Article Text

Statistics from Altmetric.com
- echocardiography
- ischaemic cardiomyopathy
- myocardial hibernation
- positron emission tomography (PET)
- single photon emission computed tomography
- SPECT
- tissue Doppler echocardiography
Coronary artery disease is the most common cause of congestive heart failure. More than 70% of the patients with heart failure symptoms have underlying coronary disease, whereas the majority of patients with ischaemic cardiomyopathy have a previous myocardial infarction.1,2 The prognosis of these patients is poor, particularly in men, and many of them need intermittent hospitalisation because of decompensated heart failure. In the near future, chronic heart failure will be encountered even more often, as our population ages.1,2 The clinical characteristics of the patient, the presence of ischaemia, and severity of left ventricular dysfunction determine the prognosis in heart failure.
Traditionally, ischaemic left ventricular dysfunction was considered an irreversible process. In patients with ischaemic cardiomyopathy, medical treatment was regarded as the only management option. However, more than two decades ago, Diamond and Rahimtoola recognised that left ventricular dysfunction in these patients is not always permanent and launched the theory of myocardial hibernation.3,4 Hibernating myocardium is defined as chronic reversible contractile dysfunction secondary to coronary artery disease. The presence of hibernating myocardium has become an additional motive to perform coronary revascularisation. In fact, if a substantial amount of hibernating myocardium is present, coronary revascularisation may substantially improve regional and global contractile function in selected patients with ischaemic cardiomyopathy.5
This article will focus on the clinical importance and identification of myocardial viability in patients with chronic ischaemic left ventricular dysfunction.
PATHOPHYSIOLOGY OF VIABLE MYOCARDIUM
In patients with ischaemic cardiomyopathy several (patho)physiological conditions of the myocardium may coexist. Often there are areas with preserved contractile function supplied by coronary arteries without significant stenoses. On the other hand, contractile dysfunction can be observed in myocardial regions that are subtended by a stenotic or occluded coronary artery. Coronary occlusion may cause cellular death resulting in irreversibly scarred myocardium.6 Alternatively, the reduced contractile function may be a result of adaptation to an (intermittent) reduction in blood flow. This physiological down-regulation of contractile function, also referred to as myocardial hibernation, may be an adequate response to myocardial ischaemia, to protect myocytes from irreversible damage. Biopsy samples obtained during coronary bypass surgery demonstrate that hibernating myocardium is characterised by a loss of contractile proteins, whereas cell membrane and cellular metabolism remain intact.7 Restoration of blood flow by coronary revascularisation may result in recovery of contractile function in hibernating myocardium. The time course of functional recovery of hibernating myocardium may vary considerably,8 and depends on several factors including the duration and severity of myocardial ischaemia, the time and completeness of myocardial revascularisation, and the extent of ultrastructural alterations within the dysfunctional myocardium. Less severely damaged myocardium may improve within three months of revascularisation, in contrast to severely damaged tissue, which may take more than one year to fully recovery in function after revascularisation.
Besides hibernating myocardium, patients with ischaemic cardiomyopathy often have some regions that contain (chronically) stunned myocardium. Myocardial stunning is characterised by a depressed contractile function in the presence of normal resting blood flow,6 and may occur as a result of repetitive ischaemic episodes.
HOW TO ASSESS MYOCARDIAL VIABILITY?
Some information can be derived from the ECG, but imaging is clearly preferred. Several non-invasive imaging techniques have been developed to identify dysfunctional but viable tissue: dobutamine stress echocardiography, single photon emission computed tomography (SPECT) imaging with thallium-201 or technetium-99 m labelled tracers, and positron emission tomography (PET) metabolic imaging with F18-fluorodeoxyglucose (FDG). These techniques evaluate different characteristics of viable myocardium and can delineate irreversibly scarred from dysfunctional but viable myocardium (table 1).
Characteristics of dysfunctional but viable myocardium
The ECG
The ECG has the obvious advantage of a widespread availability and limited costs, but there is no clear correlation between Q waves on ECG and the presence of viable or non-viable myocardium. Also, the relation between ST segment changes (in particular ST segment elevation) during stress testing and myocardial viability is not entirely clear. However, QT dispersion is related to the presence of myocardial viability in patients with ischaemic cardiomyopathy. Patients with preserved QT dispersion are likely to have a substantial amount of viable myocardium, whereas patients with a high QT dispersion have predominantly non-viable scar tissue.
Echocardiographic techniques
Resting echocardiography
From the resting images, an initial impression concerning the absence of viability can be derived. A pronounced end diastolic wall thinning virtually excludes the presence of viable tissue.9 In patients without a clear thinning of the dysfunctional area, low dose dobutamine echocardiography can be performed to evaluate myocardial viability.
Dobutamine stress echocardiography
Dobutamine stress echocardiography is a widespread and relatively inexpensive method to assess myocardial viability (fig 1). Dysfunctional but viable myocardium is characterised by preserved contractile reserve during dobutamine echocardiography.10 In hypokinetic or akinetic regions, an improvement of contraction during low dose dobutamine infusion (5–10 μg/kg/min) is indicative of viable tissue. To improve the assessment of viability, the low dose dobutamine protocol may be extended by high dose dobutamine stress (with dosages up to 40 μg/kg/min and the addition of atropine). This protocol allows assessment of the biphasic response: an initial improvement of contractility during low dose dobutamine stress and worsening of contractile function during high dose dobutamine infusion caused by stress induced ischaemia. This response is highly predictive of recovery of function after revascularisation. Dobutamine stress echocardiography is a safe test in patients with ischaemic cardiomyopathy; the most common side effects are hypotension and self limiting arrhythmias.

Transthoracic two dimensional echocardiogram (apical four chamber view, end systolic) at rest (left panel) and during infusion of low dose dobutamine (right panel) in a patient with ischaemic cardiomyopathy and severe hypokinesia of the septum and lateral wall. During low dose dobutamine, improved contraction of the dysfunctional segments indicates myocardial viability.
Tissue Doppler imaging
Tissue Doppler imaging was developed to overcome the subjective nature of the echocardiographic examination. Tissue Doppler imaging allows quantification of myocardial function using the Doppler shift principle. Tissue Doppler images may be displayed as colour encoded velocity profiles in M mode and two dimensional imaging formats. For viability assessment tissue Doppler echocardiography may be combined with low dose dobutamine infusion. In dysfunctional but viable myocardium, baseline tissue velocity is impaired, and myocardial velocities increase during dobutamine infusion. The major advantage of this technique is the high spatial and temporal resolution. Rambaldi and colleagues11 compared pulsed wave tissue Doppler imaging with dobutamine stress echocardiography in 40 patients with ischaemic cardiomyopathy, using FDG imaging as the gold standard for viability assessment. Tissue Doppler imaging resulted in a significant increase in sensitivity of dobutamine echocardiography to detect viable myocardium.
Contrast echocardiography
Two dimensional echocardiography may be combined with intravenous contrast administration to assess both myocardial function and myocardial perfusion in real time (fig 2). A bolus of contrast is intravenously injected followed by a saline flush. Echocardiography using a low mechanical index is started before contrast injection and subsequently “flash” imaging with high mechanical index is used at peak contrast intensity to destroy the microbubbles in the myocardium, to avoid artefacts and to visualise myocardial contrast replenishment. Because contrast echocardiography allows simultaneous assessment of function and perfusion, stunned myocardium can be distinguished from hibernation. Shimoni and colleagues12 studied the accuracy of contrast echocardiography in 20 patients with coronary disease and left ventricular dysfunction who underwent bypass surgery. Optimal identification of viable myocardium was obtained when perfusion as assessed by contrast echocardiography was analysed quantitatively.

Transthoracic two dimensional echocardiogram after intravenous injection of a contrast agent (apical four chamber view). Opacification of the left ventricular cavity after administration of the contrast agent facilitates endocardial border delineation (left panel). Subsequently, a destruction–fill method can be used to assess myocardial perfusion. In this example, a perfusion defect was present in the hypokinetic lateral wall.
Nuclear techniques: SPECT
Thallium-201
Thallium-201 is a cationic γ emitter, which is taken up by the myocardium similarly to potassium. The early uptake of thallium-201 is proportional to regional blood flow, whereas delayed uptake indicates a preserved sodium–potassium pump and an intact cell membrane. Several protocols have been developed to evaluate myocardial viability including stress–redistribution–reinjection and rest–redistribution. Dilsizian and colleagues13 demonstrated that reinjection of thallium-201 following acquisition of the redistribution images may further improve the detection of viable myocardium. Because the stress–redistribution–reinjection technique is labour intensive and requires three image acquisitions, many nuclear cardiology laboratories use shorter, modified imaging protocols. Exercise is the first choice stressor, because exercise capacity itself provides prognostic information. In patients unable to perform an exercise test, pharmacological stress can be used.
Technetium-99 m labelled tracers
Technetium-99 m labelled tracers (technetium-99 m sestamibi, technetium-99 m tetrofosmin) can be used to assess perfusion and intact mitochondria. The shorter half life allows the use of higher dosages than for thallium-201, and in combination with the higher photon energy, excellent image quality can be obtained with the technetium-99 m labelled agents. A major advantage is that the recent technical developments have resulted in gated imaging allowing simultaneous assessment of myocardial perfusion and contractile function. Currently, gating is performed in the majority of studies with the technetium-99 m labelled agents. Several studies have shown that technetium-99 m labelled tracers may underestimate myocardial viability as compared to FDG PET. However, more recent studies have shown that viability assessment using technetium-99 m labelled tracers can be improved by administration of nitrates.
Nuclear techniques: PET
FDG to assess glucose utilisation
Generally, glucose utilisation is evaluated with the glucose analogue FDG and compared to regional myocardial perfusion assessed with N13-ammonia, rubidium-82, or O15-labelled water.14–17 A normal perfusion and FDG uptake, or reduced perfusion with enhanced FDG uptake (mismatch pattern), indicates viable myocardium. Conversely, a concordant reduction in FDG uptake and myocardial perfusion (match pattern) is indicative of scar tissue. PET is often considered the reference technique for the assessment of myocardial viability, because of the quantitative results, high spatial resolution, and good correlation with outcome after coronary revascularisation.14–17 The introduction of SPECT using dedicated (511 keV) collimators (fig 3) has contributed to a more extensive use of metabolic imaging, since PET facilities are limited and relatively expensive. Several studies have demonstrated that FDG SPECT and FDG PET imaging have a comparable diagnostic accuracy for the assessment of myocardial viability.18
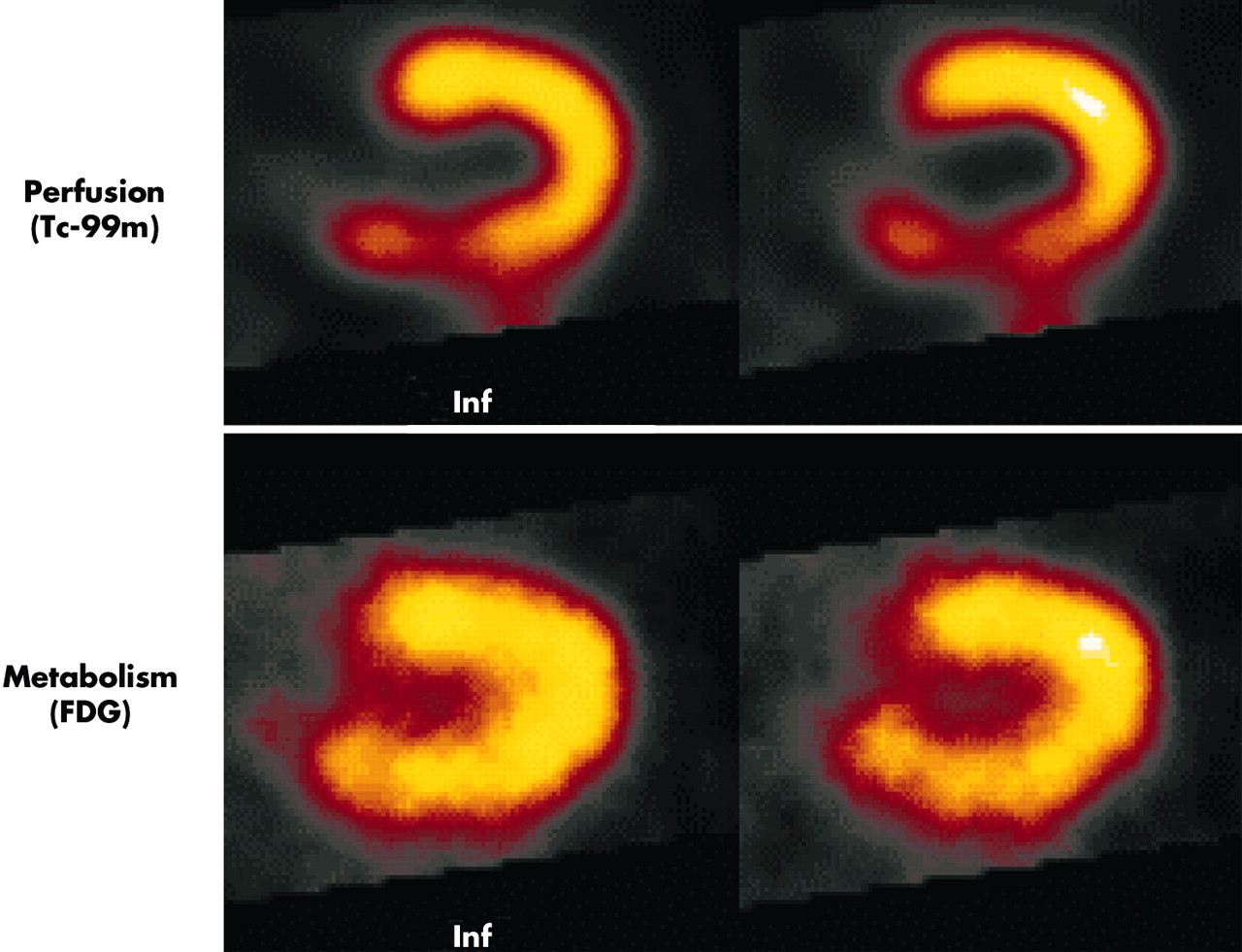
Dual isotope simultaneous acquisition SPECT scan (horizontal long axis slices) showing a substantial perfusion–metabolism mismatch in the inferior wall, indicating viable myocardium.
Alternative PET techniques
Besides FDG imaging, PET may be combined with C11-acetate to assess residual oxidative metabolism. Clearance rates of C11-acetate from dysfunctional myocardium reflect the rate of oxidative phosphorylation. The rate of oxidative metabolism has been demonstrated to correlate closely to improvement of function after myocardial revascularisation. Gropler and colleagues15 studied 34 patients with coronary artery disease and compared C11-acetate PET with FDG PET for prediction of functional recovery after revascularisation. Assessment of regional oxidative metabolism by PET with C11-acetate was an accurate predictor of functional recovery, and was slightly more accurate than FDG PET.
Rubidium-82 (Rb82) is another PET tracer, which allows assessment of both myocardial perfusion and cell membrane integrity. Yoshida and Gould16 evaluated a large cohort of patients with Rb82 and demonstrated that the prognosis of patients with chronic ischaemic left ventricular dysfunction was dependent on both the infarct size and the extent of viability, as derived from the Rb82 images.
PET also allows non-invasive assessment of the water perfusable tissue fraction (PTF). This parameter is derived from quantification of myocardial blood flow using 15O-water (H215O). Information on the accuracy of PTF for the prediction of functional recovery is still limited. Bax and colleagues17 studied 34 patients with ischaemic cardiomyopathy who underwent myocardial revascularisation with both 15O-water and FDG PET to compare the relative merits of myocardial blood flow (MBF), metabolic rate of glucose (MRG, absolute and relative), and PTF. High sensitivities for the prediction of improvement of left ventricular ejection fraction after revascularisation were observed for all PET indexes, whereas the specificities of the various techniques were somewhat lower.
Magnetic resonance imaging
Recently, magnetic resonance imaging (MRI) was introduced to evaluate myocardial viability. Currently, three techniques are being used:
-
resting MRI to measure end diastolic wall thickness
-
dobutamine MRI to evaluate contractile reserve
-
contrast enhanced MRI to detect the extent and transmurality of scar tissue.
Resting MRI
Resting MRI can be used to assess end diastolic wall thickness and contractile function at rest. Several studies have demonstrated that segments with an end diastolic wall thickness < 6 mm most likely represent transmural scar formation and contractile function will not improve after myocardial revascularisation. However, dysfunctional segments with a preserved wall thickness will not always recover after revascularisation. This may be related to the presence of subendocardial scar in these segments. Therefore, additional testing is needed to predict outcome in the segments with preserved end diastolic wall thickness.
Dobutamine MRI
Dobutamine MRI can be used to evaluate contractile reserve, in a similar manner to dobutamine echocardiography.19 The major advantage of MRI over echocardiography is the increased resolution of MRI, allowing for quantitative assessment of wall thickening during dobutamine infusion, and thus avoiding the subjective analysis of echocardiography. Baer and colleagues have initially demonstrated an excellent agreement between dobutamine MRI and FDG PET19; in a subsequent study the authors reported a sensitivity of 89% with a specificity of 94% to predict improvement in resting function after revascularisation.20
Contrast enhanced MRI
When combined with gadolinium based contrast agents, MRI allows precise detection of scar tissue. Animal experiments have demonstrated an excellent correlation between the extent and transmurality of scar tissue and contrast enhancement on MRI.21 Due to the high spatial resolution, MRI is currently the only technique that permits evaluation of the different myocardial layers and contrast enhanced imaging makes detection of subendocardial scar tissue possible (fig 4). Klein and colleagues22 compared contrast enhanced MRI with FDG PET in 31 patients with ischaemic cardiomyopathy and showed an excellent agreement between the two techniques to detect scar tissue. More recently, Kim and colleagues23 applied contrast enhanced MRI in 41 patients with chronic left ventricular dysfunction undergoing revascularisation. The authors demonstrated that the likelihood of improvement in regional contractility after revascularisation progressively decreased as the transmural extent of hyperenhancement increased.

Contrast enhanced MRI in a patient with an anterior wall infarction.
Electromechanical mapping to assess viability
Electromechanical assessment of myocardial viability has been developed using the NOGA system, a catheter based, non-fluoroscopic, three dimensional endocardial mapping system. Based on integrated assessment of function and electrical activity, delineation of dysfunctional but viable myocardium is possible. When a threshold amplitude of 7.5 mV was used, the sensitivity and specificity for detecting viable myocardium were 77% and 75%.24 Electromechanical mapping is not the technique of choice to assess viability in a diagnostic setting, but may be useful as a platform for additional procedures. For example, electromechanical mapping may be used to assess viability and generate three dimensional left ventricular reconstruction before laser revascularisation, intramyocardial gene transfer, or myoblast injection.25
CLINICAL IMPORTANCE OF VIABILITY ASSESSMENT
Patients with heart failure symptoms caused by ischaemic cardiomyopathy represent a high risk group. In various registries of patients with left ventricular dysfunction, the one year mortality rates range from 15–40%.1,2 To improve clinical outcome in these patients, several treatment options have been developed. Patients with ischaemic cardiomyopathy deserve careful evaluation and treatment needs to be tailored to the individual patient. Significant progress in the management of ischaemic cardiomyopathy has been achieved with medical treatment, including angiotensin converting enzyme inhibitors, spironolactone, and low dose β blocking agents.26–28 However, medical treatment is still associated with a suboptimal prognosis in patients with ischaemic cardiomyopathy. Heart transplantation is associated with a favourable survival, but the availability of donor hearts is limited. Many patients who are eligible for transplantation will not receive a donor heart and die awaiting transplantation. Coronary revascularisation may be a good alternative treatment for the subgroup of patients with a substantial amount of dysfunctional but viable myocardium.5 Recent studies have demonstrated that in more than 50% of patients with ischaemic cardiomyopathy, a clinically significant amount of viable myocardium is present. In these patients, revascularisation may improve, and even normalise, left ventricular ejection fraction, heart failure symptoms, exercise capacity, and survival. Moreover, data from 258 consecutive patients indicated that recovery of global function can be anticipated after myocardial revascularisation in almost 40% of patients with ischaemic cardiomyopathy.29 These observations indicate the need for a careful analysis of patients with heart failure (even in the absence of angina pectoris) including assessment of viability, on a routine basis. Two dimensional echocardiography is an excellent first step to assess regional and global contractile function and valvar function. Myocardial stress imaging can then be used to evaluate ischaemia, followed by coronary angiography to assess the extent and severity of coronary artery disease and also evaluate whether the coronary anatomy is amendable for coronary revascularisation. Finally, viability testing should be performed using one of the non-invasive imaging techniques, and based on the findings, the treatment can be tailored to the individual patient.
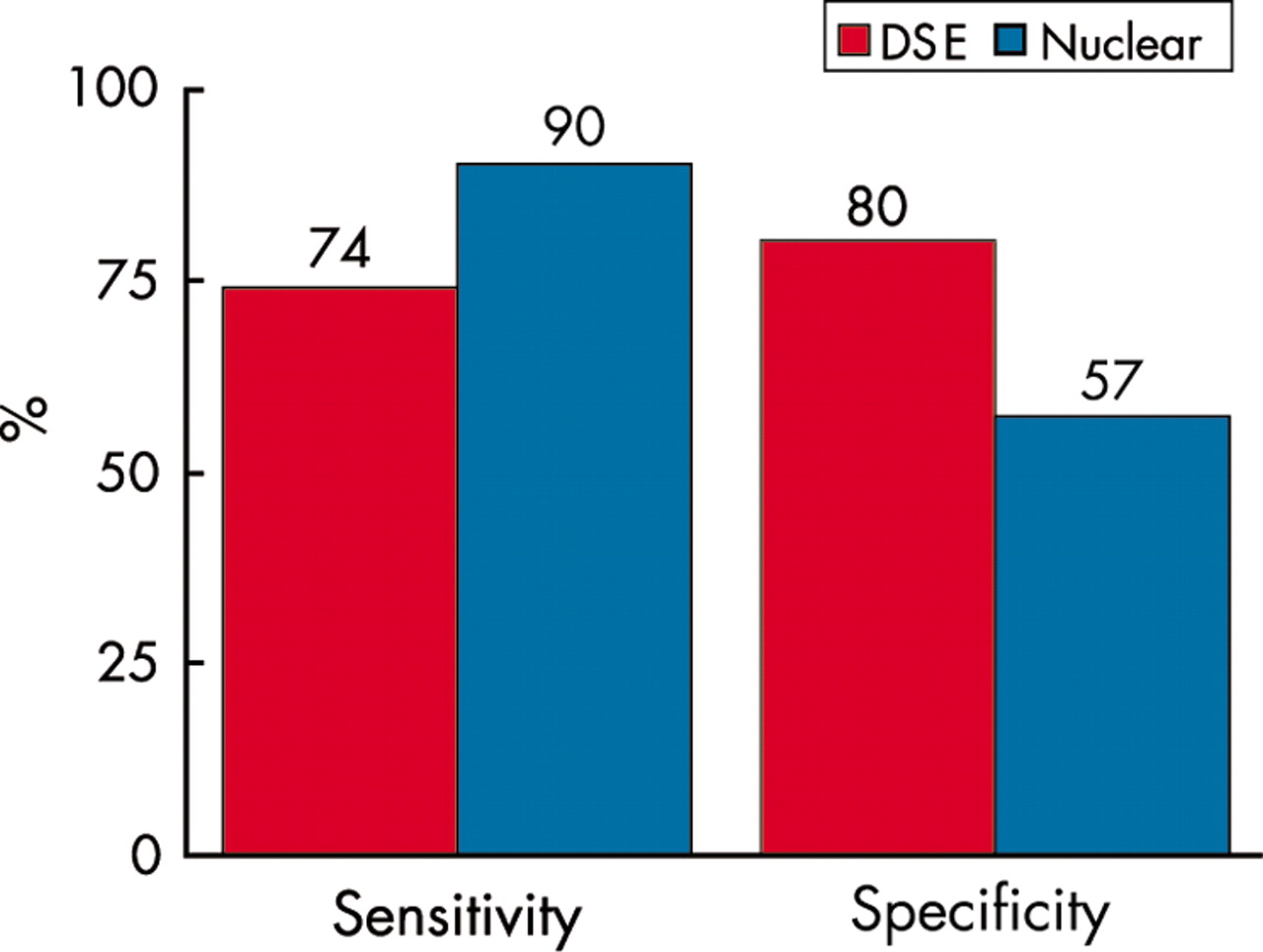
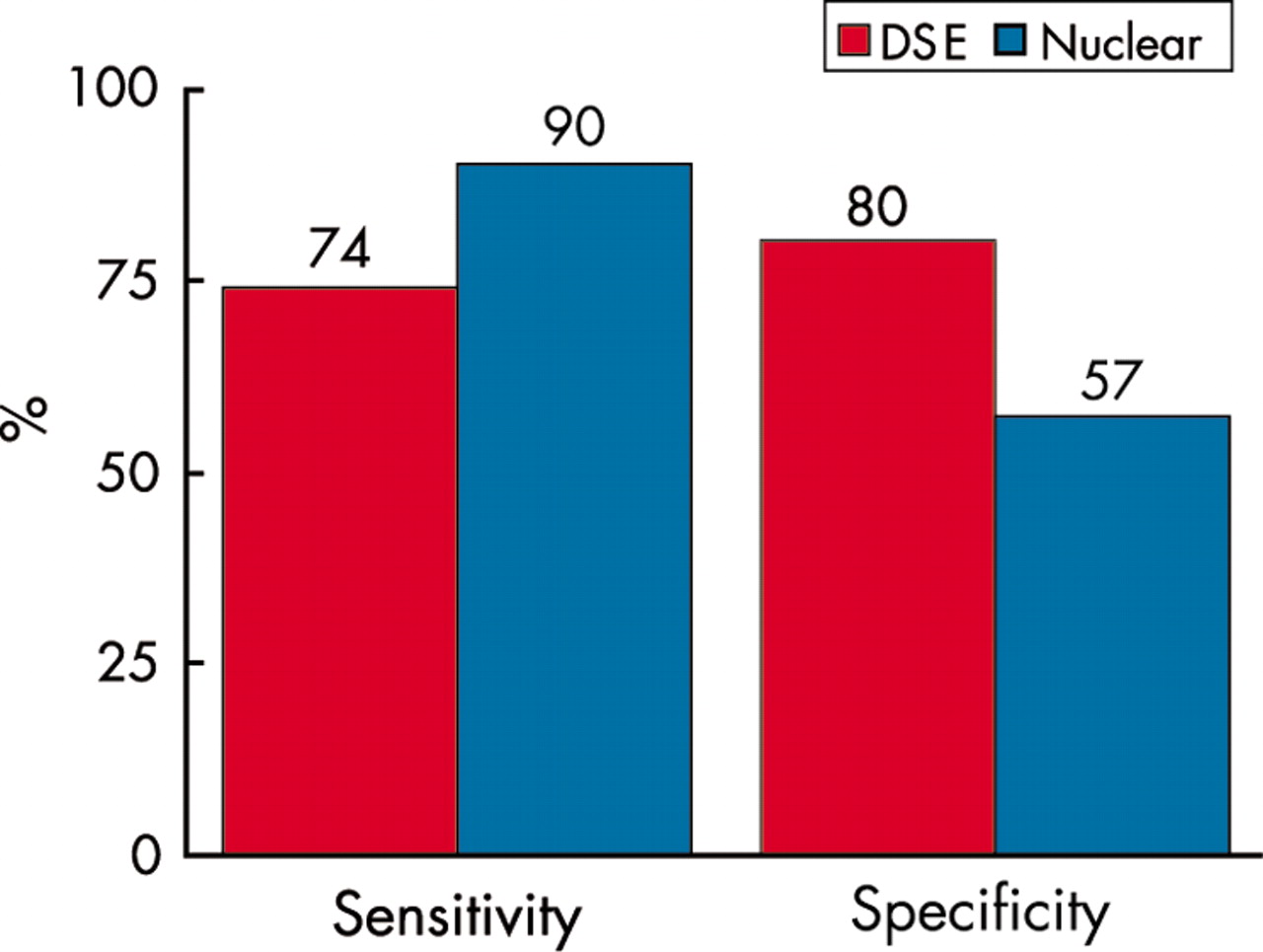
All the aforementioned techniques have been studied extensively, although most expertise has been obtained with dobutamine stress echocardiography and nuclear imaging. Pooled analysis of available data of the five most frequently used techniques to assess viability is summarised in table 2. In general, the nuclear imaging techniques appear to have a higher sensitivity for the prediction of functional recovery whereas stress echocardiography appears to be more specific.30 The difference between nuclear imaging and dobutamine stress echocardiography for the prediction of functional improvement after myocardial revascularisation is even more outspoken when only direct comparative studies are considered.30 Pooling of head-to-head comparisons underscores the differences in sensitivity and specificity of dobutamine stress echocardiography and thallium-201 SPECT (fig 5). The discrepancy between nuclear imaging and dobutamine echocardiography for the prediction of functional outcome after revascularisation may be related to different levels of ultrastructural cell damage in dysfunctional myocardium. The inotropic response during dobutamine stimulation may no longer be intact while more basal characteristics such as cell membrane integrity and glucose utilisation are still preserved. Based on these observations, nuclear imaging may be preferred in patients with depressed left ventricular ejection fraction and severely damaged myocardium.
Accuracy of non-invasive techniques to assess myocardial viability
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bar graph showing the sensitivity and specificity of dobutamine stress echocardiography and nuclear imaging to predict improvement of function post-revascularisation in patients with ischaemic cardiomyopathy. Data derived from Bax and colleagues30
How much viable tissue is needed for improvement of function?
The extent of improvement in global function is related to the extent of dysfunctional but viable tissue. Several studies have demonstrated that a certain amount of dysfunctional but viable tissue is needed for an improvement of global function following revascularisation. Usually a cut-off level of ⩾ 4 viable segments in a 16 segment model of the left ventricle is advised as a cut-off value to predict improvement of left ventricular ejection fraction.5 This cut-off value represents approximately 25% of the left ventricle, and may be used to identify patients who may benefit from revascularisation. However, this cut-off value of viable segments is to some extent artificial, because other factors also influence recovery of function. Recent data indicate that in patients with ischaemic cardiomyopathy and a mixture of viable and non-viable tissue, the extent of scar tissue should also be taken into account in order to predict accurately functional recovery after revascularisation.31 In addition, remodelling and enlargement of the left ventricle should also be considered. Remodelling of the left ventricle resulting in an enlarged end systolic volume may prevent global recovery, even in patients with substantial viability.32 Consideration of these issues and integration into a mathematical model may further improve patient selection for revascularisation.
Moreover, the surgical therapeutic options are developing rapidly, and myocardial revascularisation can now be combined with additional mitral valve repair to further optimise outcome. Also, resection of left ventricular aneurysms can be considered in the presence of extensive scar formation.
CONCLUSION
With the increasing number of patients presenting with ischaemic cardiomyopathy, assessment of myocardial hibernation and prediction of functional recovery after myocardial revascularisation have become common clinical issues. A number of non-invasive imaging techniques has been developed to identify hibernating myocardium. Although the ECG and resting echocardiogram may provide some initial clues on the presence/absence of viable myocardium, more sophisticated imaging techniques are usually needed. Both dobutamine stress echocardiography and nuclear imaging have been extensively used for the assessment of hibernating myocardium, and newer techniques such as MRI may further enhance the assessment of viability. Besides assessment of viability, additional factors need to be considered to allow precise prediction of outcome, including the presence and extent of scar tissue, the severity of remodelling of the left ventricle, and the presence of concomitant mitral regurgitation. Integrated information on all these issues will optimise patient selection for surgery, resulting in improved outcome and long term survival after revascularisation.
REFERENCES
Linked Articles
- Miscellanea
- Miscellanea