Article Text

Abstract
Regular physical exercise reduces cardiovascular morbidity and mortality. A small proportion of athletes, however, are at increased risk of exercise-related sudden cardiac death (SCD) as a result of quiescent cardiac anomalies. The preventable nature of such deaths has prompted the medical and sporting governing bodies to recommend preparticipation cardiovascular screening (PPS) in young athletes (⩽35 years) to permit the identification of potentially fatal disorders. Although evidence from the Italian experience suggests that electrocardiographic screening of young athletes has led to a significant reduction in SCD from cardiomyopathies, considerable controversy relating to the efficacy, cost-effectiveness and the impact of false-positive results of PPS still exists. This review presents an appraisal of all the available scientific evidence, attempting to resolve the concerns of the antagonists and examine how PPS compares with the World Health Organization screening criteria, providing compelling justifications for the implementation of universal PPS in young, competitive athletes.
Statistics from Altmetric.com
Regular physical exercise offers significant cardiovascular benefits.1 A small proportion of athletes, however, are at increased risk of exercise-related sudden cardiac death (SCD) as a result of quiescent cardiac anomalies.2 3 The death of an athlete is a highly emotional event given the youth of the individual and the potential number of life years lost. The counterintuitive nature of such deaths intensifies the media attention and astounds communities around the globe because young athletes are considered to represent the healthiest segment of our society. The steady trickle of sudden death in some high profile athletes has prompted the medical and sporting governing bodies to recommend preparticipation cardiovascular screening (PPS) in young athletes (⩽35 years) to permit the identification of potentially fatal disorders.4 5 6 7 8 Indeed, the role of PPS is magnified when one considers that SCD in athletes can be prevented through simple lifestyle modifications, pharmacotherapy, or the implantation of an internal cardiovertor defibrillator. There is, however, considerable controversy relating to the efficacy, cost-effectiveness and the impact of false-positive results of PPS. This article presents an appraisal of all the available scientific evidence, providing compelling justifications for the implementation of universal PPS in young, competitive athletes.
Epidemiology and pathogenesis of SCD in athletes
Current data indicate a strong predilection to SCD in relation to sporting discipline, gender and age. The largest numbers of deaths are reported in soccer and basketball, but this could be attributed to the popularity of these sports. There is a striking male predominance (male to female ratio 9 : 1), with higher participation rates providing part of the explanation.2 There is an upward trend in the incidence of SCD with increasing age; the incidence of SCD in Rhode Island joggers, in whom the mean age of the athletes was well over 35 years was 13 per 100 000 per year.9 In contrast, studies in younger athletes have reported significantly lower rates. In Italy, a prospective population-based observational study reported an incidence of 2.1 per 100 000 per year in athletes aged 14–35 years.2 In the USA a retrospective review of high school athletes aged 15–17 years reported an incidence of 0.5 per 100 000 per year.10 The lower incidence of SCD in the USA may reflect a geographical variation; however, results are probably also influenced by the retrospective study design, the younger age group and the higher proportion of female athletes (35% vs 18%) in the American series compared with the Italian study.
A broad spectrum of congenital, inherited and acquired cardiovascular diseases cause SCD. There is a strong correlation with age, with coronary artery atherosclerosis accounting for the majority of deaths in athletes aged over 35 years. In younger athletes inherited cardiomyopathies are more prevalent (fig 1).

Causes of sudden cardiac death in young athletes.
The objective of PPS in athletes and current practices
The primary objective of PPS is to identify unsuspected cardiovascular disease and prevent SCD in athletes by appropriate intervention. Both the American Heart Association (AHA) and European Society of Cardiology (ESC) agree that there are compelling justifications to provide PPS to protect athletes. Intense debate exists, however, relating to the protocols used.4 5
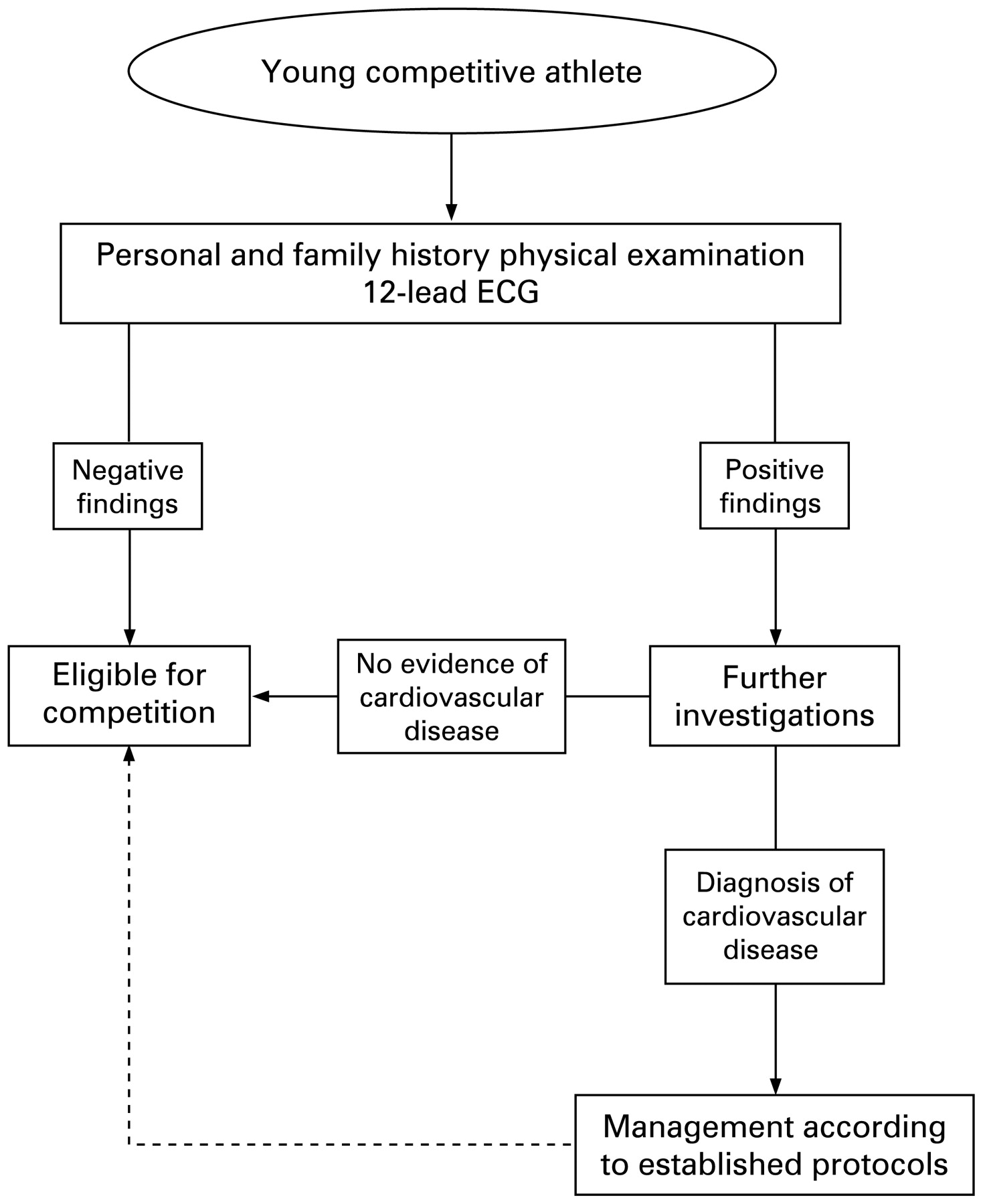
In the USA the AHA guidelines recommend PPS utilising a health questionnaire and physical examination, with a 12-point screening protocol (box 1). In Italy a unique state-sponsored, national PPS programme has been in operation for over 25 years, evaluating several million young athletes annually. Each athlete is subject to annual screening consisting of history, examination and 12-lead electrocardiogram (ECG) (fig 2). Athletes with abnormalities on initial evaluation are investigated further and those identified with potentially serious cardiovascular abnormalities are disqualified.

Flow diagram of the Italian preparticipation screening protocol endorsed by the International Olympic Committee, Federation of International Football Associations, Union of European Football Associations and the European Society of Cardiology. ECG, electrocardiogram.
Box 1 The 12-point AHA recommendations for PPS of young competitive athletes
Medical history*
Personal history
1. Exertional chest pain/discomfort
2. Unexplained syncope/near-syncope†
3. Excessive exertional dyspnoea/fatigue
4. Previous recognition of a heart murmur
5. Elevated systemic blood pressure
Family history
6. Premature death (<50 years) due to heart disease, in one or more relative
7. Disability from heart disease in a close relative less than 50 years of age
8. Specific knowledge of certain cardiac conditions in family members: hypertrophic and dilated cardiomyopathy, long-QT syndrome or other ion channelopathies, Marfan syndrome or clinically important arrhythmias
Physical examination
9. Heart murmur‡
10. Femoral pulses to exclude aortic coarctation
11. Physical stigmata of Marfan syndrome
12. Brachial artery blood pressure (sitting position, taken in both arms)
*Parental verification is recommended for high school and middle school athletes. †Judged not to be vasovagal; of particular concern when related to exertion. ‡Auscultation should be performed both supine and standing or with the Valsalva manoeuvre, specifically to identify murmurs of dynamic left ventricular outflow tract obstruction.
How effective is the ECG in identifying potentially fatal cardiovascular abnormalities in athletes?
The definitive diagnosis of cardiomyopathies is dependent on cardiac imaging. It is well recognised, however, that 95% of individuals with hypertrophic cardiomyopathy (HCM) and 80% of individuals with arrhythmogenic right ventricular cardiomyopathy (ARVC) exhibit electrocardiographic abnormalities.11 12
The efficacy of the ECG in the identification of cardiomyopathies has been established in a large population-based study of screening outcomes in 33 735 young athletes in the Veneto region of Italy. Of the 621 (1.8%) athletes disqualified due to the identification of a cardiovascular disorder, 22 (0.07%) were identified with HCM, based predominantly (73%) on an abnormal ECG.13 This frequency is similar to that observed in a population-based study in the USA, using echocardiography, suggesting that the Italian screening model performs as well as echocardiography in detecting HCM.14 The specificity of the 12-lead ECG-based Italian PPS programme in excluding the diagnosis of HCM has also been assessed in a study of 4450 elite athletes initially judged eligible for competition post-PPS. All athletes underwent echocardiographic examination to assess previously undetected HCM. After an average 8-year follow-up period, HCM was diagnosed in only one (0.02%) athlete, indicating that a normal ECG has a high negative predictive value (99.98%) excluding HCM in almost all athletes.15 More recent experience from the Italian PPS suggests that 12-lead ECG screening is also effective in identifying individuals with ARVC.16
The ECG is also the gold standard basic investigation for detecting potentially fatal conduction disorders such as Wolf–Parkinson–White syndrome and ion channel diseases including the Brugada syndrome, Lenegre’s disease and long-QT and short-QT syndrome.
Does ECG screening reduce the number of SCD in athletes?
Whereas HCM is the commonest cause of exercise-related SCD in the USA, it is responsible for a much smaller proportion of deaths in Italy. Although the antagonist could argue that this observation may reflect a lower genetic cluster of HCM in the Mediterranean region, these figures probably reflect the efficacy of the Italian programme in identifying athletes with HCM and minimising deaths through disqualification from sport; none of the 22 athletes identified with HCM in the Veneto region between 1979 and 1996 died during a mean follow-up period of 8.2 years. Of the 49 deaths recorded among young athletes during the same period, only one was attributed to HCM (2%), which is much lower than the incidence of 7.3% recorded in 220 SCD among non-athletes.13
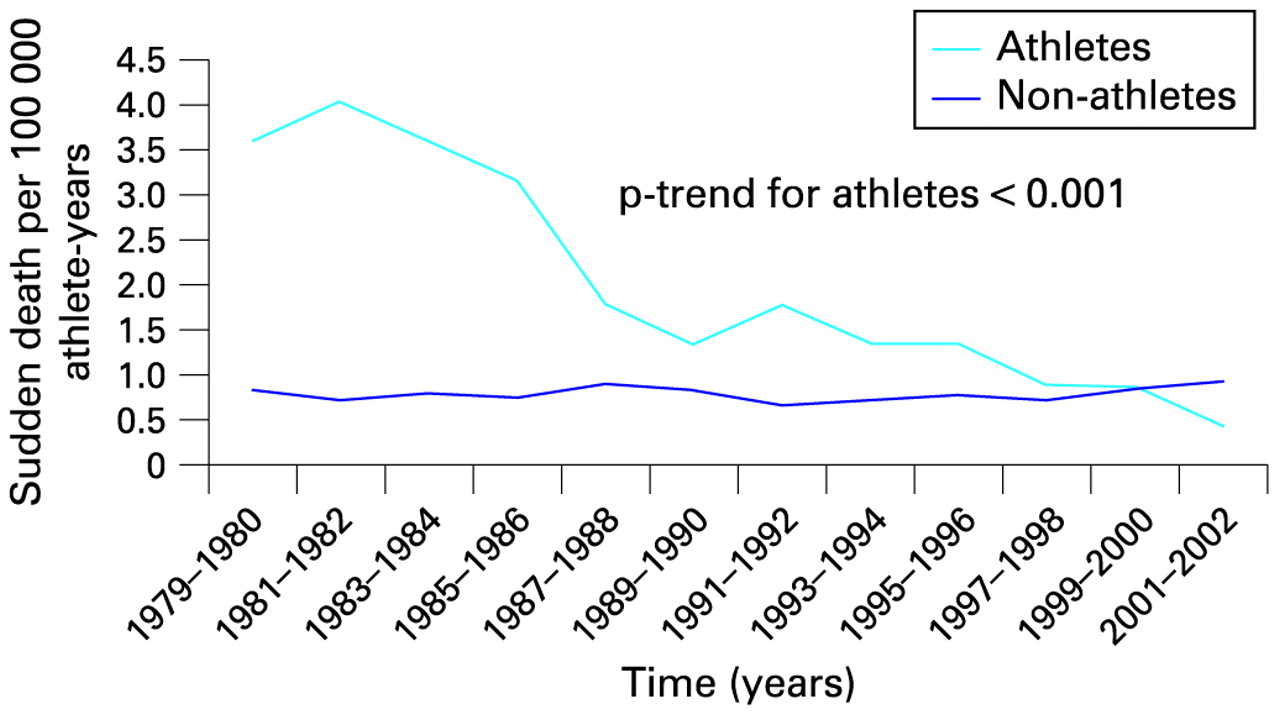
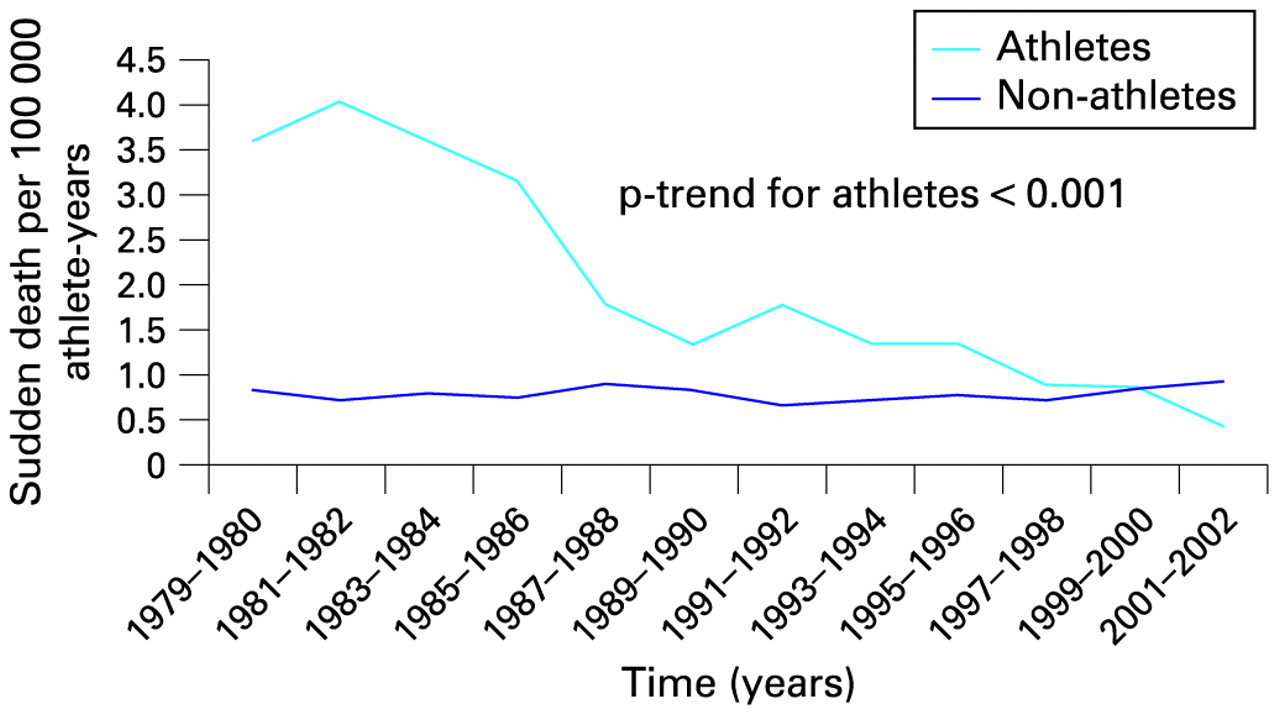
The most compelling evidence that the Italian PPS model reduces the incidence of SCD in sport is derived from a subsequent prospective study by the same group comparing the incidence of SCD between the prescreening era and a 25-year period of screening, which showed a reduction in the incidence rate of SCD from 3.6/100 000 person-years pre-screening to 0.4/100 000 person-years in 2003–4. These figures represent a 90% reduction in mortality since the implementation of PPS and are predominantly due to fewer cases of SCD from cardiomyopathies, particularly ARVC, which was a relatively novel entity and failed to be detected in the early screening era (fig 3).16
{kind=link}
{kind=link}
{kind=link}
Annual incidence rates of sudden cardiovascular death in screened competitive athletes versus non-athletes in the Veneto region of Italy (1979–2004).16
What are the limitations of 12-lead ECG as a screening tool?
In keeping with other screening tests, the ECG cannot identify all athletes at risk of SCD. In particular, it fails to identify athletes with atherosclerotic coronary artery disease and congenital coronary anomalies, and given the high prevalence of unsuspected atherosclerosis in athletes aged over 35 years, its efficiency is limited in the older age group. Indeed, ECG screening alone in older athletes has the potential for a large number of false-negative results and is not recommended by the authors.
Box 2 Common ECG changes in the athlete that should be regarded as part of the normal physiological adaptation to exercise
Sinus bradycardia
Sinus arrhythmia
First-degree atrioventricular block
Incomplete right bundle branch block
Early repolarisation pattern
Isolated voltage criteria for left ventricular hypertrophy
Concerns regarding ECG screening in young athletes relate predominantly to the potential number of false-positive tests mandating unnecessary investigations or even the false disqualification of athletes. Physical conditioning is associated with ECG changes that comprise part of the “athlete’s heart” and may overlap with those observed in cardiomyopathies.17 Therefore, PPS should be performed by expert cardiologists or other physicians with an interest in the cardiovascular adaptation to exercise as well as knowledge specific to the broad phenotypic manifestations of inherited cardiac diseases with the propensity to cause SCD. Two large prospective observational studies performed in Italy revealed that although ECG changes commonly associated with athletic activity (box 2)18 were present in almost 12% of young athletes, the false-positive rate of athletes with ECG abnormalities requiring further cardiovascular assessment before being allowed to compete (box 3) did not exceed 7% and was as low as 4%.13 19 The authors’ experience of screening highly trained athletes in the UK, using the Italian model, indicates a false-positive rate of 3.7% using history, physical examination and ECG, with only 1.9% of false-positives determined by ECG alone.20
Box 3 Criteria for a positive 12-lead ECG requiring further investigations according to the ESC consensus statement
P-wave
Left atrial enlargement: negative portion of the P-wave in lead V1 ⩾0.1 mV in depth and ⩾0.04 s in duration.
Right atrial enlargement: peaked P-wave in leads II and III or V1 ⩾0.25 mV in amplitude.
QRS complex
QRS axis deviation: right ⩾+120° or left −30° to −90°.
Increased voltage: amplitude of R or S-wave in a standard lead ⩾2 mV, S-wave in lead V1 or V2 ⩾ 3 mV or R-wave in lead V5 or V6 ⩾3 mV.
Pathological Q-waves: ⩾0.04 s in duration or ⩾25% of the height of the ensuing R-wave or QS pattern in two or more leads.
Right or left bundle branch block with QRS duration ⩾0.12 s.
R or R′-wave in lead V1 ⩾0.5 mV in amplitude and R/S ratio ⩾1.
ST-segment, T-waves, and QT-interval
ST-segment depression or T-wave flattening or inversion in ⩾2 leads.
Prolongation of heart rate corrected QT interval >0.44 s in males and >0.46 s in females.
Rhythm and conduction abnormalities.
Premature ventricular beats or more severe ventricular arrhythmias.
Supraventricular tachycardias, atrial flutter or atrial fibrillation.
Short PR interval (<0.12 s) with or without “delta” wave.
Sinus bradycardia with resting heart rate ⩽40 beats/minute*
First (PR ⩾0.21 s†), second or third degree atrioventricular block
*Increasing less than 100 beats/minute during limited exercise test. †Not shortening with hyperventilation or limited exercise test.
Failure to consider the impact of age and ethnicity on the ECG may be a source of false-positive results because most data in athletes are derived from white adult athletes and should not be extrapolated to other populations. The ECG is affected by the physical maturity of the athlete, and adolescent athletes often exhibit T-wave inversions in the right precordial leads (V1–V4), similar to ARVC, which are considered to represent the normal juvenile ECG pattern. Recent data, from our group, based on the evaluation of 1710 highly trained, predominantly white, adolescent athletes reveal that 4% of adolescent athletes exhibit significant T-wave inversions, with 2.5% present in the right precordial leads. T-wave inversions in the right precordial leads, extending beyond lead V2, were almost confined (85%) to individuals under 16 years of age. Detailed evaluation of such athletes with echocardiography, cardiac magnetic resonance imaging, 24-h ECG, exercise stress test and evaluation of their first-degree relatives failed to identify any evidence of ARVC or other cardiomyopathies in these athletes. Therefore, in asymptomatic white adolescent athletes aged less than 16 years the presence of T-wave inversions in leads V1–V4 should not justify further investigations in the absence of symptoms or a family history of premature heart disease or SCD.21 In contrast, T-wave inversions beyond V2 are uncommon (0.1%) in white athletes aged 16 years and older and their rarity probably warrants further investigation. Such considerations and appropriate adjustment of the recommended ESC 12-lead ECG criteria for further detailed evaluation could reduce the false-positive rate to as low as 2%.21
There is emerging evidence that racial factors have a significant impact on the physiological adaptation to exercise in athletes of African/Afro-Caribbean origin.22 23 Current data reveal that up to a third of black athletes exhibit marked repolarisation anomalies consisting of convex ST-segment elevation and deep T-wave inversions that are usually limited to the right precordial leads (V1–V4).24 25 The implementation of PPS in countries with a large proportion of black athletes may prove problematical and result in a high number of false-positive tests. Our experience, however, suggests that black athletes with such abnormalities in leads V1–V4 do not exhibit echocardiographic evidence of cardiomyopathy and subsequent follow-up of these athletes has not revealed any cardiac morbidity or mortality, indicating that the electrical anomalies observed in a high proportion of black athletes represent ethnic variants rather than cardiac pathology. Adjustment of the ESC criteria by taking the aforementioned changes into consideration reduces the false-positive rate, relating to ECG repolarisation anomalies, to 3% and should not pose a barrier to the implementation of PPS. In black athletes the criteria for pathological left ventricular hypertrophy include T-wave inversions in the inferior and/or lateral leads, particularly with concomitant ST-segment depression in the affected leads or, associated with voltage criteria for left atrial enlargement, pathological Q-waves and left axis deviation.24 25
What is the psychological impact of PPS?
There is a paucity of published data on the psychological impact of PPS in athletes. Studies on established screening programmes indicate that individuals with a false-positive result may experience considerable anxiety until further investigations provide reassurance, which highlights the need for the prompt evaluation of athletes who fail the initial screening. Trepidation over long-term psychological scarring of athletes with an initial false-positive result requiring further detailed investigations is not justified, because evidence from the same studies suggest that in the context of a well-organised screening programme with expert psychological support there is no significant long-term psychological burden.26 27
Diagnosing a young athlete with a potentially life-threatening condition and excluding the individual from competition may be associated with profound physical, social and psychological consequences and preclude the potential for lucrative gain. However, such corollaries may be considered relatively trivial when contrasted with the devastating impact of the SCD of a young, asymptomatic, highly trained individual.
What is the economic impact of PPS?
Current data concur that a PPS programme in young athletes utilising 12-lead ECG can be cost-effective. A cost-effectiveness analysis of a prospective observational study of 5615 high school athletes in the USA compared history and examination only, with the use of additional 12-lead ECG (assuming that 10% of the athletes identified as being at risk would live an additional 40 years and 90% an additional 20 years). The study revealed that the ECG was more cost-effective costing US$44 000 per year of life saved compared with the cost of history and examination alone, which was estimated at US$84 000 per year of life saved.28 29 An Italian cost-effectiveness analysis of 33 735 athletes, using a more conservative approach (10% of affected athletes would live an additional 20 years), estimated the cost per year of life saved at €14 220 for the Italian model and €37 750 for the US model.30 This estimate was in the context of a well-organised, national setting where cardiovascular PPS was part of a wider screening programme.
Costs for developing the necessary infrastructure for the evaluation and treatment of athletes as well as the costs of training specialist physicians should also be considered. In most western countries some form of screening of athletes is performed on a limited scale and necessary treatment is provided according to established guidelines. In most cases, however, there are no universally accepted standards and the necessary facilities and expertise are either limited or are not utilised appropriately. As with every national screening programme in its founding, these limitations should not hinder the development of a government-driven initiative to provide the necessary funds and resources required to permit national PPS in young athletes.
Does PPS of young athletes comply with the WHO screening criteria?
The antagonists contend that PPS does not fulfil the World Health Organization (WHO) screening criteria31 (box 4) and centre the argument against the implementation of PPS on the low incidence of SCD in athletes. According to the WHO, however, a disease process or disorder does not necessarily need to have a high incidence to be considered an important problem. Screening programmes for relatively rare diseases with potentially grave prognoses such as phenylketonuria have been in place for decades, justifying relatively uneconomic screening. Similarly, conditions causing SCD in the athletic field may deprive a youth of 40–50 life-years, have a potentially devastating effect on the family of the individual as well as profound reverberations in the athletic, scientific and lay communities. In a benevolent society such deaths cannot be considered acceptable, which has led a number of sporting organisations and governing bodies such as the International Olympic Committee and the Federation of International Football Associations to recommend or even mandate PPS, in young competitive athletes, based on current scientific evidence.7 8
Box 4 WHO classic screening criteria
1. The condition sought should be an important health problem
2. The natural history of the disease should be adequately understood
3. There should be a latent or early symptomatic stage
4. There should be a suitable screening test
5. The screening test should be acceptable to the population
6. There should be an accepted treatment or useful intervention for patients with recognised disease
7. There should be an agreed policy on who to treat as patients
8. The cost should be economically balanced in relation to possible expenditure on medical care as a whole
9. Facilities for diagnosis and treatment should be available
10. Case finding should be a continuing process and not a once and for all project.
One of the major challenges of PPS is that SCD is caused by a number of disorders with diverse pathology whose natural history is not always fully elucidated. The natural history of most disorders is, however, adequately understood and there is a strong association between athletic activity and SCD, with up to 90% of SCD occurring during or shortly after exertion. Indeed, young athletes with cardiac conditions have an almost threefold greater risk of dying suddenly compared with their non-athletic counterparts.2 Furthermore, there is a long latent stage, with most of the athletes being asymptomatic for many years and sudden death being the first presentation in the majority of cases. In addition, evidence from Italy shows that the 12-lead ECG is a suitable and acceptable screening test (simple, safe, precise and validated).
According to Wilson and Jungner31 of all the criteria that a screening test should fulfil, the ability to intervene when the condition is discovered is perhaps the most important. There are currently agreed policies by world experts on who to treat as a patient embodied by the eligibility in competitive sports recommendations in the 36th Bethesda Conference and the ESC consensus documents.32 33 The notion of saving a young athlete’s life with simple and usually non-invasive interventions such as lifestyle modification makes the implementation of PPS for quiescent cardiovascular diseases in young athletes an obligation and the concept of “don’t look don’t tell” deplorable.
PPS is less cost-effective than established screening programmes such as screening for breast cancer (£3000 per year of life saved);34 however, it is almost comparable with the cost of screening for cervical cancer (£5000–£10 000 per year of life saved). Furthermore, in the Italian model the screening cost is only partly funded by the state that sponsors the screening of all athletes under the age of 18 years. It is ethically challenging to deter financially endowed sporting organisations or even charities focused on preventing SCD in athletes from funding sportsmen who choose to undergo PPS for self-protection.
What is already known on this topic
Regular exercise is beneficial and reduces the risk of sudden death.
Athletes with underlying cardiovascular disease are at increased risk of SCD.
Screening using health questionnaires and physical examination alone has a poor sensitivity for the identification of athletes with cardiovascular diseases at risk of SCD.
What this study adds
Screening with an ECG in addition to a history and physical examination prevents SCD in sport.
Screening with ECG performed by expert sport cardiologists can be associated with a false-positive rate as low as 2%.
12-Lead ECG PPS can be considered cost-effective in the context of a well-organised, national screening programme, especially when considering the devastating effect of a sudden death in a young athlete.
Are there any alternative preventative strategies?
There are two other competing strategies that have been proposed for preventing SCD in athletes but neither is more efficient or cost-effective than the use of the 12-lead ECG as a screening tool.
The AHA advocates screening with history and clinical examination only.4 This strategy appears cheap and easy to perform but has limited value because 80% of athletes who experience SCD are asymptomatic and physical examination identifies few disorders implicated in SCD. The lack of sensitivity of the American model is highlighted in a series of SCD in young athletes, in which 115 cases, screened according to the AHA protocol, were reported. A correct diagnosis was identified in only one (0.9%) athlete who was allowed to compete.35 The limited sensitivity of this strategy has been further highlighted by prospective observational studies in the UK and Italy.13 20
The presence of automated external defibrillators has also been proposed as an alternative strategy. Although defibrillators are a useful provision in athletic events, current evidence suggest that the efficiency of such a strategy is fairly limited in young athletes because only 11% survived a cardiac arrest during competitive sport, despite a witnessed collapse, timely cardiopulmonary resuscitation and prompt defibrillation.36 Co-existent stresses of extreme exercise such as dehydration, acidosis, electrolyte imbalances and high concentrations of circulating catecholamines provide a plausible explanation for low resuscitation rates in athletes collapsing during sport.
Conclusion
PPS of young competitive athletes is recommended by both the AHA and ESC. The European recommendations have been endorsed by the International Olympic Committee and the football governing bodies, with the Union of European Football Associations advocating mandatory screening of all players participating in European championships. These recommendations are based on the 25-year Italian experience, which has shown that PPS of young athletes with a 12-lead ECG is effective in reducing SCD predominantly from cardiomyopathies and electrical disorders of the heart at the expense of a small number of false-positive tests. Healthcare governing bodies need to be convinced that now is the time for universal ECG screening of all young athletes and make the necessary provisions for nationwide screening programmes to commence.
REFERENCES
Footnotes
Contributors MP and SS carried out the literature search, analysed and interpreted the data, drafted the article and revised it critically for scientific content and approved the final version for publication. SS is the guarantor.
Funding MP is funded by a research grant from the charitable organisation Cardiac Risk in the Young (CRY), which supports preparticipation screening in young athletes.
Competing interests MP is funded by Cardiac Risk in the Young (CRY) and SS is consultant cardiologist to CRY and a CRY trustee.
Provenance and peer review Commissioned; not externally peer reviewed.