Article Text

Abstract
Objectives: To screen all players registered for the 8th CAF African Under-17 Championship for risk factors of sudden cardiac death.
Design: Standardised cardiac evaluation prior to the start of the competition.
Study population: 155 male football players from all eight qualified teams; mean age 16.4 (SD 0.68) years (range 14 to 17).
Methods: The cardiac evaluation consisted of a medical history, clinical examination, 12-lead resting electrocardiogram (ECG) and echocardiography, and was performed by three experienced cardiologists using established guidelines.
Results: Nine (5.8%) players reported cardiac symptoms, and the clinical examination was abnormal in only two players with elevated blood pressure. A total of 40 players (25.8%) showed abnormal ECG patterns. None of the players with a positive ECG showed correlating echocardiographic findings. The echocardiogram of one player appeared highly suspicious for early-stage hypertrophic cardiomyopathy, and in another player the myocardium was suspicious for non-compaction cardiomyopathy, but both had normal ECGs. Thirteen (8.4%) players showed echocardiographic findings that needed further follow-up. The percentage of players with pathological ECG patterns and some abnormal echocardiographic measurements varied substantially between different ethnic groups.
Conclusion: Cardiological screening for risk factors of sudden cardiac death of football players prior to an international competition proved feasible, and conduction by independent experts allowed high-quality standards and a consistent protocol for the examinations. Differences observed between ethnic groups indicate that guidelines for the analysis of ECGs and echocardiography might be adjusted to the target population.
Statistics from Altmetric.com
Although sudden cardiac death (SCD) related to competitive sport is relatively rare, from 0.5:100 000 per year in high school students1 to 2.3:100 000 per year in the Veneto Region of Italy,2 3 prevention of these fatal and tragic events is a major target when providing medical care for athletes. Particularly competitive sports, apart from carrying an injury risk, can serve as a trigger for sudden cardiac arrest (SCA) and even SCD.2 4 5 Apart from commotio cordis,6 vigorous exercise can trigger SCA in the presence of an abnormal underlying substrate or condition which mainly consists of structural cardiac changes (such as hypertrophic cardiomyopathy) or conduction anomalies.4 7 8 Above 35 years of age, SCD is mostly due to atherosclerotic coronary artery disease.9 10 11
Current consensus documents recommend a standard precompetition screening for every competitive athlete from the very beginning of their career and repeated regularly every 1–2 years.12 13 14 This standard screening protocol integrates a detailed medical history (including personal and family history) as well as a clinical examination and a 12-lead resting electrocardiogram (ECG).2 3 13 14 15 16 Although this protocol is recommended by the European Society of Cardiology (ESC)13 and the International Olympic Committee (IOC),14 other guidelines from North America (eg, American Heart Association) generally forego the ECG mainly due to the potential generation of false-positive findings which can generate high costs for subsequent examinations and unnecessary anxiety in an athlete until a diagnostic work-up is completed.12 17 The world’s governing body in football, the Fédération Internationale de Football Association (FIFA), has declared the prevention of sudden cardiac death in sports as one of its major targets, albeit a zero-risk circumstance will never be achievable.2 12 13 18
Thereby, it has to be respected that football players all over the world underlie various ethnic, socio-economic and specific local conditions where implementation of these screening recommendations is difficult. To ensure maximal efficacy and to achieve maximal probability to detect SCD risk factors FIFA Medical Assessment and Research Centre (F-MARC) developed a precompetition medical assessment (PCMA) which is based on the current guidelines of the ESC13 and the IOC and integrates medical history, clinical examination, 12-lead resting ECG and supplementary echocardiography. First implemented in the 2006 FIFA World Cup and FIFA Women’s World Cup 2007, the PCMA went through revision and adjustments.19
Black African athletes represent a challenging segment in sports cardiology and seem to have an increased risk for adverse cardiac events during sports.20 Unfortunately, the same group of athletes is very difficult to screen for potentially harmful underlying conditions due to presumably training-related physiological changes on ECG that are significantly more common in black athletes than in Caucasian athletes.20 21 22 23 24 25 26 Assessment of medical history and clinical examination is equivalent among different ethnic groups, although the relatively low specificity of history and physical examination as a screening test in athletic populations is a well-known disadvantage of this tool in general.24 27 28 29 30 31
The aim of the present study was to screen all players registered for the 8th African CAF Under-17 Championship 2009 in Algeria for risk factors of SCD, with respect to specific ethnic origin of the players.
Methods
The cardiac evaluation was part of a comprehensive PCMA19 and consisted of a medical history, clinical examination, 12-lead resting ECG and echocardiography.
The medical history addressed present and past complaints as well as family history according to the “Lausanne Recommendations” of the IOC.14 The physical examination was based on the Consensus Statement of the Study Group Sport Cardiology of the ESC.13 The 12-lead resting ECG was performed after 5 minutes’ rest and analysed by three cardiologists according to the same established guidelines.13 The echocardiographic measurements were performed following an adapted protocol of the American Society of Echocardiography.32 All physical examinations were performed by three experienced cardiologists during 4 days (15–18 March 2009). A high-quality standard of acquired data and a certain “unité de doctrine” in terms of a consistent protocol for the examinations could be reached with the help of international and local native-speaking FIFA approved specialists. Ethical approval was obtained from the Conseil National de L’Ordre des Medecins, Algiers, Algeria.
Results
Study population
All eight teams qualified for the 8th African CAF U-17 Championship 2009 in Algiers took part in the study with a total of 155 male players. According to the official player list, the examined players were on average 16.4 (SD 0.68) years old (range 14 to 17). However, the players’ age might not be accurate in all cases, since one team was disqualified from the competition due to an overaged player. The mean height was 173.2 (6.2) cm and the mean weight 69.2 (7.3) kg, which resulted in an average body surface area of 1.8 (0.13).
The participants originated from different ethnic groups (approximate classification): Bantu (two teams), Semitic-Hamitic (one team), Mande (one team), combination of Western-Bantoid, Mande (one team), combination of Western-/Central-Bantoid, Mande (one team), combination of Eastern-/Western-Bantoid, Central-/Eastern-Sudanese, Bantu (one team), combination of Hausa, Songhai, Kanurim and Semitic-Hamitic (one team). All players spoke either French or English, and there were no linguistic problems. The body surface area with regard to ethnicity is shown in fig 1.
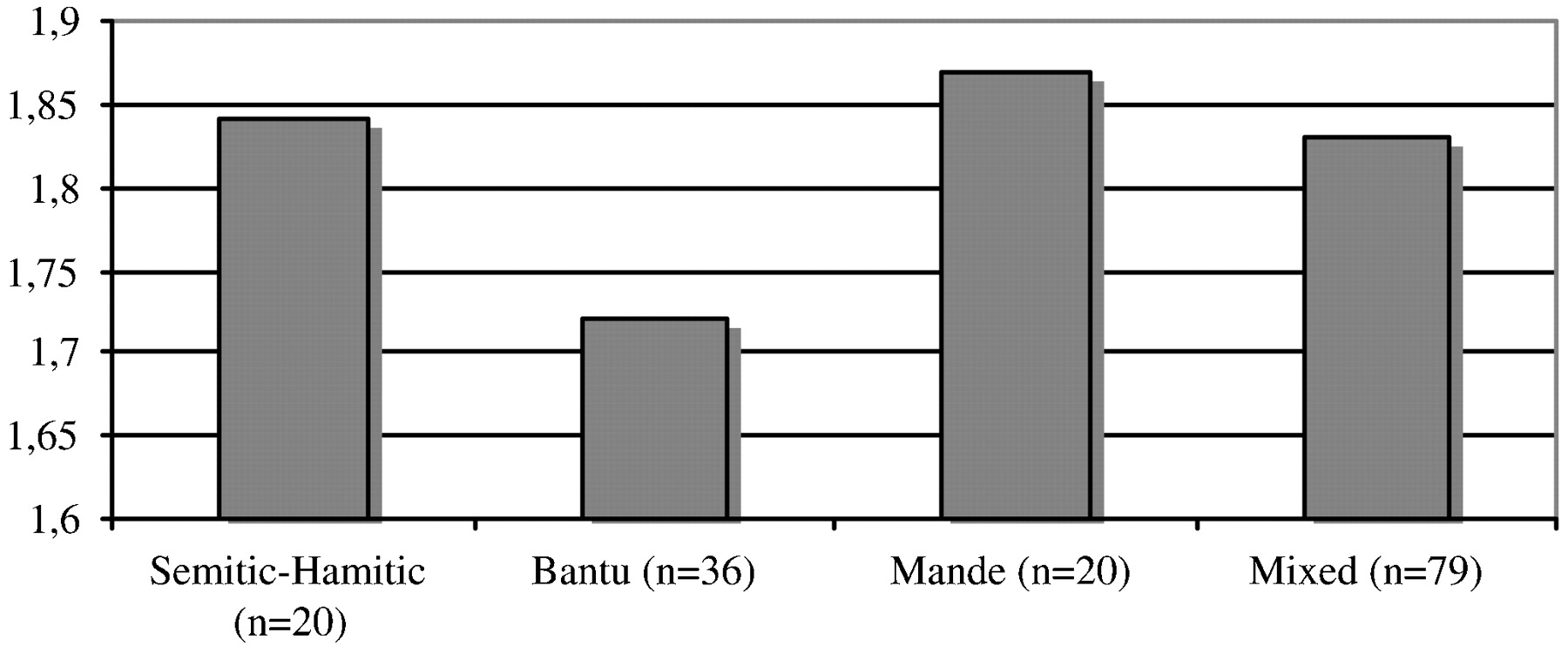
Body surface area (cm/m2) with regard to ethnicity.
Medical history and clinical cardiological examination
Teams varied substantially in the number of players who had been medically screened before the current PCMA. While in three teams all players have been medically examined before, the percentage decreased in other teams to 78%, 65%, 56%, 55% to only one player (6%) on a team. Nine (5.8%) players reported cardiac complaints, such as chest pain during exercise (n = 4), palpitations (n = 2), shortness of breath (n = 2) and dizziness during exercise (n = 1). Systemic hypertension (defined as greater than 140/90 mm Hg) was documented in two players (150/100 mm Hg and 145/95 mm Hg respectively).
Twelve-lead resting ECG
A total of 40 players (25.8%) showed abnormal ECG patterns. None of the players with a positive ECG showed correlating echocardiographic findings.
The abnormal findings consisted of significant T wave inversions (anterior and/or lateral leads) with (2/155, 1.3%) or without Q waves (29/155, 18.7%), significant Q waves without T wave changes (2/155, 1.3%), three Wolff–Parkinson–White patterns (3/155, 1.9%) and four players with an ECG suggestive for Brugada syndrome (2.6%).
Abnormal precordial R wave progression (R>S wave only in V5, V6) was not included as a criterion of abnormal ECG findings because it was present in more than half of the players (n = 80; 51.6%). Abnormal precordial R wave progression was exclusively observed in black African players but not players of Semitic–Hamitic origin.
Distribution of pathological ECG findings varied significantly (χ2 = 13.5; p<0.01) between the four ethnic groups (see fig 2).
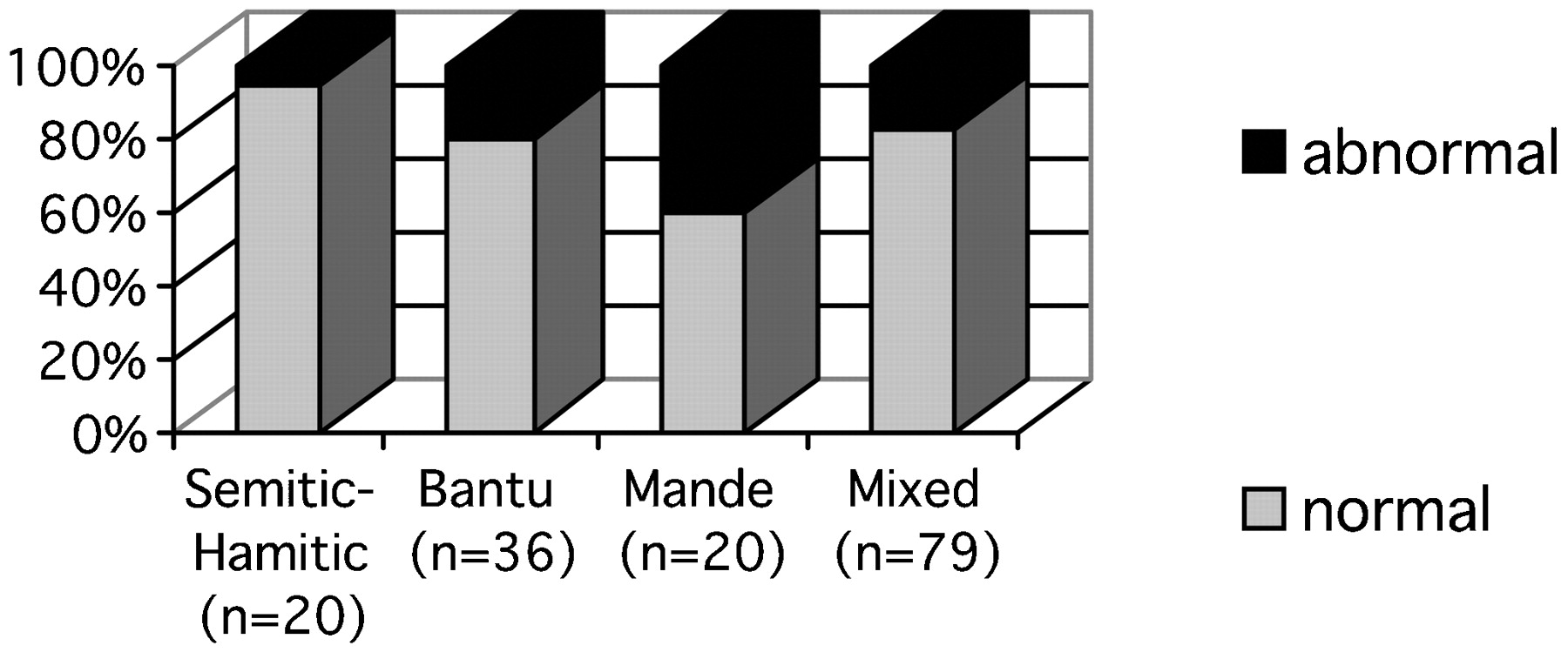
Distribution of ECG findings with regard to ethnicity.
Echocardiography
Thirteen players (8.4%) showed echocardiographic findings that needed further assessment or at least regular follow-up. Two findings should be specifically mentioned: there was one echo that appeared highly suspicious for possible mildly expressed or early-stage hypertrophic cardiomyopathy with asymmetrical septal hypertrophy (end-diastolic thickness of the interventricular septum = 12–15 mm, end-diastolic thickness of the left ventricular posterior wall = 13 mm), mild mitral regurgitation and mild aortic regurgitation (but otherwise normal findings). Another player showed suspicious myocardium suggestive for non-compaction cardiomyopathy with cryptic left ventricular apex in echocardiography (but otherwise normal findings). The other echocardiography findings requiring follow-up were non-specific and showed no statistical variance between ethnic groups. All of these athletes also had a normal ECG. The original rating of the examining cardiologist is shown below:
left ventricular hypertrophy with normal diastolic function and mild aortic regurgitation plus “palpitations” in the patient’s personal history;
left ventricular hypertrophy without signs of established hypertrophic cardiomyopathy plus “arrhythmia” in family history;
congenital subaortic membrane without significant gradient, moderate tricuspid regurgitation (normal pulmonary pressure);
moderate tricuspid regurgitation, mild mitral regurgitation with normal estimated pulmonary pressure;
moderate tricuspid regurgitation with mild pulmonary hypertension (estimated systolic pulmonary artery pressure = 43–48 mm Hg) plus patient history inconclusive for “chest pain”;
moderate tricuspid regurgitation with mild pulmonary hypertension, mild pulmonary valve regurgitation, mild mitral regurgitation plus “shortness of breath” in patient history and high blood pressure in family history;
mild to moderate mitral regurgitation;
mild to moderate tricuspid regurgitation, mild mitral regurgitation, mild pulmonary regurgitation, fibrotic papillary muscles;
moderate pulmonary valve regurgitation (prolapse);
mild pulmonary valve regurgitation and stenosis, thickened valve plus “chest pain or tightness” in patient history;
mild pulmonary hypertension (estimated systolic pulmonary artery pressure 36–41 mm Hg).
The average values of the echocardiographic findings are presented in table 1. Significant differences between the ethnic groups were observed for the left ventricle in end-diastolic diameter (p<0.001), end-diastolic volume (p = 0.011), end-diastolic thickness of the posterior wall (p<0.01), muscle mass (p = 0.002), the end-diastolic thickness of the interventricular septum (p<0.01) and the ratio of transmitral E-and A-wave velocity (p<0.02) (for details, see tables 1, 2 and fig 3).

{kind=link}
{kind=link}
{kind=link}
Significant differences between ethnic groups in echocardiographic measurements. E/A, ratio of transmitral E-and A-wave velocity; IVSTd, end-diastolic thickness of the interventricular septum; LV-EDD, left ventricular end-diastolic diameter; LV-EDV, left ventricular end-diastolic volume; LVMMI, left ventricular muscle mass; PWTd, end-diastolic thickness of the left ventricular posterior wall.
Basic echocardiographic data (n = 155)
Criteria for a positive 12-lead ECG in the present study according to the 2005 European Society of Cardiology guidelines17
Ethnic variations observed in the echocardiography may explain the differences in ECG findings between the teams. Although all players were declared to be 17 years or younger, some constellations consistent with classical “athlete’s heart” were observed. There were some high left-ventricular mass indices (highest value 181 g/m2) but the corresponding left ventricular volumes and diastolic measurements were normal and thus the enlarged cardiac mass was considered due to physiological changes.33
Discussion
The revised version of the PCMA19 34 performed by an independent expert group prior to the competition in the host country proved to be well accepted, feasible and accurate. Performing the PCMA in a relatively unpredictable environment and under difficult conditions is not always simple, but the experience and network of the local medical team as well as a great team effort of the international group of physicians allowed accurate examinations. Team officials and players were thankful and interested, and these conditions created a feeling of good team spirit. This method of data collection ensured a consistent protocol, and a high-quality standard of examinations. Thus, every player could be examined and judged directly with the responsible team physician. However, more time and resources to follow-up on suspicious findings with further specific examinations (eg, exercise test) should be considered for future PCMAs.
Challenge to perform PCMA in black-African football players
Black-African athletes seem to have an increased risk for adverse cardiac events during sports, and there are difficulties with interpreting screening findings in these athletes.21 In the present study, about a third of players had not been medically screened before. Furthermore, PCMA of black-African athletes can be challenging due to a large “grey zone” of borderline findings.
Assessment of history and clinical examination in a black-African athlete may be seen as equivalent to other ethnic groups. As expected for a group of young athletes, suspicious or pathological clinical findings were rare. Only nine players (5.8%) reported current or recent cardiac complaints. Probably some players denied any complaints because they were afraid of the consequences (eg, possible disqualification), or did not know all details about their medical family history.
Twelve-lead ECG as the crux of the matter
Twelve-lead resting ECG is part of most precompetition screening recommendations,12 13 even though its relatively low specificity as a screening test in athletic populations is a well-known disadvantage of this tool, and some consensus documents do not recommend using it in primary screening.24 27 28 29 30 31 Moreover, it is well known that black athletes show significantly more ECG alterations than Caucasian athletes,21 22 23 24 25 and black race is an independent predictor of abnormal ECG findings.1 In a previous study by Magalski et al,21 abnormal ECG patterns were present in 25% of elite American football players (mean age 23 (0.9) years) and were twice as common among black players (overall 30%) compared with white players or other races. Notably, ECG criterions have been constantly adapted in recent years to decrease the number of “false-positive” ECG findings.
Wilson et al35 reported only a 1.8% false-positive ECG rate when a modern ECG criterion was applied to screen a population of young highly trained athletes in the UK.
In the present study, the incidence of suspicious ECG changes was quite high (25.8%) based on the 2005 ESC protocol.13 If the ECGs were analysed in accordance with the subclassification of Pelliccia et al,28 36 36.4% of the players showed mildly and 19.5% distinct abnormal ECG patterns. This impressively underlines the fact that application of different ECG criteria to distinguish abnormal findings leads to dramatically different “abnormal” ECG rates. It also suggests that an improved understanding of physiological ECG changes in athletes and the influence of different ethnic backgrounds on the ECG will allow further modifications of the ECG criterion used to distinguish abnormal findings and should yield lower false-positive rates. Specifically from this study, a large proportion of athletes (20%) had significant T wave inversions in the anterior and/or lateral leads. The significance of this finding in black African athletes deserves further clarification through a larger study.
It is also of note that abnormal precordial R wave progression (R>S wave only in V5, V6) was excluded as a criterion because it was present in about every second player. Interestingly, this finding was not observed in any player of Semitic–Hamitic origin. The frequency of abnormal ECG patterns varied substantially between teams and ethnic groups. The percentage of suspicious ECG changes increased from non-black African (Semitic–Hamitic) to southern Africans (Bantu) to south-western Sub-Saharan groups (Mande). This finding needs further evaluation and might have impact on recommendations for different regions in Africa.
Brugada-like ECG patterns were found in four (2.6%) players. These athletes were found to have ECG findings suspicious for Brugada syndrome, but no definitive diagnosis could be made that warranted disqualification. “Brugada ECG patterns” are sometimes difficult to differentiate from right bundle branch block and ST segment elevation, which are quite common findings in trained athletes.25 However, without related symptoms, Brugada syndrome is less likely, and its occurrence remains to be assessed in a larger black-African population.25
Magalski et al concluded that 12-lead ECG should not be part of primary screening of young athletes due to the generation of potentially false-positive findings.21 This conclusion is debatable, and it does not solve the general problem. In the present study, some players had ECG specific pathological findings (eg, Wolff–Parkinson–White syndrome); others need a further examination and follow-up. Additional echocardiography in certain risk groups (eg, black Africans) may help to understand the value of these findings.
Lack of substrate for a multitude of ECG changes
As described in other surveys,21 none of the abnormal ECG findings we observed was related to an unequivocal structural abnormality on echocardiography. However, some ECG changes may represent an early stage of a structural heart disease and may have an impact on the general risk profile and prognosis of an athlete.27 37 38 39 40 Therefore, these players need regular follow-up examinations. In our population, one player showed LV morphology compatible with possible mildly expressed HCM and another with a suspicious myocardium suggestive for non-compaction cardiomyopathy whose prevalence may have been underestimated in the past and influenced by racial origin.26 In addition, three athletes were found with increased estimated pulmonary pressure, which was unexpected. The athletes with borderline echocardiographic findings, representing a grey area of undefined cardiac diagnosis, certainly deserve additional medical care and periodic follow-up.
Significant variations in left ventricular muscle mass, end-diastolic thickness of the interventricular septum and ratio of transmitral E-and A-wave velocity were observed between different ethnic groups. These ethnic differences probably affect the ECG findings and deserve a larger study. To the best of our knowledge, there are no population-based studies of the normal ECG in African adolescents that is correlated with echocardiographic changes. Such studies are required to establish ECG norms among the various subpopulations of Africa.
Conclusion
Standardised cardiac screening for risk factors of SCD of football players prior to an international competition proved to be feasible, and conduction by independent experts allowed high-quality standards and a consistent protocol for the examinations. As expected, personal and family history were of limited value and potentially complicated by a tendency for players to conceal symptoms to avoid possible disqualification for the competition. The ECG was the key point of the screening: about a quarter of the players showed an abnormal ECG pattern, but none related to unequivocal evidence of a structural abnormality on echocardiography. However, a substantial proportion of borderline findings imply that more time and resources to follow-up with further specific examinations should be considered for future PCMA. Finally, differences observed between ethnic groups indicate that guidelines for the analysis of ECGs and echocardiography might be adjusted to the target population.
Acknowledgments
We thank the Fédération Algérienne de Football (FAF), for their support, and the Confédération Africaine de Football (CAF), for their cooperation. The authors highly appreciate A Rahli, S Chabane, M Tahmi and S Boumeridja (Algeria) for their assistance with the cardiological examinations. We acknowledge P D’Hooghe (Belgium), W Meeuwisse (Canada) and P Awaragi (PrivIT Healthcare) for their collaboration. The authors express their gratitude to Cerner Corporation (USA), particularly J Wander, T Kilzer, S Wallace, B Hutchison and A Amzert for developing the electronic database and entering the cardiological data. Special thanks to the coaches and players of the teams for their participation in the study.
REFERENCES
Footnotes
Funding The authors gratefully acknowledge Fédération Internationale de Football Association for the funding of the study.
Competing interests None.
Ethics approval Ethics approval was provided by the Conseil National de L’Ordre des Medecins, Algiers, Algeria.
Provenance and peer review Commissioned; not externally peer reviewed.