Article Text

Abstract
The treatment of pulmonary hypertension (PH) secondary to bronchopulmonary dysplasia (BPD) in infants has evolved in recent years, improving both quality of life and survival for patients. One of the potential agents for this condition is sildenafil, a phosphodiesterase-V inhibitor with proven efficacy within the idiopathic PH population. However, only limited evidence exists for its use as either monotherapy or part of a combination approach towards the management of PH in BPD. This review summarises the evidence base for sildenafil alone and in combination with other recognised therapeutic agents for ameliorating paediatric PH in the presence of BPD. It also examines the suitability for current practice with the aim of clarifying regimens that produce improved patient outcomes. We conclude that sildenafil is both safe and effective in this utility. Doses should be started at 0.5 mg/kg every 8 h before titrating up towards 2 mg/kg every 6 h to effect reductions in pulmonary vascular resistance and arterial pressure. Evidence suggests that if continued until PH resolution, this improves survival from 61% to 81% at 12 months. Furthermore, there are also data suggesting that in treatment refractory PH cases, the addition of endothelin antagonists and prostacyclin analogues to sildenafil therapy can also be considered.
- Paediatric
- Respiratory
- pulmonary hypertension
- sildenafil
- bronchopulmonary dysplasia
Statistics from Altmetric.com
Introduction
Bronchopulmonary dysplasia (BPD), also known as chronic lung disease, most commonly affects premature neonates with respiratory distress syndrome requiring mechanical ventilation or oxygen therapy. However, it can also occur when there are few signs of underlying lung pathology.1 An estimated 13%–35% of preterm infants beyond 36 weeks postmenstrual age have BPD. Furthermore, the lack of knowledge regarding BPD's pathology and complications, coupled with no consensus on best treatment, means significant scope remains for improved therapy.2
One of the most important complications of BPD is pulmonary hypertension (PH).3 Sildenafil, a phosphodiesterase-V inhibitor (PDE-Vi), has proven efficacy in PH as monotherapy and in combination with other medications; however, data regarding its specific use in BPD-induced PH (BPD-PH) remain elusive. This review outlines the utility of sildenafil in this context given currently available evidence.
BPD and PH
The definition of BPD has been extensively modified since the initial description of Northway and coworkers in 1967.4 Historically, the most widely accepted consensus defines BPD as a need for oxygen therapy at 36 weeks postmenstrual age in an infant older than 28-days-old.5 More recently, a consensus workshop redefined BPD to include a severity grading system while taking into account differing postmenstrual ages, as in table 1.6 However, exactly how BPD should be defined remains unclear.
Criteria for diagnosing BPD6
Currently, BPD incidence is approximately 30% among children born less than 1000 g.7 Preterm infants with BPD are vulnerable to various cardiovascular sequelae including cor pulmonale, systemic hypertension and ventricular hypertrophy.8 It is of note that up to 37% of BPD cases are complicated by PH,9 although the reasons for this remain unclear but presumably linked to global hypoxia. BPD-PH is the most common cause of PH due to respiratory disorders (Group 3) and is found in approximately 5% of childhood PH.10
Earliest possible detection of BPD-PH is essential to facilitate prompt intervention and improved outcomes, especially regarding right heart failure. However, presentation can be indistinct from other respiratory conditions and therefore screening is necessary. Criteria for this have been suggested by other groups as outlined in figure 1,3 although screening in all small for gestational age neonates is unrealistic, particularly during current economic conditions.

Criteria for bronchopulmonary dysplasia-induced pulmonary hypertension (BPD-PH) screening according to Kheman et al.3
The gold-standard PH diagnosis is defined as mean pulmonary arterial pressure (pPA) ≥25 mm Hg at rest on cardiac catheterisation.11 However, this is invasive and therefore Doppler echocardiography, with a tricuspid valve regurgitant jet velocity more than or equal to 2.8m/s, is a commonly accepted screen. Additionally, PH is also recognised as a systolic pulmonary to systemic pressure ratio exceeding 0.5. Less widely used qualitative echocardiography alternatives include right atrial enlargement, septal flattening, right ventricular hypertrophy or dilatation, and right ventricular ejection time into the pulmonary artery <15 ms, but their sensitivity and specificity remain questionable. Where possible (ie, infants >5 kg), diagnosis made using echocardiography should be confirmed by cardiac catheterisation, and include vasoreactivity testing to oxygen and inhaled nitric oxide (iNO). Confirmation of PH requires pulmonary vascular resistance (PVR) >3 Wood units × BSA.m2 with capillary wedge pressures ≤15 mm Hg. This is important to distinguish PH from the hyperkinetic flows of unrepaired congenital heart disease.12 ,13
Mortality
Recent data based on contemporary treatments suggest BPD-PH survival rates after diagnosis of just 64% at 6 months, and 61% and 52% at 1- and 2-years, respectively.3 PH severity is an important prognostic marker for BPD, increasing mortality fourfold.14 That stated, prolonged sildenafil monotherapy data show 81% survival at 12 months and this is reinforced by other studies.15 ,16
BPD-PH management strategies
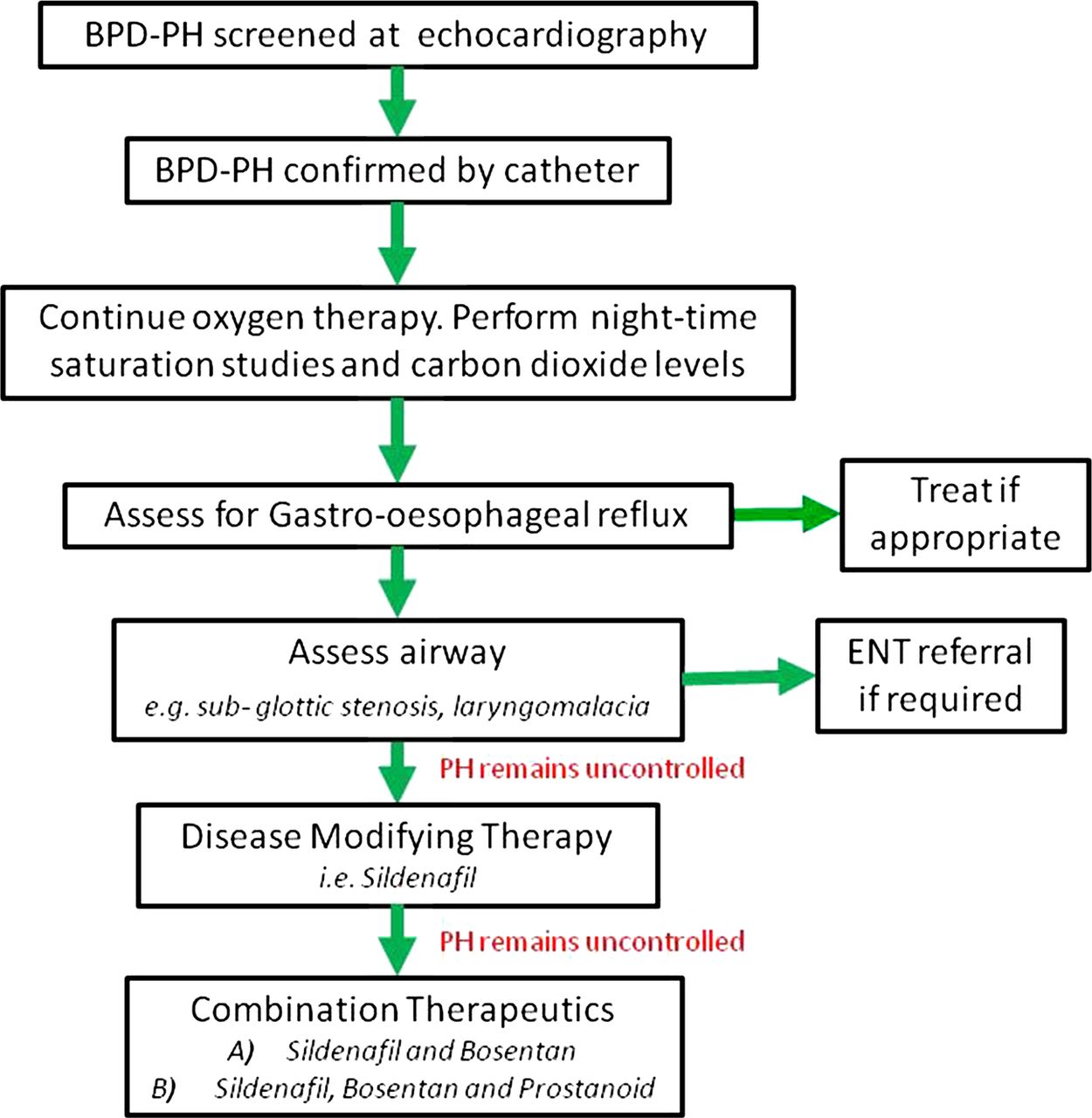
In most patients, BPD-PH gradually resolves over the course of the first year of life; however, active management is mandatory to avoid fatal right heart failure (cor pulmonale). Oxygen is the most potent vasodilator and the mainstay of therapy, but with oxygen alone BPD-PH has up to 50% mortality, with the majority of these deaths being linked directly to PH.9 iNO is a pulmonary vasodilator that relieves right ventricular afterload and improves ventilation–perfusion mismatching, yet this is expensive and cumbersome. That stated, the choice of vasodilator remains controversial, with sildenafil, prostacyclin analogues and endothelin receptor antagonists all manipulating different facets of pulmonary artery physiology. These agents have been compared on their ability to relieve BPD-PH, and a suggested guide to their application in this context is illustrated in figure 2.

Suggested treatment algorithm for the management of bronchopulmonary dysplasia-induced pulmonary hypertension (BPD-PH).
Sildenafil
The PDE-Vi sildenafil was the first US Food and Drug Administration (FDA) approved oral NO-augmentation strategy in PH for both adults and children.17 Current European Medicines Agency licensing includes those aged between 1 and 17 years for patients in WHO Group 1 PH under the guise of improving exercise tolerance. However, its use in BPD as well other conditions remains off-license; such issues are explored in further depth in a recent review.18
Pharmacodynamics
PVR is controlled by a balance of paracrine constrictors and dilators acting on vascular smooth muscle cells (VSMCs).19 ,20 In vivo, endothelial cell NO diffuses into VSMCs to activate soluble guanylate cyclase. This generates cyclic guanosine monophosphate (cGMP), which in turn mediates vasodilatation. Hence, instead of increasing production of cGMP like NO, PDE-Vis act to reduce cGMP degradation for similar vasodilator effect.21
Furthermore, a range of novel sildenafil actions leading to lasting PH resolution have been noted. This includes increased matrix metalloproteinase-2, and the modulation of the Rho-associated kinase signalling, reducing VSMC contraction and proliferation.22 ,23 In addition, evidence supports prolonged improvement in right ventricular function.24
Dosing
After oral administration, maximal sildenafil serum concentrations are reached within 0.5–1.5 h at 40% bioavailability.25 Importantly, sildenafil's 4 h half life before metabolism by the cytochrome P450 system has a range of consequences. This includes variable metabolic rates secondary to agents that either inhibit or induce this system. In practice, this causes plasma concentrations either above or below the targeted therapeutic window. Moreover, a neonate's system of metabolism requires time for maturation after birth, and delays in this cause drug half lives notably longer than anticipated, increasing the risk of adverse reactions and overdose.26
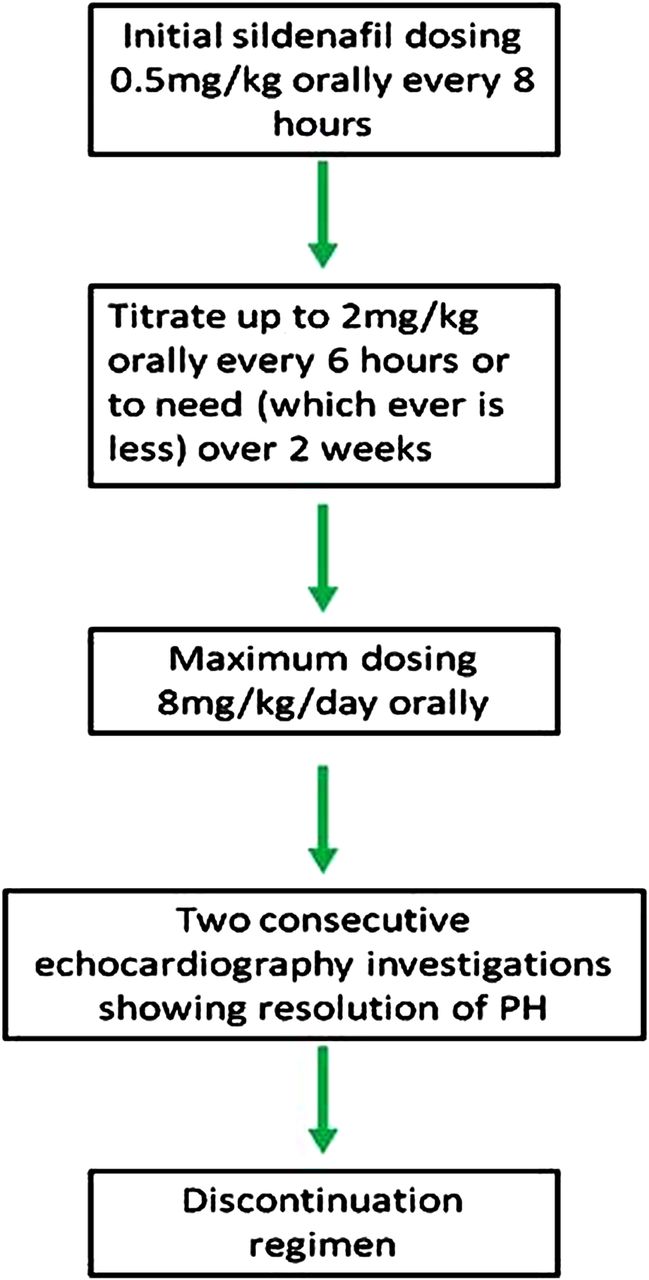
Broadly speaking, administration every 6–8 h with daily oral doses of 1–5 mg/kg, up to a maximum of 8 mg/kg/day, are effective and well tolerated, as explored more thoroughly later in this article.27 ,28 A guide dosing regimen is outlined in figure 3.

{kind=link}
{kind=link}
{kind=link}
Suggested treatment algorithm for bronchopulmonary dysplasia-induced pulmonary hypertension (PH) management using sildenafil.
Recently, intravenous sildenafil has become available and is primarily used to cover hospitalised patients normally maintained on oral sildenafil, although it has equal utility in infants starting sildenafil who cannot tolerate enteral administration. Increased bioavailability means smaller doses, usually 0.5 mg/kg, are given every 8 h.
It is important that patients commencing therapy are carefully monitored. Once discharged from hospital, children should be seen as paediatric cardiology outpatients every 2 months. Treatment can be gradually reduced and stopped when a patient is asymptomatic with two negative serial echocardiography investigations.29
Side effects
The most common adverse reactions are gastrointestinal upset, pyrexia and cough, although migraine and sleep disturbance can also be triggered.30 Notably, PDE-Vis have been linked with an unproven interference with retinal function and discontinuation is recommended in the context of visual disturbance and sildenafil is contraindicated in inherited retinal pathology.31 However, no evidence supports the withdrawal of treatment in the context of retinopathy of prematurity.32
Of the 43 patients with BPD-PH treated in published sildenafil studies, just two reported reactions required cessation of treatment. This includes systemic hypotension while using 0.5 mg/kg/day in an infant; however, after a 3-day therapeutic holiday this dose was successfully tolerated and then titrated up to 4 mg/kg/day.15 The other adverse effect was of frequent erections, a unique yet important reaction when considering lasting sildenafil compliance.
In 2012, a new controversy regarding the utility of sildenafil in paediatrics surfaced. A 3-year follow-up data detailing dose-dependent increases in child mortality with sildenafil led to the FDA withdrawing its recommendation for use in paediatric PH.33 ,34 However, the European Medicines Agency still supports this function, and the data's relevance to acute settings and BPD-PH remains unknown, especially given an altered risk–benefit balance.
Sildenafil evidence
Evidence for sildenafil in BPD-PH is limited. This is understandable given the complicated ethics of this field; however, this should not negate the trialling of newer strategies such as sildenafil, as this is how clinicians can potentially improve patients’ outcomes.
Sildenafil monotherapy
Regarding sildenafil monotherapy, there is a single case report documenting the successful resolution of BPD-PH in an infant.35 This 23-week gestation infant required sildenafil from 5 months age at oral doses up to 8 mg/kg/day alongside prolonged assisted ventilation. Treatment normalised right ventricular morphology (RV to LV end-diastolic diameter ratio 1.25 to <0.7) and resolved PH (pPA 70 to <25 mm Hg). Eighteen months after discontinuation of therapy, the patient was asymptomatic and pPA had normalised, suggesting long-lived effects. Furthermore, reducing the dose of sildenafil in this patient by 50% at 8 months caused a surge in pPA, suggesting a strong dose–effect relationship. Monotherapy is not recommended for BPD-PH in normal hospital situations, and this should be restricted to occasions in which no other option exists.
Sildenafil with NO
As stated above, combination therapy using sildenafil with iNO therapy has more extensive trialling.
A retrospective review into the use of sildenafil with iNO involved 5 years following 21 preterm infants suffering moderate or severe BPD.15 Sildenafil, titrated to a maximum oral dose of 6 mg/kg/day from a median age of 167 days, produced clinically significant reductions in estimated right ventricular peak systolic pressure (mean 65–53 mm Hg; p=0.01). Such reductions demonstrate the links between PVR and right-ventricular afterload, illustrating how BPD-PH management can improve both pulmonary and cardiac pathologies.
There is also a review tracing 25 sildenafil and iNO treated patients over 3 years.16 Oral sildenafil, dosed to a maximum of 8 mg/kg/day, was initiated at a median age of 184 days (range: 14–615 days) for a mean duration of 40 days (range: 6–60), and 22 of the 25 of infants showed PH improvement on echocardiogram at 40 days. In all, 13 patients also had echocardiography pPA estimates revealing decreases in both absolute pPA (64.9±20.3 to 40.2±13.2 mm Hg; p<0.001) and pPA to systolic blood pressure ratio (0.78±0.23 to 0.41±0.14; p<0.001). Additionally, 72% of patients exhibited improvement in inter-ventricular septal flattening. There were five deaths in this study and two adverse reactions; nevertheless, the authors concluded sildenafil to be safe and effective in BPD-PH.
Briefly stated, although limited in size and lacking random allocation, these studies suggest that the addition of sildenafil therapy is beneficial in the management of BPD-PH. In practice, combinations of therapies thought to augment each other are common. Such approaches allow clinicians to increase the likelihood of successful BPD-PH resolution, especially in refractory cases. As outlined in figure 2, this may involve iNO with sildenafil, or if this combination fails, then the further addition of endothelin antagonists and prostanoids.
Endothelin antagonists
Endothelin-1 (ET-1) antagonists act upon VSMC and endothelia via ETA and ETB receptors to affect NO and prostaglandin-independent vasodilatation. A dual receptor antagonist, bosentan, and a more ETA selective antagonist, ambrisentan, have both shown notable efficacy in paediatric PH.36 Case studies include the combination of sildenafil and bosentan in two infants over 3 years duration from an age of 2.5 years.37 Bosentan, at 31.25–62.5 mg twice daily, and sildenafil, 3–4 mg/kg/day, were well tolerated and associated with marked improvement in both clinical and physiological parameters, a point highlighted by substantial improvements in Ross Scale activity classification from class 4 to class 1.
Prostacyclin analogues
Prostacyclin analogues, such as iloprost, act upon cyclic AMP signalling in VSMCs to cause NO-independent vasodilatation. Data are limited regarding prostanoid–sildenafil combinations; however, one case study describes a 4-month-old preterm infant.38 Intravenous iloprost (2 ng/kg/min), oral sildenafil (0.5 mg/kg every 6 h, maximum 0.8 mg/kg/dose) and digoxin (10 µg/kg/day) were used. This combination treated the PH and at 1-year post-discontinuation the infant had normal pPA values and was asymptomatic, highlighting the combination's potential benefits.
Persistent PH of the newborn
Although a separate pathology from BPD-PH, persistent PH of the newborn (PPHN) shares many similarities with BPD-PH, principally the management of PH from the neonatal period. PPHN data are therefore additive to the existing body of evidence. Importantly, this evidence includes a recent Cochrane review.39 Here, sildenafil improved arterial oxygenation by 16 mm Hg (95% CI 7 to 24 mm Hg) with a relative mortality risk of 0.2 (95% CI 0.07 to 0.57). The review advocated the use of sildenafil in PPHN but highlighted that current randomised controlled trial (RCT) evidence remained insufficient. Although there is no official guidance or approval, doses typically start at 0.25–0.5 mg/kg and are titrated to need.
Current limitations
Alongside the aforementioned lack of available data, there are also questions around the studies and their terms and methods. Clinically, the exact definition of BPD used to select patients was rarely specified by the studies and due to a number of definitions existing, this could prove relevant to disease management. Additionally, the documentation of patient comorbidities and concurrent therapies was not always available and may have altered outcomes.
In terms of methodology, the lack of a control group in the above studies means that clinical improvement is vulnerable to confounding, and therefore may not directly reflect sildenafil effect. The requirement of a large double-blinded RCT into the use of sildenafil in BPD-PH is clear. Additionally, reliable morbidity and mortality data are essential before the prescribing of sildenafil for BPD-PH becomes widespread. An RCT investigating whether sildenafil reduces duration of ventilator support in preterm infants with evolving BPD born at 28 weeks gestation or less is now nearing completion.40 This trial, if robust, will add significantly to safety evidence supporting the use of sildenafil BPD-PH.
The use of case studies as evidence for sildenafil's utility also increases the probability of publication bias. Failed trials of sildenafil in BPD-PH are unlikely to be written-up or published meaning there is a risk that only favourable data are available for compilation within this review. That stated, our own clinical experiences show a generally positive effect with a trend in line with aforementioned evidence.
Last, long-term outcomes are not yet available. This is partly due to the relatively infrequent nature of BPD-PH and the recent application of sildenafil in this utility. It is important that these cases are analysed longitudinally, as continued improvement and possible resolution is the aim of BPD-PH therapy, especially given the aforementioned recent mortality data for long-term sildenafil in paediatric PH.
Conclusions
Evidence suggests prolonged sildenafil therapy at doses of 2 mg/kg every 6 h can be considered when managing infants with BPD-PH. Encouraging data exist for its haemodynamic benefits, safety profile and use in combination with other therapies, especially in the long-term settings where iNO is not suitable. However, due to a limited and underpowered evidence-base, and recent controversial mortality data in paediatric PH, prescribing should be restricted to specialist units and physicians, ideally with experience in dealing with both BPD and PH.
References
Footnotes
-
RW and AW are acting as joint first authors on this project.
-
Contributors All the authors contributed significantly to the conception and design of this work, including the analysis and interpretation of data, drafting of the article with subsequent revisions regarding important intellectual content. All the authors also gave their final approval for the version submitted for publication.
-
Competing interests There is no conflict of interest. Dr Tulloh has received unrestricted educational grants from Pfizer, GSK, Actelion and Encysive for his work in pulmonary hypertension.
-
Provenance and peer review Not commissioned; externally peer reviewed.