcutaneous oxygen saturation in Eisenmenger patients is lower during CPET compared to 6MWT. Symbols and error bars indicate mean±SD. To describe the change in SO2 during 6MWT, a linear mixed effects model with higher-than-linear (a+x+x3/2) terms to account for the observed shapes and the repeated measurements structure of the data was fitted using the NLME package in R (dotted lines)16: curve 1: SO2= 95.8–4.5*t+1.4*t1.5, p<0.01 for all coefficients; curve 2: SO2=92.4–4.0*t+1.4*t1.5, p<0.0001 for all coefficients; curve 3: SO2= 76.5–14.9*t+4.9*t1.5, p<0.0001 for all coefficients. t=time in minutes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatterplot exploring the relationship between the difference in maximal heart rate (HR) during cardiopulmonary exercise testing (CPET) and 6-min walk test (6MWT). The plot illustrates that while some patients with a peak oxygen consumption (pVO2) below 20 ml/kg/min had similar or even lower heart rates during CPET compared to 6MWT (left lower quadrant), patients with a pVO2>20 ml/kg/min had consistently higher heart rates during CPET compared to 6MWT and the difference in heart rate increased with increasing exercise tolerance (right upper quadrant).
Discussion
This study shows that children with PAH have markedly depressed exercise capacity. In children with a 6MWT distance below ∼300 m or a pVO2 below ∼20 ml/kg/min a close correlation was found between measures of exercise capacity derived from CPET and the 6MWT distance. In contrast, there was a much weaker, if any, association between these assessments of exercise capacity in less compromised patients. Therefore, it appears that the 6MWT distance fails to reflect maximal exercise tolerance in less impaired children with PAH and that CPET may be a useful adjunct in the comprehensive assessment of patients with a 6MWT distance above 300 m.
pVO2 is an established and reliable measure of exercise intolerance and is widely employed in the assessment of patients with congenital heart disease and PAH.6 19 We found a significantly reduced pVO2 and 6MWT distance in children with PAH compared to reference values derived from healthy children of similar age.12 These findings are in agreement with those in similar studies carried out on adult patients with PAH.4 20,–,22 However, there is little data available on the 6MWT distance and especially on CPET in children with PAH. As a consequence, considerable controversy exists regarding the merits of performing CPET in these children. While 6MWT is easy to perform and can be repeated at low cost, CPET with metabolic monitoring requires expensive equipment, technical expertise and training of the subject. It does, however, provide additional objective measures of exercise capacity such as oxygen uptake and ventilatory efficiency, which can be regarded a surrogate variables of pulmonary blood flow.6 23 In addition, VO2 at anaerobic threshold and markers of ventilatory efficiency can be calculated based on CPET. A modest correlation between 6MWT distance and VE/VCO2 at anaerobic threshold—a parameter of ventilatory efficiency—was found in the current study. Recently, measures of ventilatory efficiency such as VE/VCO2 at anaerobic threshold or the VE/VCO2-slope have been found to be related to prognosis in various cardiovascular cohorts. Conceptually they are appealing due to their robustness and the fact that they are independent of patient effort. In fact, studies in patients with congenital heart disease and congestive heart failure have established that VE/VCO2-slope is superior to pVO2 in predicting prognosis.24 25 Whether these parameters relate to prognosis in children with PAH as they do in adults with PAH and without a patent foramen ovale7 remains to be established. In patients with right-to-left shunting at rest or during exercise the value of parameters of ventilatory efficiency may be limited. Parameters of ventilatory efficiency do not carry important prognostic information in cyanotic patients, such as patients with Eisenmenger syndrome, for reasons discussed in detail by Dimopoulos et al.24 However, in selected children with PAH, parameters of ventilatory efficiency may prove helpful in assessing disease severity, for assessing response to drug therapy and for consideration as potential end points in future PAH trials.
Remarkably, the correlation coefficient between 6MWT distance and pVO2 (0.49 in the current study) is almost identical with that published in a large cohort of adult patients who underwent exercise testing as part of a multicentre clinical trial evaluating sitaxsentan—an endothelin receptor antagonist (r=0.483).8 The authors suggested that this modest correlation was at least in part due to lack of standardisation of CPET and a different level of experience at centres participating in this drug trial. This study demonstrates that even when all tests are performed at a single institution using a standardised protocol, skilled technicians and properly calibrated CPET equipment the correlation between the 6MWT distance and pVO2 is only modest and that the 6MWT distance cannot be used as a surrogate for pVO2.
The heart rate recorded during 6MWT in the current study demonstrates that 6MWT represents submaximal effort in many children. Estimated peak heart rate during maximal exercise of children with an average age of 13 years would be approximately 195 bpm (220 bpm minus age).26 Thus, the peak heart rate in this study was approximately 60% of the normal predicted peak heart rate for age. In contrast, the maximal heart rate during CPET averaged 152 bpm, representing 78% of the predicted value. As illustrated in figure 5, heart rate increased early during 6MWT with a plateau after 1–3 min, which is consistent with the concept of a steady-state metabolism reached after this point in analogy to patients performing a submaximal test or a CPET below the anaerobic threshold.27
Clinical implications
Knowing how far a child with PAH can walk in 6 min is helpful in assessing the degree of exercise limitation, and in evaluating prognosis and response to medical therapy. Although changes in the 6MWT distance are routinely used as an end point in PAH clinical trials and provide valuable information when managing children with PAH, this study suggests that CPET should be considered as a complimentary test in less impaired children with PAH who have a 6MWT distance of more than 300 m, because the 6MWT distance appears to represent a submaximal test in these children. None of the patients included in the current study suffered any adverse events during CPET or 6MWT. This suggests that exercise testing is safe even in children with PAH, which is in agreement with previous studies in adult patients with congenital heart disease and pulmonary hypertension including patients with IPAH and Eisenmenger syndrome.19 24 Despite the fact that none of the patients in the current study experienced any relevant complications during exercise, we suggest that exercise tests in children with PAH should be supervised by a trained exercise physiologist and that a physician with experience in handling children with PAH should be present at all times. We operate a policy of carrying out regular 6MWTs from the age of approximately 4 years onwards. Initially these tests are performed to accustom the children with 6MWT. In our experience, most children can perform a 6MWT from the age of 5–6 years reliably, although other authors have recommended not to perform walk tests in children with PAH below the age of 7 years.28 CPETs are performed on a bicycle ergometer in our centre and this requires that children should have a minimum height of 140 cm. While some children cannot perform a CPET due to problems with coordination, it is our impression that most children with mild to moderate developmental disorders including Down's syndrome can reliably perform a 6MWT. While this study was performed in children with PAH it may have implications for a variety of paediatric conditions. 6MWT is used in children with neurologic conditions (such as cerebral palsy or spinal muscular atrophy),29 30 orthopaedic disorders (such as idiopathic scoliosis),31 haematologic diseases (such as sickle cell disease and haemophilia)32 33 and a variety of respiratory and cardiac conditions.34 35 As a consequence, the results of the current study may be of relevance for these patient cohorts as well. There appears to be no doubt that in healthy individuals 6MWT represents a submaximal exercise test, mainly reflecting the patient's ability to perform day-to-day activities. Roul and colleagues, investigating adult patients with heart failure, suggested that in highly compromised patients 6MWT may represent a maximal exercise test.18 As in the present paediatric study, the 6MWT distance in adults with heart failure correlated with pVO2 only when the 6MWT distance was less than 300 m. In addition, the 6MWT distance was predictive of survival in heart failure patients walking less than 300 m in 6 min. The present study establishes for the first time that pVO2 is closely related to the 6MWT distance in children with PAH who have a poor exercise capacity (ie, a 6MWT distance below ∼300 m or a pVO2 below ∼20 ml/kg/min). For higher values of 6MWT distance this association is weak or absent. Therefore, when assessing the effect of medical therapies on exercise capacity in children with higher exercise capacity a CPET should be the preferred exercise testing modality.
Study limitations
Predicted values for the 6MWT distance were derived from a study published recently by Geiger et al12 who used a measuring wheel to record the walking distance. This represents a slight modification from conventional practice. It is difficult to know whether and to what extent this would have influenced their results. Future studies will focus on studying exercise capacity in PAH of different aetiologies and attempt to correlate performance with outcome. This was a cross-sectional analysis and further longitudinal studies are required to assess whether serial CPET or 6MWT represent effective efficacy end points for pulmonary hypertension trials.
In conclusion, performing 6MWT and CPET in children with PAH is feasible and safe. 6MWT reflects maximal exercise capacity in PAH children with a 6MWT distance of less than 300 m or a pVO2 of less than 20 ml/kg/min. CPET should be considered as a complimentary test in children whose exercise tolerance is well above these thresholds.
Acknowledgments
The authors wish to thank very sincerely all the UK paediatric cardiologists and paediatricians who referred and helped care for these children as part of the UK Pulmonary Hypertension Service for Children.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Great Ormond Street Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.