Article Text

Abstract
Objectives Recent studies suggest that comprehensive smoking regulations to decrease exposure to second-hand smoke reduce the rates of acute myocardial infarction (AMI). The objective of this paper is to analyse if deaths due to AMI in Spain declined after smoking prevention legislation came into force in January 2006.
Design Information was collected on deaths registered by the Instituto Nacional de Estadística for 2004–2007. Age- and sex-specific annual AMI mortality rates with 95% CIs were estimated, as well as age-adjusted annual AMI mortality rates by sex. Annual relative risks of death from AMI were estimated with an age-standardised Poisson regression model.
Results Adjusted AMI mortality rates in 2004 and 2005 are similar, but in 2006 they show a 9% decline for men and a 8.7% decline for women, especially among those over 64 years of age. In 2007 there is a slower rate of decline, which reaches statistical significance for men (−4.8%) but not for women (−4%). The annual relative risk of AMI death decreased in both sexes (p<0.001) from 1 to 0.90 in 2006, and to 0.86 in 2007.
Conclusion The extension of smoke-free regulations in Spain was associated with a reduction in AMI mortality, especially among the elderly. Although other factors may have played a role, this pattern suggests a likely influence of the reduction in population exposure to second-hand smoke on AMI deaths.
- Public health
- preventive medicine
- health policy
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Using mortality data, this paper investigates if deaths due to acute myocardial infarction (AMI) declined country-wide as smoking prevention legislation came into force.
Key messages
The extension of smoke-free regulations in Spain was associated with a reduction in AMI mortality.
The magnitude of the reduction was similar in both genders, and greater among the elderly.
Although other factors may have played a role, this pattern suggests a likely influence of the reduction in population exposure to second-hand smoke on AMI deaths.
Strengths and limitations of this study
The use of secondary data (country-wide mortality statistics) is both a strength (as regards size) and a limitation (no information on individual characteristics beyond sex, age, vital status and cause of death).
The study is limited to a 4-year period because of confounding events in previous years.
Introduction
Smoking is known to be a causal factor for coronary heart disease, and both the consumption of cigarettes—even in small amounts—and exposure to second-hand smoke (SHS) are associated with acute myocardial infarction (AMI).1 Cigarette smoke, either mainstream or second-hand, can produce cardiovascular disease through a number of inter-related modes of action, including oxidative stress, haemodynamic and autonomic effects, endothelial dysfunction, thrombosis, inflammation, hyperlipidaemia and other mechanisms.2 Recent reviews of empirical studies performed after the introduction of regulations to reduce SHS exposure, have shown an associated decline in AMI.3–5 Using cause of death data, this paper analyses if the smoking prevention legislation implemented in 2006 in Spain was associated with a drop in AMI mortality.
Methods
This study is based on deaths registered by the National Statistics Institute (INE in its Spanish acronym) which since 1999 has provided data on causes of mortality, currently coded according to the 10th revision of the International Classification of Diseases (ICD-10). In addition to cause of death, the registry includes other variables such as place of residence, age and sex. These data are compiled and analysed, and statistics and reports are published periodically. The collected information is available for consultation and for studies.6
Deaths from 2004 to 2007 were selected. Data from previous years were not used because in 2003 Spain experienced a heat wave which caused an significant increase in mortality (6595–8648 excess deaths); the health effects of heat waves affect AMI and other circulatory conditions disproportionally, so this would distort the mortality pattern.7 8 The study included all deaths of Spanish residents over 34 years of age which were due to AMI (ICD-10: CM 055). Population estimates provided by the INE for each year were used as denominators (as estimates of the population at risk).9 Age- and sex-specific mortality rates were estimated for each year, with 95% CIs for comparisons.10 Besides stratified rates, directly adjusted rates were obtained with the Epidat 3.1 program, using the 2007 population as standard.11 The relative annual change in adjusted rates was estimated by dividing the rate difference (initial rate minus final rate) by the initial rate. Finally, to formally test the hypothesis that the regulatory change was associated with a decrease in mortality, age-standardised Poisson regression analyses were carried out using STATA 10.0 and annual relative risks and their 95% CIs obtained.
On 1 January 2006 tobacco advertisements were banned, the numbers of points of sale were reduced, and smoking was prohibited in workplaces (with exemptions for bars, cafes, restaurants, night clubs and discos) as the 28/2005 law came into effect. Previous regulations were limited, and compliance was variable.12 This law was widely covered by the media and was the subject of much public interest, and its actual implementation in workplaces (including shops and other enclosed public areas) was perceived as satisfactory.13
Results
Table 1 presents annual AMI deaths and mortality rates for the studied period by age and sex strata. The rates in 2004 and 2005 were essentially similar in both sexes. In contrast, there is a sharp decline in 2006, especially in age groups above 64 years. The confidence intervals of the total crude rates do not overlap for men or women. Comparing specific rates by age and gender, confidence intervals do not overlap for men in the age groups 65–69 years, 70–74 years and 75 and over, or for women above 74 years. There is also a decline in 2007, but it is small, although for men the confidence intervals for overall rates do not overlap, nor do those for the age group 65–69 years.
Deaths due to acute myocardial infarction (AMI) by age group and sex (rates per 100 000 population), by year, before and after the enforcement of regulatory changes in January 2006 (Spain, 2004–2007)
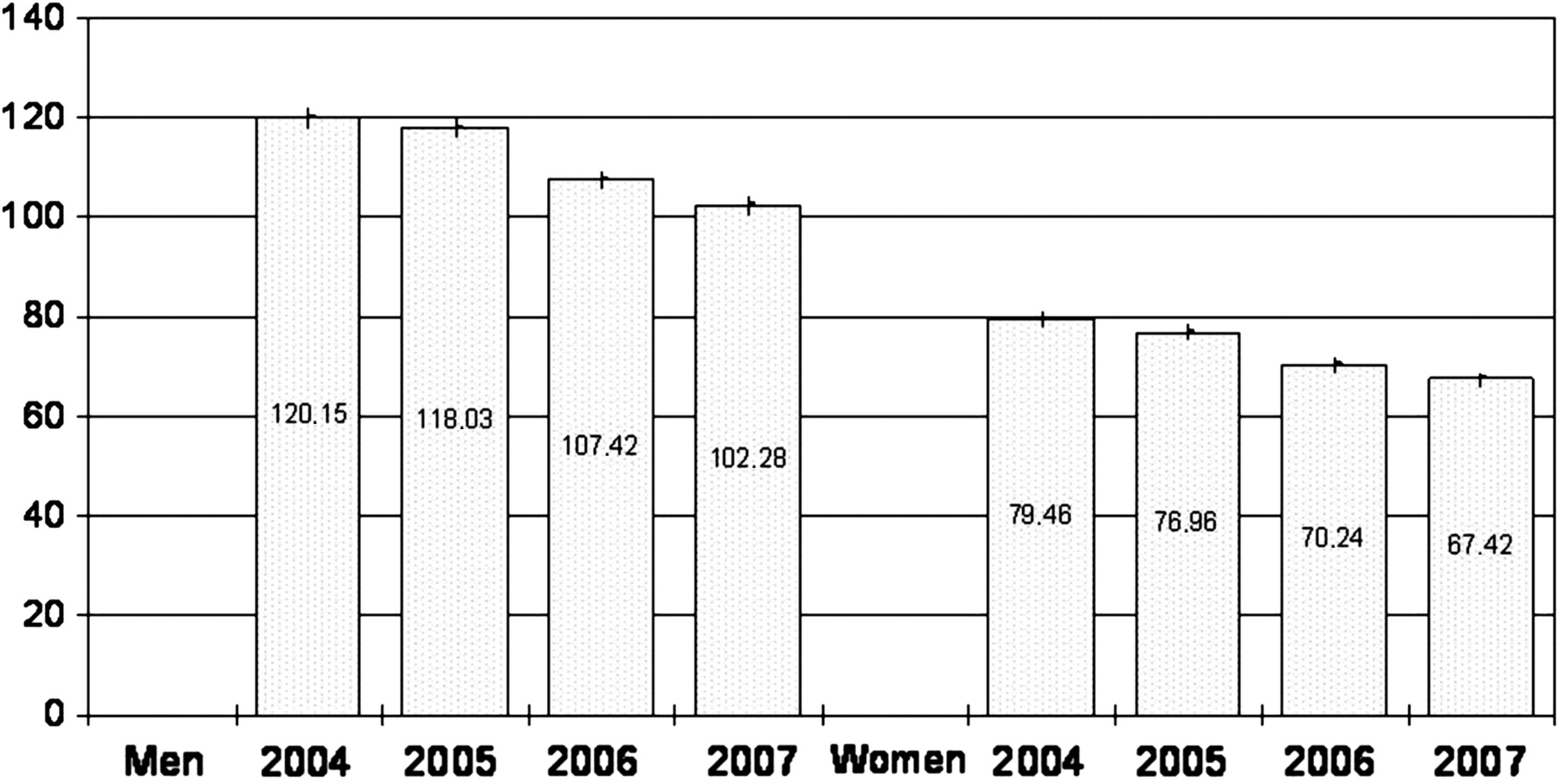
The age adjusted annual AMI mortality rates by sex are shown in figure 1, together with the annual relative change in rates. The rates in 2004 and 2005 were essentially similar in both sexes. In contrast, there is a sharp decline in 2006. In fact, mortality declines throughout the period, especially from 2005 to 2006 (−9% in men and −8.7% in women). From 2006 to 2007 the decline is less steep (−4.8% for men and –4% for women), although still higher than between 2004 and 2005.

{kind=link}
Evolution of annual adjusted mortality rates (per 100 000 population) due to acute myocardial infarction and 95% CIs, by sex, before and after the enforcement of regulatory changes in January 2006 (Spain, 2004–2007).
The results of the age-standardised Poisson regression model are shown in table 2. The 2004 and 2005 data are pooled and used as reference, in comparison with data after enforcement of the new regulations in January 2006. The relative risk figures show how the risk of death from AMI drops significantly for men, women and both sexes in 2006 (p<0.001), and declines further in 2007.
Annual age-standardised relative risk of death by acute myocardial infarction and 95% CIs after the January 2006 regulatory changes, by sex and year (Spain, 2004–2007)
Discussion
In 2006 there was a steep reduction in population-based AMI mortality rates in both sexes in Spain, after legislation banning smoking in indoor workplaces and many enclosed settings came into force in January 2006. The magnitude of the reduction (−8.7% in women and –9% in men) is comparable to that estimated in a previous study, which reported a reduction in AMI hospitalisations of 8.8% among women and 10.7% among men in the Barcelona metropolitan area in the first year after the 28/2005 law came into effect.14 It is also compatible with the effects estimated in general reviews.4 5 It is similar in magnitude for men and women, but for women the confidence intervals of the age-specific rates overlap, due to smaller figures as coronary heart disease is much less frequent among women than among men. There is a significant reduction in the relative risks of AMI death in both sexes after enforcement of the new regulation.
Most hospital-based studies do not report data by age, apart from three Italian studies and the studies from Scotland and England.5 15 Our results suggest that the magnitude of the reduction is greater among the elderly, as in Scotland and England.15 This is plausible, as the indirect evidence from studies of exposure to ambient particulate matter suggests that SHS may trigger acute coronary events in vulnerable myocardium, which should be more prevalent among the elderly.2 The three Italian studies found diverse results5: the Piedmont study suggested greater effects among women; in the Four Regions study the decline was concentrated among men 45–49 years old; in the Rome study (which added AMI deaths extracted from registries to hospitalisations) there were similar reductions for the 35–64 and 65–74-year-old age groups. These differences across studies could be due to different patterns of healthcare, as hospital-based studies reflect population events only if a similar proportion of cases reach the hospital for treatment across subgroups. Unlike the other Italian studies, the Rome study is practically a population-based study and its results are closer to those we found. In fact, as AMI death varies across age, younger patients are more likely to be hospitalised, while more elderly cases die before reaching hospital.16
These data suggest that previous estimates of the impact of SHS on mortality in Spain were somewhat conservative.17 When the 2005–2006 rate difference is applied to the reference populations, the number of AMI deaths avoided in the country over a year would be 1602 (1038 in men and 564 in women), after discounting the decline observed in 2004–2005, before the law came into effect.
The 28/2005 law imposes rigorous restrictions in indoor workplaces, with no options for ‘smoking rooms’, but has wide exemptions for bars and restaurants.18 Heavy SHS exposure was widespread before its enactment, and recent studies have shown important improvements in population exposure to SHS, both in perceived exposure and with environmental measures.12 13 19 20 Thus, the proportion of employed workers monitored in the SIVFRENT population-based surveillance system describing their job as smoke-free rose from 54% to 91% after enactment of the law.19 Environmental concentrations of nicotine decreased by an average of 97% in workplaces, and by 60–67% in healthcare or educational settings (where they were already low due to prior regulation).13 In addition, tobacco consumption has continued its decline, as shown both by cigarette sales data and by population surveys, but this process takes place cumulatively and is relatively small for any single year: the annual difference in daily smoking prevalence was estimated to be −0.57% for women and −1.15% for men around that time.21 22 Over the last few years there have been other relevant changes in the management of ischaemic heart disease and its risk factors, including increasing efforts to control high blood pressure, lipids or diabetes in primary care, fibrinolytic treatment of coronary episodes before hospitalisation, and increasing use of primary or secondary angioplasty.23 24 The development of these improvements has been gradual, and thus their effect would be incremental and unlikely as sudden as the reduction in mortality seen in 2006.23 In fact, the secular decline in ischaemic heart disease mortality has been estimated at an annual 1.30% for men and 1.19% for women.25 On the other hand, in 2007 the gains of the previous year are maintained and there is another reduction, although smaller; such a step effect would be compatible with a preventive effect concentrated in a short period and simultaneously reaching wide segments of the population and both genders, as would be expected from the wide implementation of a new regulation. Moreover, its size is huge as it covers the entire population.
This analysis is based on secondary data. The INE is a source of routine information, whose population base and comprehensiveness are strengths of this study. A limitation is the restricted time frame (4 years), caused by the epidemiological events of the summer of 2003. The denominators may be slightly overestimated, but this would not cause a differential bias as it would impact across the 4 years: the amount of immigration over this period caused changes, although mainly in younger age groups. Other limitations are the lack of a control site and the inability to assess the impact this regulation may have had on smoking cessation (although some data suggest that this would be rather small).5 21 Although these results should be confirmed with other studies, they suggest the regulation had a favourable impact, of a magnitude similar to that described in systematic reviews. Although we are not aware of comparable studies based on country-wide mortality data, they may be soon available in other countries which adopted smoking bans in recent years.26 In Spain, the expansion of these regulations under the 42/2010 law to the entire hospitality sector in January 2011 will bring new progress from a preventive perspective, reducing general SHS exposure and specially the risks to workers in this sector, whose high exposure to SHS has been documented.13
In conclusion, this study reports a steep reduction in population-based AMI mortality rates in both sexes in Spain, as a regulation banning smoking in indoor workplaces and in many enclosed settings was enforced. The reduction is comparable to that estimated in other studies based on hospital activity data. To the best of our knowledge, this is the first study based on national mortality statistics providing such evidence. The magnitude of their preventive effect in population terms emphasises the importance to public health of smoke-free policies.
Acknowledgments
The authors gratefully acknowledge the contribution of all members of the Barcelona Group for Smoking Regulation Policies Evaluation, whose discussions and work provided the framework on which this study was built, and especially thank Albert Espelt for his help in statistical analysis.
References
Supplementary materials
Supplementary Data
Files in this Data Supplement:
Footnotes
To cite: Villalbí JR, Sánchez E, Benet J, et al. The extension of smoke-free areas and acute myocardial infarction mortality: before and after study. BMJ Open 2011;1:e000067. doi:10.1136/bmjopen-2011-000067
Members of the Barcelona Group for Smoking Regulation Policies Evaluation include Josep Benet, Carmen Cabezas, Antonia Castillo, Montse Cleries, Albert Espelt, Alex Guarga, Rosa Martínez, Manel Nebot, Esteve Saltó, Emília Sánchez, Moisés Sualdea, Ricard Tresserras, Emili Vela and Joan R Villalbí.
Funding This work was supported partially with funds provided by the Centro de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP) to the Agència de Salut Pública de Barcelona for evaluative research in public health.
Competing interests None.
Contributors JRV conceived the study, collected secondary data, carried out the initial statistical analysis, and drafted the manuscript. EmS, EsS and CC wrote sections of the manuscript. All authors reviewed the manuscript and contributed to its final form. Albert Espelt performed the Poisson regression model.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Not applicable.