Article Text

Abstract
Objective: To examine changes in the health of bar workers after smoke-free legislation was introduced.
Design: Longitudinal study following bar workers from before legislation introduction, at 2 months after introduction and at 1 year to control for seasonal differences.
Setting: Bars across a range of socio-economic settings in Scotland.
Participants: 371 bar workers recruited from 72 bars.
Intervention: Introduction of smoke-free legislation prohibiting smoking in enclosed public places, including bars.
Main outcomes measures: Change in prevalence of self-reported respiratory and sensory symptoms.
Results: Of the 191 (51%) workers seen at 1-year follow-up, the percentage reporting any respiratory symptom fell from 69% to 57% (p = 0.02) and for sensory symptoms from 75% to 64% (p = 0.02) following reductions in exposure, effects being greater at 2 months, probably partly due to seasonal effects. Excluding respondents who reported having a cold at either baseline or 1 year, the reduction in respiratory symptoms was similar although greater for “any” sensory symptom (69% falling to 54%, p = 0.011). For non-smokers (n = 57) the reductions in reported symptoms were significant for phlegm production (32% to 14%, p = 0.011) and red/irritated eyes (44% to 18%, p = 0.001). Wheeze (48% to 31%, p = 0.006) and breathlessness (42% to 29%, p = 0.038) improved significantly in smokers. There was no relationship between change in salivary cotinine levels and change in symptoms.
Conclusions: Bar workers in Scotland reported significantly fewer respiratory and sensory symptoms 1 year after their working environment became smoke free. As these improvements, controlled for seasonal variations, were seen in both non-smokers and smokers, smoke-free working environments may have potentially important benefits even for smokers.
Statistics from Altmetric.com
The adverse effects of second hand smoke (SHS) exposure on health are widely acknowledged. Prior to the introduction of smoke-free legislation in Scotland it had been estimated that between 1500 and 2000 non-smokers’ deaths per year in Scotland were attributable to SHS exposure.1 Occupationally exposed individuals are likely to be at greater risk and a recent analysis suggests that about 54 hospitality workers die every year in the UK as a result of their exposure to SHS.2 Legislation on reducing SHS exposure in public places is becoming more common worldwide3 with restrictions now in place in Ireland, Spain, Italy, Finland, Norway, parts of the United States, Scotland, England, Wales and Northern Ireland. The Smoking, Health and Social Care (Scotland) Act prohibited smoking in enclosed public and work places, including pubs, bars and restaurants, and came into force on 26 March 2006.4 Taking advantage of this natural experiment, funding was provided for a suite of studies on the effects of the smoking legislation on health,5 including a study of an occupationally exposed group, bar workers (The Bar Workers’ Health and ETS Exposure (BHETSE) study). From this study we have already shown that the smoke-free legislation resulted in an 86% reduction in airborne levels of PM2.5, a marker for second hand smoke, in Scottish pubs and bars,6 a similar reduction to that found in previous studies in Ireland7 and the USA.8 The BHETSE study has also reported results detailing the high level of bar workers’ support for the legislation both before and after the introduction of the ban and how this support increased in both smoking and non-smoking staff since it was implemented.9
Previous studies on the health effects of reducing SHS exposure have suggested rapid benefit in terms of symptoms and, perhaps more surprisingly, lung function. A study of 53 bar staff in San Francisco after smoking legislation was introduced in 1998 showed significant improvement in both symptoms and lung function after only a month,10 while the All Ireland Bar Study showed a 17% reduction in overall respiratory symptoms 1 year after legislation, which matched a fall in non-smoking bar workers’ salivary cotinine levels from 29 to 5.1 nmol/l.11 A study of 77 bar workers in Scotland also reported improvements in symptoms and lung function following the ban, but the study design and short follow-up period did not account for seasonality.12
We examined the effects of the Scottish smoke-free legislation on the health of 371 bar workers in a range of socio-economic areas in urban and rural Scotland, before and 2 and 10 months after enactment of the legislation. This paper reports the changes in self-reported respiratory and sensory symptoms of this group of bar workers.
METHODS
Study design
The BHETSE study was a prospective cohort study of bar workers. Workers were studied before the legislation was enacted (phase 1) and 2 months after (phase 2) and 1 year after the baseline measurements (phase 3) to allow for seasonality.
Recruitment
A total of 861 bars in designated postcode areas in three cities (Glasgow, Edinburgh and Aberdeen) and small towns (population <3000) in Aberdeenshire and the Borders area of Scotland were identified. These were situated in a broad range of socio-economic areas and consisted of different types of bars in urban, semi-urban and rural settings. Of these, 159 bars were randomly selected, contacted by telephone and invited to take part in the study. Bar managers who expressed interest were sent letters and other material describing the study to distribute to all their bar staff. Once permission was granted by bar managers, bar visits were conducted by a researcher at pre-arranged times to maximise the number of bar staff recruited at each visit. Of the 159 bars, 72 (45%) agreed to participate. We carried out convenience sampling between 7 January and 25 March 2006 of 371 bar workers (including managers, owners and bar staff) who were available and willing to take part at the time of our visits, across a range of weekday and weekend shift times. Participants were followed up on two further occasions between May and July 2006 and again between January and March 2007 either through work or, where an individual had left the original place of work, through their home, contact details having been taken at phase 1. The fieldwork was carried out by three researchers, one for each city, so that all measurements for a single individual were carried out by the same researcher.
Questionnaire
At all three visits participants completed a questionnaire (see supplementary file) based on that used in the All Ireland Bar Study,11 providing demographic details, smoking history, and health, exposure, days of sick leave in defined periods before each ban and attitudinal data. This allowed direct comparison with the Irish data.
Lung function
Spirometry was performed by one of three researchers using a Vitalograph Pneumotrac or Vitalograph 2120 spirometer (Vitalograph, Buckingham, UK) at each visit. The best of three reproducible values of FEV1 within 100 ml of each other was used as an acceptable blow. Later quality assurance on the traces to American Thoracic Society criteria13 using both flow volume and volume time curves resulted in exclusion of over 50% of the tests. In many cases this appeared to be due to reduced effort by bar staff at the 1-year follow-up point, similar to the experience from the Irish study (Clancy L, personal communication, September 2007) and so the lung function data were not analysed further.
Salivary cotinine
A non-stimulated sample of saliva was taken from each participant using a salivette (Sarsredt, Leicester, UK) following the protocol used for salivary cotinine measurement in the Scottish Health Survey. These surrogate exposure data have been reported elsewhere14 but are used here in validating each participant’s self-reported smoking status.
Statistical analysis
Analysis initially considered the entire occupational cohort concentrating on those who were available at both the baseline (phase 1) and 1-year (phase 3) time points. Data were then analysed for non-smokers and smokers at all three phases. Non-smokers were defined as those who reported being never or ex-smokers at both baseline and at 1-year follow-up and who had salivary cotinine levels of <20 ng/ml at both these time points. In the US population, the cut-off for non-smokers is 15 ng/ml,15 but given the higher exposure to SHS in bar workers,16 a level of 20 ng/ml as a cut-off was regarded as reasonable as used in the Irish bar study.11 Smokers were defined as those reporting either regular or current smoking and who had salivary cotinine levels >20 ng/ml. Ex-smokers were regarded as those with salivary cotinine levels of <20 ng/ml and who reported having stopped smoking for at least 6 months.
Changes in numbers having each symptom between occasions were assessed using McNemar’s procedure, that is, comparing the off-diagonals of a 2×2 table of matched counts against a null hypothesis of equality, with a two-sided alternative. Significance was assessed using exact binomial probabilities. The Wilcoxon–Mann–Whitney test was used to test whether the change in the median number of symptoms experienced was significant. As a small number of people did not answer every question relating to symptoms, the reported increases, decreases and p values for each question are based on those who answered that question either at both phase 1 and phase 2 or at both phase 1 and phase 3.
Ethics approval
The BHETSE study proposal was submitted for ethical review to the Grampian Research Ethics Committee whose chairman stated that the study did not require ethics approval. To provide a level of ethical assessment, an ethical review monitoring process was set up as part of the remit of the project Advisory Committee Group established by the funder, NHS Health Scotland. The committee considered the ethical aspects of the study on several occasions prior to field work commencing and were satisfied that there were no ethical problems with the study. However, we obtained written informed consent from all those who participated.
RESULTS
Reductions in airborne PM2.5 levels are reported in detail elsewhere6 but in summary fell by 86% from a mean of 246 μg/m3 (range 8–902 μg/m3) to 20 μg/m3 (range 6–104 μg/m3) between phases 1 and 2.
Overall, 371 individuals were seen and assessed at baseline and of these 266 were seen at phase 2 and 191 at phase 3. Table 1 shows the characteristics of those seen at both phase 1 and phase 3 (n = 191) compared to those seen only at phase 1 and phase 2 (n = 89) or at phase 1 only (n = 91). The mean age of all three groupings was less than 30 years, but those seen at both phases 1 and 3 were somewhat older than those who did not attend phase 3. There was also a higher proportion of young people lost to follow-up in Edinburgh than in Aberdeen or Glasgow, most likely due to Edinburgh having a more transient population of hospitality workers.
The pattern of those lost to follow-up by job was as expected; it was more likely that permanent bar staff and owners would be in the same job and thus be more easily contacted at follow-up, whereas temporary bar staff would be more likely to move on. Those seen both at phases 1 and 3 had also worked longer in bars generally and in the study bars specifically, reflecting both age and job differences. In other demographic respects those seen at both phases 1 and 3 were broadly representative of the whole cohort (table 1).
There were 57 consistent non-smokers who reported being non-smokers at both baseline and 1 year and had salivary cotinine levels of <20 ng/ml (table 2). Sixty five respondents were deemed to be consistent smokers in that they reported either regular or occasional smoking at both time points and had salivary cotinine values >20 ng/ml. The remaining 69 members of the cohort were classified as inconsistent smokers or were unclassifiable and were excluded from the analysis by smoking status.
Symptoms
Total cohort
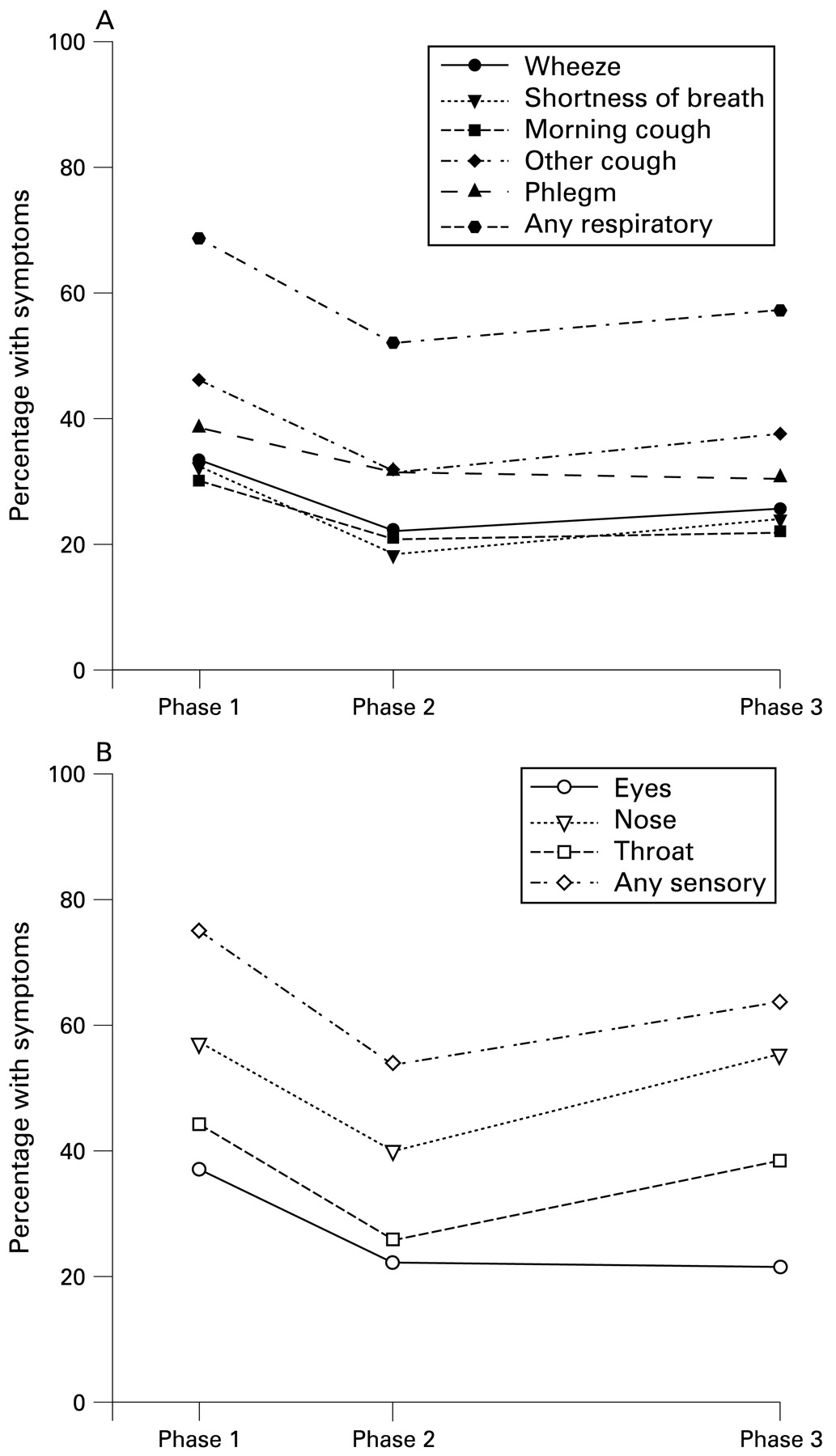
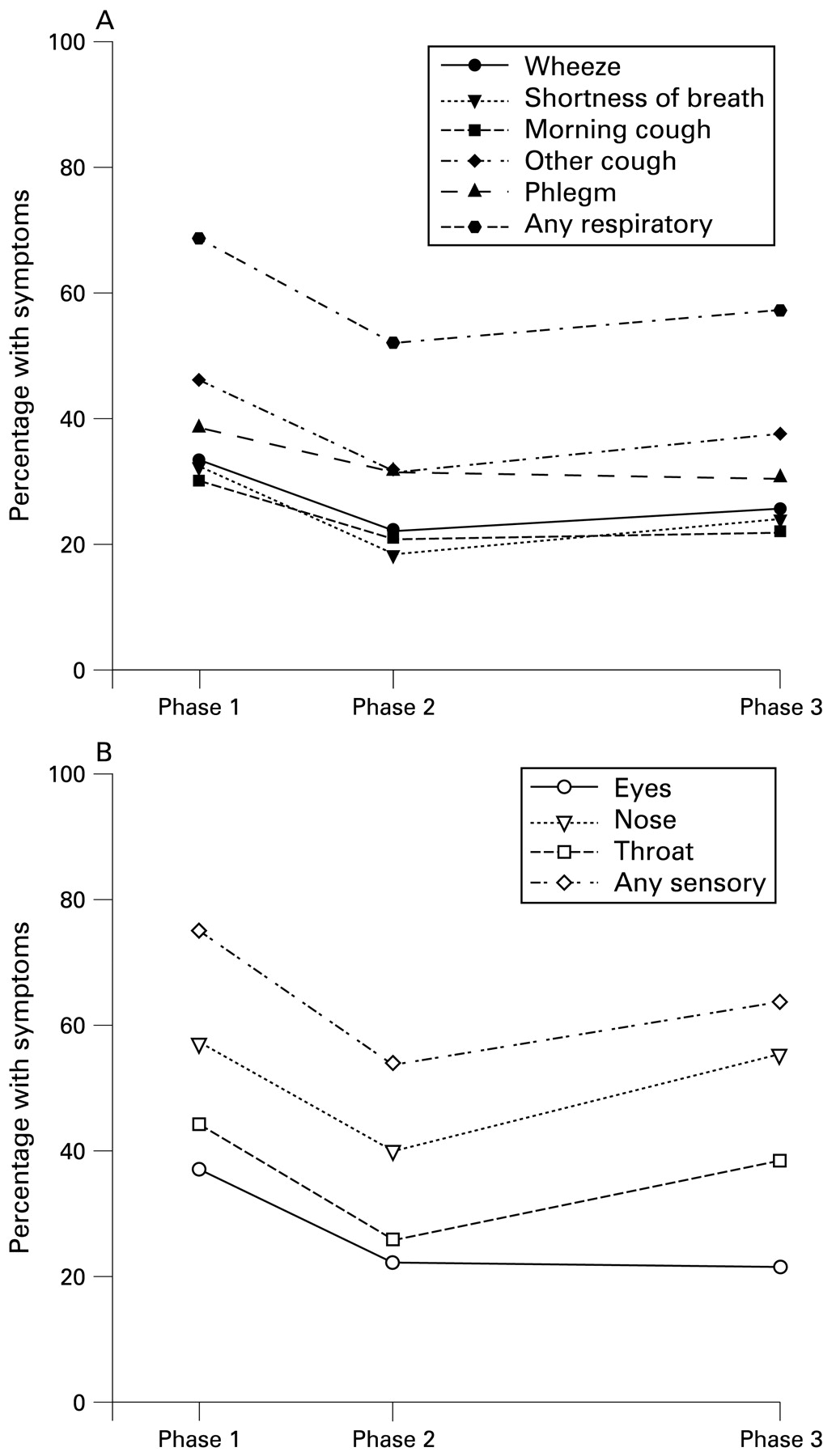
For the 177 individuals seen at all three phases, all symptoms were reduced at 2 months (fig 1), with a smaller difference from baseline in most symptoms at 1 year. When comparing responses in the 191 seen both at phases 1 and 3, all five respiratory and all three sensory symptoms showed reductions at 1 year (table 3A). The changes in all five respiratory symptoms and one of the sensory symptoms were statistically significant at the conventional 5% level.
{kind=link}
Changes in reported symptoms in 177 subjects seen at all three phases.
Effect of excluding participants with a current cold
When re-analysing those seen at both phases 1 and 3 and excluding those reporting a current cold at either baseline or 1 year (n = 191; table 3B), the pattern for reported respiratory symptoms was similar and reported sensory symptom improvement became more marked (any symptom: baseline 69% falling to 54%, p = 0.011; red/irritated eyes: 33% to 19%, p<0.001; throat sore or scratchy: 42% to 30%, p = 0.02).
Effect of smoking behaviour on symptoms
From 57 consistent non-smokers seen at both phases 1 and 3, the overall pattern was of improvement across all respiratory and all sensory symptoms (table 4A). The proportion of those reporting phlegm production reduced significantly (32% to 14%, p = 0.011) as did red/irritated eyes (44% to 18%, p = 0.001). When excluding those reporting a current cold at either baseline or follow-up from the analysis, the pattern of reducing symptoms was maintained and the reduction for several symptoms (morning cough and sore throat) approached statistical significance (table 4B).
Bar workers who were consistent smokers (n = 65) demonstrated baseline values of respiratory symptoms that were much higher than in the non-smoking group (any respiratory symptom at baseline: 85% vs 54%). However, levels of baseline sensory symptoms were similar (any sensory symptom at baseline: 75% vs 74%). Between baseline and follow-up smokers showed reductions in all five respiratory symptoms and in two of three sensory symptoms (table 5A). The only increase, in self-reports of a runny nose or sneezing, was minimal. There were large and statistically significant falls in the proportion of smokers reporting wheezing/whistling (48% to 31%, p = 0.006), shortness of breath (42% to 29%, p = 0.038) and red/irritated eyes (35% to 25%, p = 0.02). After removal of smokers who had a cold at either phase 1 or 3 (table 5B), the improvements were maintained although generally with reduced statistical significance.
Changes in symptoms were not related quantitatively either to baseline salivary cotinine or to change in salivary cotinine over time in a consistent manner.
While there was a trend for days lost from work and prescribed medication to reduce in the immediate period after the smoking ban, the changes were not statistically significant.
DISCUSSION
Main findings
These data show that for this group of bar workers reduction in exposure to SHS was associated with statistically significant reductions in both respiratory and sensory symptoms at 2 months after the ban was introduced, but that the improvements after 1 year were smaller, while remaining statistically significant (fig 1). However, the effects at 1 year were large, with reductions of 12% for respiratory symptoms (69% to 57%) and 11% for any sensory symptom (75% to 64%) (table 3A).
Effects of colds
We were aware of the potential effects season and infections could have on our study results and hence, in addition to our 1-year follow-up design, we have analysed our data after removal of those participants reporting a cold at either phase 1 or 3. Our results showed that there continues to be a pattern of improvements in respiratory health once this group was excluded, with some evidence of greater statistical significance despite fewer numbers of subjects (129 rather than 191). The results of excluding those with colds were similar for non-smokers and for smokers.
Clearly the overall symptom improvements found in the present study are not due to changes only in those with colds. The results suggest rather that colds, which are widespread in the population, may mask the extent to which reductions in SHS may lead to reduced respiratory and sensory symptoms. In this study, in multiple regression analyses (not reported here), the two main factors governing both respiratory and sensory symptoms were having recently had a cold and living with a smoker, with a suggestion that female gender might also play a role, women showing more sensory symptoms than males. In addition, the reporting of fewer infections by smokers than non-smokers may reflect different thresholds for symptom awareness. This highlights the importance, in this and in future studies, of identifying recent respiratory infections and developing approaches to deal with possible confounding from them.
We have not examined whether SHS exposure reduction would result in falls in rates of respiratory infections over time as this cannot be determined with accuracy over one season. However, one mechanism for health improvements in this context might be a less inflammatory, less pro-infective state induced by reduction in SHS exposure, and so there may be respiratory benefits in the longer term greater than have been shown here.
Smoking status
A previous study of Californian bar workers10 reported large, statistically significant, changes in self-reported respiratory and sensory irritation symptoms in the whole study group. Perhaps surprisingly, the improvements were shown in smokers as well as in non-smokers. The study has however been criticised for short follow-up (about 8 weeks) and small sample size (n = 53). The All Ireland Bar Study11 looked at a much larger cohort and followed these up over a full year, and reports the symptom improvements of non-smokers (n = 138). The BHETSE study was designed to examine changes in both smoking and non-smoking bar workers followed up 1 year after baseline. The effect of smoking behaviour on health improvements associated with the introduction of smoke-free legislation has not been previously explored on such a scale. Our study shows that smokers report improvements in their respiratory health to a similar degree to that experienced by non-smokers. It is possible that domestic environmental tobacco smoke exposure might have confounded these findings, although the difference in salivary cotinine levels between non-smokers living with a smoker and non-smokers not living with a smoker was small (means 3.85 and 4.1 ng/ml, respectively).
Given that the bar workers in the BHETSE study were more likely than the general Scottish population to smoke (54% v 27%), the evidence that smoke-free work places are associated with improvements in self-reported respiratory health has important implications for the health of this occupational group. The removal of exposure to SHS at work and/or the reduction in opportunity to actively engage in smoking may explain the health improvements experienced by smokers. As exposure to other peoples’ smoke has been suggested to be more toxic, on a mass for mass basis, than mainstream smoke,17 it is reasonable to postulate that reductions in exposure to SHS over a full working shift may lead to health improvements even among active smokers.
The finding of an association between the introduction of smoke-free work places and improvements in smokers’ health is also important in terms of analysing any health benefits that may accrue at a population level.
While data on work loss and medication were collected, there was no significant improvement in these health economic outcomes at 2 months although there was a trend to improvement. While the study was not powered to assess these indices over time, such outcomes would be important in determining the overall health benefit at a population level.
Comparison with other studies
Table 6 presents the results of changes in symptom prevalence for the 57 non-smokers in the BHETSE study alongside those of the 138 non-smokers from the All Ireland Bar Study11 and 53 mixed smokers/non-smokers from the Californian study.10 While the data both from the American study11 and from Dundee12 resulted from a follow-up spanning only 8 weeks, both the BHETSE study and the All Ireland Bar Study present changes over a longer 1-year period.
The prevalence of baseline symptoms in the All Ireland Bar Study is broadly similar to those reported by non-smokers in the BHETSE study; similarly, the magnitude of change seen at follow-up is comparable in both studies. The percentage improvements in symptoms in the smaller Californian study were much greater where baseline reported symptoms were considerably higher. It is possible that these differences might be explained by differing thresholds for reporting symptoms between the populations.
Seasonality
Baseline measurements had to be acquired in the winter, shortly before the introduction of the ban in March. In the UK, episodes of acute bronchitis are maximal in January,18 although Scottish surveillance data19 in primary care for the period of the study show acute consultations for respiratory illness in May 2006 to be broadly similar to those experienced in January 2006. However, this is not always the case and large seasonal differences in respiratory illness can occur in some years. It is safe to conclude that factors other than falls in exposure to SHS could contribute to reductions in self-reported respiratory and general sensory symptoms over the months from before to shortly after the introduction of the legislation, making it difficult or impossible to draw reliable conclusions about the effects of the legislation itself unless these other factors are controlled for either in study design or analysis. This seasonality was anticipated in the BHETSE study design, as it was in the All Ireland Bar Study, by undertaking follow-up measurements not only shortly after the legislation was introduced but also 1 year after the initial baseline, that is, at the same time of year. The earlier reported study on the Scottish ban12 did not address this issue of seasonality19 and thus the short-term benefits in lung function and symptoms reported there are likely to be over optimistic when considered in the light of 1-year follow-up data from this and the All Ireland Bar Study.11
Recruitment and attrition
We believe there was no significant recruitment bias in terms of socio-economic status and once agreement had been obtained from the bar managers, staff were generally happy to be involved in the study. Many bar staff are temporary, remaining in jobs for short time periods, although only 12 of the 191 workers seen at both phases 1 and 3 in this study described themselves as temporary. At the 2-month follow-up we made contact with 75% of the original cohort which fell to just over 50% at 1 year. This was better than we had expected but not as high as in the Irish study whose subjects had volunteered themselves to the study team, rather than being contacted and invited by the researchers. The demographic characteristics of those seen both at baseline and at 1 year were generally very similar to those who were lost to follow-up. Those included in the present analyses were slightly older, with longer experience as bar workers. This is unlikely to have introduced significant bias.
Main messages
Introduction of legislation to control smoking in public places significantly improves bar workers’ health in line with previous studies from other countries.
Symptom improvement at 1 year was less than at 2 months probably at least partly an effect of seasonality.
Effects were for the first time also seen in smoking bar workers who continued to smoke, suggesting a more important impact of environmental tobacco smoke in smokers.
Policy implications
The success of smoking control legislation is reinforced but also highlights that continuing active smokers may also benefit.
This suggests that more attention should be paid to the toxicity of environmental tobacco smoke at home given the concern that the smoking legislation might lead to smoking displacement into the home environment with children subsequently achieving higher exposures than before.
Self-report of symptoms
Our assessment of health changes is based on self-report of symptoms and not any objective measure of a biological parameter or physiological response. There is the possibility that participants were influenced in their responses to our questions by the publicity surrounding the legislation and health information provided by NHS Health Scotland, Cancer Research UK and other similar organisations detailing the health effects of exposure to SHS. This is likely to be true of any evaluation of smoke-free legislation, including the previous studies undertaken in Ireland and California. There, the reports of symptom improvements were supported by lung function measurements, showing that the apparent benefits to health were not due to (possibly subconscious) reporting biases. The present analyses of symptoms also provide some reassurance – although self-reports of symptoms generally showed improvements, it is interesting to note that the main sensory symptom that is most likely to be associated with a viral infection, namely having a runny nose and sneezing, showed no change from baseline to follow-up (47%) among our total cohort (on removal of those with a current cold). A population who were responding in a biased manner might be expected to also show decreased symptom prevalence for this question and this is perhaps an indication that participants’ responses were less prone to external influences than anticipated. The inadequacy of the lung function data especially at follow-up was also a problem in the Irish study and highlights the difficulties in acquiring reliable lung function data in an open work place in the presence of both workmates and customers.
Recommendations for future research
The BHETSE study is a large, longitudinal study of bar workers who have experienced a step-change in their exposure to SHS, one aspect of the study being that direct comparison could be made with the All Ireland Bar Study,11 and a similar evaluation study is now underway as part of work examining the effects of the English smoke-free legislation. However, this study was not designed for long term follow-up which, given the transient status of many bar workers, may be unfeasible. One of the benefits of this uniform protocol approach is that the data can be combined and similarities and differences between countries can be explored.
CONCLUSIONS
These data add to the knowledge on the short- to medium-term benefits to bar workers’ health of reductions in SHS exposure. This and other similar studies could not, and so did not, provide direct information on the health benefits over longer time scales. There is reason to suspect that the longer term benefits may be significant. The BHETSE study has confirmed substantial reductions in SHS; and sidestream smoke is 4 to 6 times more toxic than mainstream smoke on a mass for mass basis.17 In terms of health effects, it has long been recognised that exposure to SHS is associated with respiratory symptoms in children20 and an increased incidence of lung cancer21 and ischaemic heart disease22 in adults. There may be other health benefits. In particular, the consistent changes observed in a number of studies on bar workers around smoking bans suggest that airway inflammation due to SHS is a more important contributor to respiratory symptoms, and potentially the future development of chronic obstructive pulmonary disease, than had previously been thought.
In conclusion, our findings are very similar quantitatively to those found in the All Ireland Bar Study.11 Importantly, we additionally demonstrate marked improvements in the respiratory health of smokers at 1 year after the introduction of smoke-free work places, a finding that should be considered in future evaluations of the effect of smoke-free legislation. We have also shown the importance of allowing for reporting of respiratory infections in studies such as these where multiple environmental exposures can affect the outcomes.
Acknowledgments
We are extremely grateful to the bar staff and managers who took part in this study and to members of the BHETSE study Advisory Committee Group (Ms Sally Haw, Dr Colin Fischbacher, Professor David Hole and Dr Martie van Tongeren) for their help and contribution. We are very grateful to Shane Allwright who shared the Irish questionnaire on which ours was based to allow direct comparison of data.
REFERENCES
Supplementary materials
Web only appendix 66;5:339-46
Files in this Data Supplement:
Footnotes
Competing interests: None.
Funding: This study was funded by a grant from NHS Health Scotland. MP was funded by the Chief Scientist Office of the Scottish Executive Department of Health at the time the study was undertaken.
▸ Additional information is published online only at http://oem.bmj.com/content/vol66/issue5