Article Text

Statistics from Altmetric.com
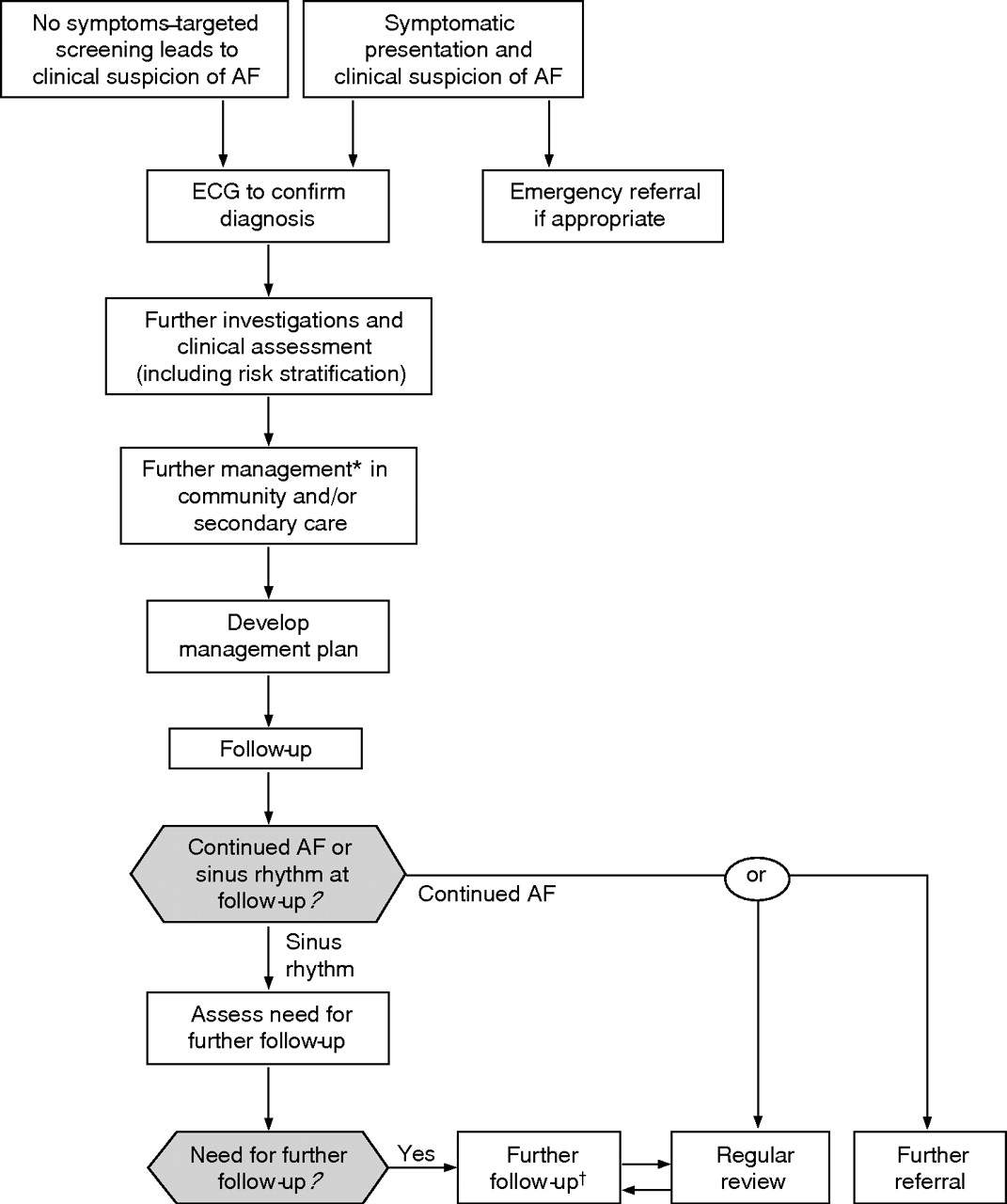
The patient care pathway maps the sequence of decisions that will be required to identify, assess, manage and monitor patients with atrial fibrillation (fig 1⇓). The pathway also provides a “guide to the guideline” in that the decisions taken will be informed by the evidence base and recommendations of the full guideline document.
{kind=link}
Care pathway for diagnosing and treating atrial fibrillation. AF, atrial fibrillation; ECG, electrocardiogram.*Further management to include rate or rhythm control treatment strategy and appropriate antithrombotic therapy based on stroke risk stratification model.†Further follow-up for co-existing conditions and assessment for ongoing anticoagulation.
Diagnosis
The guideline recommends that in patients presenting with breathlessness, palpitations, syncope, chest discomfort or stroke, pulse palpation should be carried out to determine the presence of an irregular pulse that may indicate underlying atrial fibrillation. Thus, the detection of patients with atrial fibrillation, especially those asymptomatic, will be enhanced by opportunistically checking the pulse in “high-risk” patients attending for review. Confirmation of the arrhythmia through an electrocardiogram (ECG) is essential.
Further investigation and clinical assessment
Further assessment and investigation focuses on identifying the cause of atrial fibrillation, on judging whether electrical or pharmacological intervention is required to control the arrhythmia and, finally, on establishing the risk of stroke and thromboembolism. Much of clinical assessment, basic blood tests (including thyroid function tests) and a chest x ray can be initiated in primary care. More specialised investigations, such as echocardiography or electrophysiological studies, may require referral to secondary care. Some general practitioners have access to open-access echocardiography, which may facilitate patient assessment for structural and functional heart disease. While most cardiologists would perform echocardiography, the guideline offers some pragmatic recommendations on when transthoracic (and transoesophageal) echocardiography should be done.
Treatment strategy
In all cases of atrial fibrillation, consideration should be given to whether the arrhythmia should be treated and how. A rhythm control strategy is directed towards the reduction of paroxysms or recurrences of atrial fibrillation, cardioversion of persistent atrial fibrillation and long-term maintenance of sinus rhythm. In contrast, a rate control strategy is directed towards controlling the ventricular rate to reduce symptoms and optimise cardiac function. In patients with newly diagnosed atrial fibrillation in which antithrombotic treatment is indicated, such treatment should be initiated with minimal delay after the appropriate management of comorbidities.
All patients with paroxysmal, persistent or permanent atrial fibrillation should undergo regular risk–benefit assessment using the National Institute for Health and Clinical Excellence (NICE) risk stratification algorithm. Even in patients with atrial fibrillation who have undergone successful cardioversion, anticoagulation should be continued long term in patients at high risk of atrial fibrillation recurrence or with co-existent stroke risk factors. Many clinicians also erroneously regard paroxysmal atrial fibrillation as being at lower stroke risk, dispensing with the need for anticoagulation, whereas the approach to thromboprophylaxis remains the same as that for permanent atrial fibrillation.
However, other considerations also apply when assessing a patient for thromboprophylaxis—for example, whether a patient can access anticoagulation monitoring facilities, associated comorbidities (eg, falls, bleeding tendencies) and the need for polypharmacy.
Monitoring
Patients who are successfully cardioverted should be subject to specialist review at 1 month and at 6 months to check the maintenance of sinus rhythm, after which they may be discharged with an appropriate management strategy to primary care. Patients should be educated to attend primary care if symptoms suggestive of atrial fibrillation recur.
Most patients with atrial fibrillation will be followed up in primary care. This will provide an opportunity to check the heart rate and rhythm, to manage comorbid conditions and to reassess risk stratification. Patients taking warfarin should attend for anticoagulant dose monitoring in services that have been commissioned locally.
Referral
A small group of patients are haemodynamically compromised at the onset of atrial fibrillation (box 1⇓). Such patients require immediate hospitalisation. Emergency referral for cardioversion should also be considered in patients who have had atrial fibrillation for <48 h, as they may be cardioverted without the need for anticoagulation. The strategy for managing paroxysmal atrial fibrillation is tailored to the patient and referral is required for specialist advice. In patients with persistent atrial fibrillation, referral is required for elective cardioversion and for specialist advice on pharmacotherapy. Specialist advice may be required to establish pharmacotherapy in patients with permanent atrial fibrillation, but not all patients with atrial fibrillation require pharmacotherapy and not all patients requiring pharmacotherapy require specialist advice. The most common reason for referral for specialist investigation or intervention is failed medical treatment, lone atrial fibrillation, or specific electrophysiological problems including Wolff–Parkinson–White syndrome and focal or slow, symptomatic atrial fibrillation.
Indications for referral of patients with atrial fibrillation
Immediate
haemodynamic compromise at the onset of atrial fibrillation
Early
onset of atrial fibrillation within 48 h
patients with symptomatic atrial fibrillation
Elective
paroxysmal atrial fibrillation
persistent atrial fibrillation for possible cardioversion
persistent or permanent atrial fibrillation for advice on pharmacotherapy
failure of medical treatment
Wolff–Parkinson–White syndrome
lone atrial fibrillation
focal or slow symptomatic atrial fibrillation, which may benefit from pacing
IMPLEMENTATION AND AUDIT
Box 2⇓ gives the priorities for implementation. The successful implementation of these guidelines depends on a partnership between primary and secondary care and the patient. Some people may present with atrial fibrillation that is sufficiently symptomatic for conducting the initial management as an emergency in a secondary care setting. However, for most people with atrial fibrillation the initial diagnosis and management will be conducted in primary care. All practices will need to ensure that they have rapid access to 12 lead echocardiographs so that these can be taken during an episode of irregular pulse. Ideally, this standard investigation should be available in each instance. Many practices have open access to 24-h ECGs for selected indications and this service should be made more widely available to avoid unnecessary referral for the diagnosis of paroxysmal atrial fibrillation.
Priorities for implementation
The following five recommendations have been identified as priorities for implementation:
An electrocardiogram should be performed in all patients, whether symptomatic or not, in whom atrial fibrillation is suspected because of the detection of an irregular pulse
As some patients with persistent atrial fibrillation will satisfy the criteria for either an initial rate-control or a rhythm-control strategy (eg, age >65 years but also symptomatic):
the indications for each option should not be regarded as mutually exclusive, and the potential advantages and disadvantages of each strategy should be explained to patients before agreeing on which to adopt
any comorbidities that might indicate one approach rather than the other should be taken into account
irrespective of whether a rate-control or a rhythm-control strategy is adopted in patients with persistent atrial fibrillation, appropriate antithrombotic treatment should be used
In patients with permanent atrial fibrillation who need treatment for rate control:
β-blockers or rate-limiting calcium antagonists should be the preferred initial monotherapy in all patients
digoxin should only be considered as monotherapy in predominantly sedentary patients
In patients with newly diagnosed atrial fibrillation for whom antithrombotic treatment is indicated, such treatment should be initiated with minimal delay after the appropriate management of comorbidities
The stroke risk stratification algorithm should be used in patients with atrial fibrillation to assess their risk of stroke and thromboembolism, and appropriate thromboprophylaxis given
Once the diagnosis has been made, further investigations may be needed to assess and risk stratify the patient. Many primary care trusts (PCTs) have provided open access to echocardiography, mainly for the diagnosis of left ventricular systolic dysfunction. An extension of this service to selected patients with atrial fibrillation would also help to prevent unnecessary referrals.
Equipped with the results of the investigations and having risk stratified the patient, two main decisions are to be made regarding (1) whether anticoagulant or antiplatelet therapy is needed and (2) whether a rate or rhythm strategy is the best option. The patient and/or carers will need to be given sufficient information and advice to help them make the appropriate decisions. In uncomplicated cases, anticoagulation and the rate control strategy can be dealt with in primary care, but a rhythm control strategy will normally be implemented in secondary care. Long-term follow-up will normally take place in the community. In patients with atrial fibrillation who require long-term anticoagulation, monitoring may be done in the practice as a locally enhanced service or may be commissioned from a third party under the commissioning process. Self-management with point of care testing should be considered only when an adequate educational programme is in place to train patients or carers, when the patient or carer is motivated and able to perform self-monitoring, and provided the ability to perform self-monitoring is regularly reviewed.
To enhance the patient experience and to optimise clinical management, each local health economy should agree on an optimal care pathway. Ideally, this should be achieved through a clinical network which is comprised of committed clinicians, managers and commissioners who work together to improve care. Networks are uniquely placed to make a difference, as they link clinicians involved in every aspect of the patient journey through the local National Health Service (NHS) system in primary, secondary and tertiary care. Networks are intended to ensure delivery of an equitable standard of care to all patients irrespective of geographical location.
There should be some synergy with local plans to delivery of chapter 8 of the National Service Framework (NSF) on Arrhythmia and Sudden Cardiac Death—for example, in West Yorkshire, a first draft consultation document was published in January 2006, and once finalised it will be used by local implementation teams/modernisation teams to help implement the NICE atrial fibrillation recommendations. It is planned to review implementation on a quarterly basis and there will be formal performance management by the strategic health authority.
However, models for the delivery of care in the NHS are changing and arrhythmia clinics are likely to be provided both in primary and in secondary care as a means of assisting with the assessment, management and review of patients with arrhythmias, including atrial fibrillation.
Audit
An important audit tool in primary care is the Quality and Outcomes Framework (QOF) of the new General Medical Services (GMS) contract. The latest annual revision of the QOF came into effect from 1 April 2006, and 138 points in the previous QOF have been re-assigned to new clinical areas. Of note, 30 of these have been allocated to atrial fibrillation. The requirement on practices to produce a register of patients with atrial fibrillation will provide an essential basis for structured and systematic care. Furthermore, all patients diagnosed will need to have their diagnosis confirmed by an ECG or by a specialist, and practices are required to provide details regarding the decision to treat the patient with anticoagulant or antiplatelet treatment. Auditing performance in the QOF will be used by PCTs, strategic health authorities and networks to monitor progress. Comparative data will identify poor performance, which needs to be managed, and good practice, which can be shared.
The implementation of atrial fibrillation guidelines will need to be monitored if the ideal of continuous quality improvement is to be applied to this area of clinical care. Audit criteria that reflect key the areas for implementation are needed. Table 1⇓ gives the suggestions that work synergistically with QOF and are suggested markers of best practice.
Audit criteria
AREAS FOR FUTURE RESEARCH
Five topics for future research are recommended as priorities for research funding in this guideline. Topics were chosen on the basis of a lack of published evidence on which recommendations may be made for important areas in the management of atrial fibrillation.
Cardioversion
Further research is needed to determine the comparative efficacy of different modalities of cardioversion, including pharmacological cardioversion, electrical cardioversion, or electrical cardioversion with the adjunctive use of antiarrhythmic drugs pre-cardioversion. Long-term outcomes and short-term outcomes should be considered.
Echocardiography
Although there is evidence supporting the use of transthoracic echocardiography (TTE) to inform the management of those patients in whom a strategy of rhythm control is being considered, there is little evidence supporting the use of routine TTE in all patients with newly diagnosed atrial fibrillation. Further research is needed in this aspect to determine the cost effectiveness of routine TTE of all newly diagnosed patients with atrial fibrillation.
Co-prescribed anticoagulation and antiplatelet treatment
Although there is strong evidence supporting the use of anticoagulation as thromboprophylaxis in patients with atrial fibrillation, there is little evidence supporting the use of aspirin, either alone or in addition to warfarin. This represents a dilemma for those patients with stents, or a history of myocardial infarction in addition to atrial fibrillation in whom both anticoagulation and antiplatelet treatment are indicated. Further research is needed in such patients to determine the most effective antithrombotic treatment.
Pill-in-pocket treatment
Although continuous antiarrhythmic treatment may be appropriate in some patients with paroxysmal atrial fibrillation, in others the infrequency or tolerability of the paroxysms may not justify the possible side effects. A pill-in-the-pocket treatment may therefore be a safer and effective solution in some patients with paroxysmal atrial fibrillation. Further research is needed to determine the long-term safety and effectiveness, in addition to the effect on patient quality of life.
Anticoagulation in paroxysmal atrial fibrillation
Further research is needed to determine the safety and efficacy of anticoagulation in patients with paroxysmal atrial fibrillation and whether it is justified for use in all patients regardless of the frequency or duration of paroxysms.
DISCUSSION
Although some people present to secondary care with severe and acute symptoms attributable to atrial fibrillation, for most people with atrial fibrillation the initial diagnosis and, for many, the management will be conducted in primary care. These guidelines should be used in each and every practice to ensure that their practice protocol contains clear information about how to lead discussions regarding the rate and rhythm control options and the use of anticoagulants.
Key partnerships have an influence on successful implementation of guideline. Firstly, the patients or carers will need to be given sufficient information and advice to help them participate in management decisions that will ensure that their treatment is the one most suitable for them. An informed discussion of risk–benefit issues which consider patient preference is essential. Secondly, the successful implementation of the guidelines depends on a partnership between primary, secondary and tertiary care. There is cause for optimism from an increasing understanding that co-operation is essential when we look to redesign services.
Practice-based commissioning will include all practices by the end of 2006 and, in principle, allows practices to commission or decommission care with the agreement of their PCT. Practice-based commissioning provides opportunities for the development and extension of services in primary care that might include aspects of atrial fibrillation assessment and management that have previously been provided in secondary care. Further education and training of staff will be required to manage the case load of patients with atrial fibrillation that active case finding will generate, but the existence of cardiac clinical networks provides a forum in which clinicians from primary and secondary care can work together to ensure that appropriate care is provided by appropriate people and in an appropriate location.
Although monitoring the implementation of this guidance is likely to be left to PCTs, the business of delivering improved care to patients will be down to the efforts of motivated and well-informed clinicians working in a structured manner.
Footnotes
Published Online First 4 September 2006
Competing interests: None declared.