Article Text

Abstract
This glossary presents a comprehensive list of indicators of socioeconomic position used in health research. A description of what they intend to measure is given together with how data are elicited and the advantages and limitation of the indicators. The glossary is divided into two parts for journal publication but the intention is that it should be used as one piece. The second part highlights a life course approach and will be published in the next issue of the journal.
- health
- indicators
- social class
- social epidemiology
- socioeconomic position
Statistics from Altmetric.com
Socioeconomic position (SEP) is a commonly used concept in health research. Although researchers have an intuitive sense of what SEP means, the numerous ways of measurement indicate the complexity of the construct. A variety of other terms, such as social class, social stratification, social or socioeconomic status, are often used interchangeably despite their different theoretical bases and, therefore, interpretations. These issues have been discussed in detail by Krieger et al1 and we use SEP rather than socioeconomic status in line with their suggestion. “Socioeconomic position” refers to the social and economic factors that influence what positions individuals or groups hold within the structure of a society,1,2 and encompasses concepts with different historical and disciplinary origins, which will briefly be reviewed here. SEP is related to numerous exposures, resources, and susceptibilities that may affect health. This glossary presents a comprehensive list of indicators of SEP used in health research, together with a description of what they intend to measure, how data are elicited, and their main advantages and limitations. The glossary builds on previous work2–6 by providing updated information on the use and meaning of each measure, specifically in relation to epidemiological and health research.
There is no single best indicator of SEP suitable for all study aims and applicable at all time points in all settings. Each indicator measures different, often related aspects of socioeconomic stratification and may be more or less relevant to different health outcomes and at different stages in the life course. The choice of SEP measure(s) should ideally be informed by consideration of the specific research question and the proposed mechanisms linking SEP to the outcome. This is the case when SEP is the exposure of interest as well as when it is being considered as a confounding/mediating factor. If the central interest is to show the existence of a socioeconomic gradient in a particular health outcome then the choice of indicator may not be crucial. However, even in a case such as this, using different indicators of SEP may result in gradients of varying slopes. Furthermore, while a single measure of SEP may show an association with a health outcome, it will not encompass the entirety of the effect of SEP on health. This issue is of particular importance when SEP is a potential confounding factor. Multiple SEP indicators, preferably measured across the life course, will be needed to avoid residual confounding by unmeasured socioeconomic circumstances.7,12 The notion that the choice of SEP measure should be determined by the particular research question is exemplified by Snow’s work on exposures related to people working in the “offensive trades”.8,9 With respect to socially patterned exposures that have aetiological effects specific to particular stages of the life course it is clear that the socioeconomic indicators should relate to these life stages.10 Other researchers have emphasised the importance of theoretically grounded measures of social position in recent contributions.11 However, in practice, the measures used tend to be driven by what is available or has been previously collected. Even when a researcher cannot influence the particular SEP measure(s) available in a study, an understanding of their theoretical basis is important to making appropriate inferences.
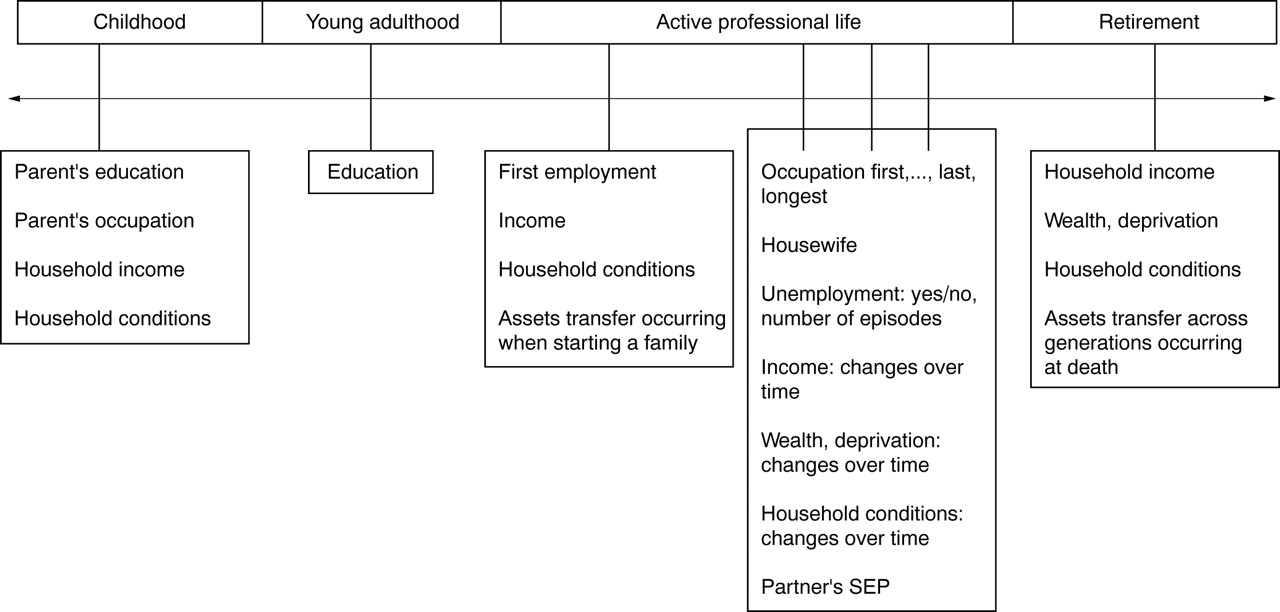
In this glossary we highlight the theoretical basis, measurement, interpretation, strengths, and limitations of each indicator. Where possible we present the interpretation or mechanism that may be of particular relevance to each indicator, but this is difficult because most of these indicators are strongly correlated. For example, despite education reflecting some particular aspects of SEP such as possession of a richer score of knowledge, it does, at the same time, help determine a person’s adult occupation and income, and therefore shares some of the health effects of these other indicators. This is particularly evident when a life course approach is considered (see fig 1 and part 2 of this glossary).
{kind=link}
Examples of indicators measuring life course socioeconomic position.
Most work on health inequalities has been conducted in developed countries and has generated indicators appropriate to this context. Further research is necessary to develop indicators that might be more appropriate in developing country settings. The glossary is organised such that individual level indicators are considered first, and within this they are presented in alphabetical order. Various forms of aggregate indicators (composite indicators and indices of area deprivation) follow. Finally, we briefly discuss life course SEP and multilevel approaches to considering SEP influences. The glossary is divided in two parts for journal publication, but the intention is that it should be used as one piece.
THEORETICAL ORIGINS
Many of the concepts underlying the use of SEP in epidemiological research have their origin in the work of two social theorists, Karl Marx and Max Weber. For Marx, SEP was entirely determined by “social class”, whereby an individual is defined by their relation to the “means of production” (for example, factories, land). Social class, and class relations, are characterised by the inherent conflict between exploited workers and the exploiting capitalists or those who control the means of production. Despite the palpable political weight of Marxist ideology in the 20th century we are aware of only two classifications used in epidemiological research that are based on Marx’s theory of social class, these are Erik Olin Wright’s classification13 and others developed in South America.14 In contrast with Marx, who viewed social stratification in capitalist societies as both source and outcome of the conflict between two necessarily opposed social groups, Weber’s theory suggests that society is hierarchically stratified along many dimensions, creating groups whose members share a common market position leading to shared “life chances”. For Weber, market position is not necessarily only defined by Marx’s class relations. For a more detailed summary of these sociological theories see Bartley.15
EDUCATION
Theoretical basis
Education is a frequently used indicator in epidemiology. The use of education as an SEP indicator has its historical origins in the status domain of Weberian theory,3 and it attempts to capture the knowledge related assets of a person.2 As formal education is normally completed in young adulthood and is strongly determined by parental characteristics, it can be conceptualised within a life course framework as an indicator that in part measures early life SEP.16,17
Measurement
Education can be measured as a continuous variable (years of completed education), or as a categorical variable by assessing educational milestones such as completion of primary or high school, higher education diplomas, or degrees. The continuous measure assumes that every year of education contributes similarly to a person’s attained SEP and that time spent in education has greater importance than educational achievements, whereas the latter assumes that specific achievements are important in determining SEP.3
Interpretation
Although education is often used as a generic measure of SEP, there are specific interpretations to explain its association with health outcomes3,18–20:
-
Education captures the transition from parents’ (received) SEP to adulthood (own) SEP and it is also a strong determinant of future employment and income.2,17 It reflects material, intellectual, and other resources of the family of origin, begins at early ages, is influenced by access to and performance in primary and secondary school and reaches final attainment in young adulthood for most people. Therefore it captures the long term influences of both early life circumstances on adult health, as well as the influence of adult resources (for example, through employment status) on health.17,21,22
-
The knowledge and skills attained through education may affect a person’s cognitive functioning, make them more receptive to health education messages, or more able to communicate with and access appropriate health services. A recent attempt to measure knowledge in terms of “cultural literacy” and assess its role in the association between education and health highlighted the great difficulty in trying to unpack some of the specific ways in which education and knowledge may affect health.23,24
-
Ill health in childhood could limit educational attendance and/or attainment and predispose to adult disease, generating a health selection influence on health inequalities.25
Strengths and limitations
Education is comparatively easy to measure in self administered questionnaires, garners a high response rate, and is relevant to people regardless of age or working circumstances, unlike many other SEP indicators.3 In addition, the collection of information on education may be less contentious in some contexts than other SEP indicators such as income.
The meaning of educational level varies for different birth cohorts. In addition to secular trends in improving educational attainment, there have been considerable changes in educational opportunities for women and some minority groups over recent decades. Such cohort effects can be important but are seldom accounted for in epidemiological studies. The results from studies that use years of education or educational qualifications that include participants from a number of different birth cohorts may be biased if cohort effects are not taken into account, because older cohorts will be over-represented among those classified as less educated.26 There are examples of how cohort effects have been accounted for in epidemiological studies. In one study the authors classified participants into low, medium, or high levels of education, these categories being defined with specific relevance to their birth cohort.16 This will help account for the fact that cohorts born earlier who have, in absolute terms, fewer years of education, may be classified in the same relative group of education than cohorts born later, despite these having greater absolute number of years of education. Another option is to stratify the analysis by age group, for example examining health inequalities by educational attainment within five year age groups.27 A further limitation of educational levels exists if individuals have obtained their education outside the country of residence—that is, in a different educational regime in which indicators of education may have very different implications than within the host country. Finally, measuring the number of years of education or levels of attainment may contain no information about the quality of the educational experience, which is likely to be important if conceptualising the role of education in health outcomes specifically related to knowledge, cognitive skills, and analytical abilities but may be less important if education is simply used as a broad indicator of SEP.
HOUSING TENURE, HOUSING CONDITIONS, AND HOUSEHOLD AMENITIES
Theoretical basis
Housing characteristics measure material aspects of socioeconomic circumstances. Housing based indicators are used in industrialised and non-industrialised countries, although the characteristics assessed differ. Moreover, these may be very specific to the area where they were developed. A recent glossary presents some of these indicators.28 We mention here those that are more directly related to SEP.
Measurement
The most commonly used characteristic is housing tenure—whether housing is owner occupied (owned outright or being bought with a mortgage), or rented from a private or social landlord. In rural populations ownership of a farm and farm size may better define housing characteristics.29
A number of household amenities are used in epidemiological studies, including access to hot and cold water in the house, having central heating and carpets, sole use of bathrooms and toilets, whether the toilet is inside or outside the home, having a refrigerator, washing machine, or telephone. These household amenities are markers of material circumstances and may also be associated with specific mechanisms of disease. For example, lack of running water and a household toilet may be associated with increased risk of infection.29,30 In addition the meaning of these amenities will vary by context and cohort (see the example of car access below). Very few people in contemporary advanced industrial societies will be without running hot water, indoor toilet or bathroom facilities and, therefore, some of these measures are not able to differentiate individuals in these populations. However, these indicators or other household amenities will have relevance in developing country populations (see below), and as indicators of childhood SEP in older adults in contemporary developed country populations (see for example their use in some articles12,31,32). One amenity that has proved to be a useful SEP indicator in the UK, but that has been used less in other populations, is car access.33–35 In rural areas of industrialised countries car ownership may not be a useful indicator of SEP as even the poorest households often own cars, out of sheer necessity.36 In non-industrialised countries, other assets that have been used as indicators of SEP in health related research include the number of livestock, owning a bicycle, refrigerator, radio, sewing machine, TV, or a clock.37–39
In addition to household amenities, household conditions such as the presence of damp and condensation, building materials, rooms in the dwelling, and overcrowding are housing related indicators of material resources. These are used in both industrialised and non-industrialised countries.40–43 Crowding is calculated as the number of persons living in the household per number of rooms available in the house (usually excluding kitchen and bathrooms). Overcrowding is then defined as being above a specific threshold (commonly two or more people per room). Overcrowding can plausibly affect health outcomes through a number of different mechanisms: overcrowded households are often households with few economic resources and there may also be a direct effect on health through facilitation of the spread of infectious diseases.
Recent efforts to better understand the mechanisms underlying socioeconomic inequalities in health have lead to the development of some innovative area level indicators that use aspects of housing. For example, a “broken windows” index measured housing quality, abandoned cars, graffiti, trash, and public school deterioration at the census block level in the USA.44 This indicator was more useful in explaining the variance in gonorrhoea rates than a poverty index that included income, unemployment, and low education. Similarly, an indicator of the “social standing of the habitat” combined characteristics of the building, their immediate surroundings and the local neighbourhood of residential buildings can be used to assign SEP.45 Concordance of this measure with education or occupation was good for people of either high or low socioeconomic position, but not for those with medium education and/or occupation, showing the heterogeneity of socioeconomic circumstances among people labelled as middle class.45
Interpretation
These indicators are mainly markers of material circumstances. Housing is generally the key component of most people’s wealth, and accounts for a large proportion of the outgoings from income. Housing (and its context) is an important, multifaceted and sometimes difficult to interpret indicator of SEP. As discussed above, some housing characteristics may be direct exposures or markers of exposures for specific diseases.
Strength and limitations
Housing characteristics and amenities are extensively used as measures of SEP. They are comparatively easy to collect and may also provide some indications of specific mechanisms linking SEP to particular health outcomes (for example, crowding). Their main limitation is that, although measuring the same underlying concept, these indicators may be specific to the temporal and geographical context where they were developed and thus be difficult to compare across studies.
INCOME
Theoretical basis
Income is the indicator of SEP that most directly measures the material resources component. As with other indicators such as education, income has a “dose-response” association with health,46,47 and can influence a wide range of material circumstances with direct implications for health.2,3 Income also has a cumulative effect over the life course48 and is the SEP indicator that can change most on a short term basis, although this dynamic aspect is rarely taken into account in epidemiological studies.49 It is implausible that money in itself directly affects health, thus it is the conversion of money and assets into health enhancing commodities and services via expenditure that may be the more relevant concept for interpreting how income affects health. Consumption measures are, however, rarely used in epidemiological studies.
Measurement
People can either be asked to report their absolute income or can be asked to place themselves within predefined categories. Most often income of the household rather than of individuals is measured. While individual income will capture individual material characteristics, household income may be a useful indicator, in particular for women, who may not be the main earners in the household. Using household income information to apply to all the people in the household assumes an even distribution of income according to needs within the household, which may or may not be true. For income to be comparable across households, additional information on family size or the number of people dependent on the reported income should be elicited.1 This can be then transformed into “equivalised income”,47,50 which adjusts for family size and its associated costs of living.3
Income may be measured as a relative indicator establishing levels of poverty (for example, percentage above or below the official poverty level in a given year48).
Interpretation
Income primarily influences health through a direct effect on material resources that are in turn mediated by more proximal factors in the causal chain such as behaviours. The mechanisms through which income could affect health are:
-
Buying access to better quality material resources such as food and shelter.
-
Allowing access to services, which may improve health directly (such as health services, leisure activities) or indirectly (such as education).
-
Fostering self esteem and social standing by providing the outward material characteristics relevant to participation in society.
-
Reverse causality may also be considered as income level can be affected by health status.
Strengths and limitations
Income is arguably the best single indicator of material living standards. There is evidence that personal income is a sensitive issue and people may be reluctant to provide such information,51 although this may have been overstated.52 In different settings (including different countries, different birth cohorts, different sexes) income may be a more or less “sensitive” indicator (with respect to participants’ willingness to disclose this information accurately) relative to educational attainment and occupation. Ideally we want to be able to collect disposable income as this reflects what individuals/households can actually spend, but often we collect gross incomes or incomes that do not take account of in-kind transfers that function as hypothecated income (such as food stamps in the USA). While income may be a sensitive question and potentially subject to greater non-response than other SEP questions, more sophisticated methods for eliciting accurate income information (especially for in-person interviews) have been developed, but of course these come at a cost of having to devote more space and time to collect these data. The meaning of current income for different age groups may vary and be most sensitive during the prime earning years. Income for young and older adults may be a less reliable indicator of their true SEP because income typically follows a curvilinear trajectory with age.
OCCUPATION BASED MEASURES
Theoretical basis
Occupation based indicators of SEP are widely used. Occupation can: represent Weber’s notion of SEP as a reflection of a person’s place in society related to their social standing, income and intellect; characterise working relations between employers and employees; or, less frequently, characterise people as exploiters or exploited in class relations.
Measurement
Most studies use the current or longest held occupation of a person to characterise their adult SEP. However, with increasing interest in the role of SEP across the life course, some studies include parental occupation as an indicator of childhood SEP in conjunction with individuals’ occupations at different stages in adult life.53 Occupational measures are in some sense transferable: measures from one individual, or combinations of several individuals, can be used to characterise the SEP of others connected to them. For example, the occupation of the “head of the household”, or the “highest status occupation in the household”, can be used as an indicator of the SEP of dependants (for example, spouse, children) or the household as a unit.
Interpretation
Different occupational classification schemes measure particular aspects of SEP, although it may be difficult to disentangle the specific effects of individual indicators. Some of the more general mechanisms that may explain the association between occupation and health related outcomes are presented here (for each classification we highlight the specific aspect it focuses on):
-
Occupation (parental or own adult) is strongly related to income and therefore the association with health may be one of a direct relation between material resources—the monetary and other tangible rewards for work that determines material living standards—and health.
-
Occupations reflect social standing and may be related to health outcomes because of certain privileges—such as easier access to better health care, access to education, and more salubrious residential facilities—that are afforded to those of higher standing.
-
Occupation may reflect social networks, work based stress, control, and autonomy and thereby affect health outcomes through psychosocial processes.
-
Occupation may also reflect specific toxic environmental or work task exposures such as physical demands (for example, transport driver, labourer).
Strengths and limitations
An important strength of these measures is their availability in many routine data sources, including census data and on death certificates. One of the most important limitations of occupational indicators is that they cannot be readily assigned to people who are not currently employed. As a result, if used as the only source of information on SEP, socioeconomic differentials may be underestimated through the exclusion of some of the population.54 Groups commonly excluded are retired people, people whose work is inside the home (mainly affecting women), the unemployed, students, and people working in unpaid, informal, or illegal jobs. Although previous occupation can be assigned to those who are retired and to some unemployed people, and husband’s occupation is often used to assign women’s SEP, this may inadequately index current social circumstances. Furthermore, other groups are less readily defined or willing to disclose their “occupation”. People who are self employed can be difficult to classify, for example it is unclear in some occupationally based classifications whether someone who is a self employed builder with a team of 20 workers working for her is classified as a manager or a skilled manual worker. Some contemporary classification systems (see part 2) operationalise the classification of the self employed in a more meaningful way.
As with education, occupation may have different meanings for different birth cohorts and in different geographical settings (which may make international comparisons problematic). For example, for older generations the allocation of a husband’s occupation to define a woman’s SEP may have been appropriate and acceptable, but this is unlikely to be the case for many contemporary working populations where the participation rates of women, and their expectations of recognition, are much higher. Cohort influences are also relevant in terms of the changing structure and composition of the workforce—in industrialised societies fewer contemporary school leavers go into unskilled or semi-skilled occupations, whereas computer or IT based occupations are increasingly common. Additionally, the exposure consequences of working in different jobs may change with the advent of stricter occupational health legislation and new technologies that eliminate toxic exposures.
The second part of the glossary continues by describing specific occupation based indicators.
REFERENCES
Footnotes
-
Funding: The work of JWL and GDS is supported (in part) by a Robert Wood Johnson Foundation Investigators Award in Health Policy Research. Funds from this award also partly support BG. MS is funded by the South West Public Health Observatory. DAL is funded by a UK Career Scientist Award. The views expressed in this paper are those of the authors and not necessarily any funding bodies.
-
Conflicts of interest: none declared.