Article Text

Abstract
Objective The ‘hybrid procedure’, consisting of surgical banding of the pulmonary arteries with intraoperative stenting of the arterial duct, was developed as primary palliation in hypoplastic left heart syndrome (HLHS), avoiding the risks of cardiopulmonary bypass. In many centres, it is reserved for low birth weight, premature or unstable neonates; however, its role in such high risk cases of HLHS has yet to be defined.
Methods The preoperative condition of all patients with HLHS who underwent either the hybrid or the Norwood procedure for HLHS between 2005–2011 was analysed retrospectively, using a modified comprehensive Aristotle score. We then compared operative, interstage and 1 year mortalities between the groups after Aristotle adjustment via Cox proportional hazards analyses.
Results Of 138 patients with HLHS, 27 had hybrid and 111 Norwood procedures. The hybrid group had significantly higher Aristotle scores (mean 4.1 vs 1.8; p<0.001); however, there was no significant difference in mortality at any stage. At 1 year, the overall unadjusted survival among Norwood and hybrid patients was 58.6% and 51.9%, respectively, yielding an Aristotle adjusted hazard ratio for mortality among hybrid patients of 1.09 (95% CI 0.56 to 2.11, p=0.80).
Conclusions Applying a hybrid approach to high risk patients with HLHS produces a comparable early and interstage mortality risk to lower risk patients undergoing the Norwood procedure. Prospective studies are needed to establish whether the hybrid procedure is a viable alternative to the Norwood procedure in all HLHS patients in terms of both mortality and long term morbidity.
- Congenital Heart Disease
Statistics from Altmetric.com
Introduction
In most centres, the 30 day survival following the Norwood procedure as the first stage operation to palliate hypoplastic left heart syndrome (HLHS) is >70%, although there remains significant perioperative and interstage mortality and morbidity.1 The risk increases with factors such as poor preoperative condition, prematurity, low birth weight, preoperative obstruction to pulmonary venous return, small ascending aorta diameter, and if the procedure is performed beyond 2 weeks of age.2–4 Survival rates are independent of the type of pulmonary shunt used.5 The obligatory use of cardiopulmonary bypass may be a significant contributing factor to adverse outcomes.
In view of these concerns, an off-pump ‘hybrid procedure’ combining both surgical and catheter techniques has been developed, consisting of surgical placement of bilateral pulmonary artery bands through a midline sternotomy, followed by stenting of the arterial duct (percutaneously or via direct pulmonary artery access), and finally percutaneous septostomy if needed.6 The patient then undergoes a staged surgical pathway similar to the Norwood approach, although the next stage is more complex, involving debanding of both pulmonary arteries, removal of the ductal stent, and reconstruction of the aortic arch with proximal aortopulmonary anastomosis. A source of pulmonary blood supply must be established either by a superior cavopulmonary anastomosis (‘combined stage I and II’) or a modified Blalock-Taussig (BT) shunt as for a classical stage I operation. The subsequent stages (upper cavopulmonary and then total cavopulmonary anastomosis=Fontan circulation) are the same whichever route is adopted.
Initial results suggested that outcomes following the hybrid procedure were comparable to the Norwood procedure6–8; however, objective comparison has been difficult as the indications for hybrid versus Norwood are not standardised. In some centres, including our own, the hybrid procedure is reserved for higher risk, more complex and/or unstable patients. Thus, to provide a more practical comparison of the two approaches, both the preoperative condition of the patient and extracardiac risk factors need to be considered. To date there have been no reports published that compare the outcomes of the Norwood and hybrid procedures in this way.
The aim of this study was therefore to compare the medium term outcomes following the hybrid versus Norwood procedures in HLHS patients after risk adjustment based upon a modified comprehensive Aristotle score.
Methods
The study was approved as an audit by the institutional board of the Evelina Children's Hospital (ECH), London, on 15 October 2009. The need for parental consent was waived.
Patients with HLHS who underwent either the Norwood or hybrid procedure during the hybrid era (from December 2005 onwards) were identified from the institutional database of the Department of Congenital Heart Disease (Heartsuite, Systeria, Glasgow, UK) up to and including September 2011. Any patients without a diagnosis of classical HLHS (eg, unbalanced atrioventricular septal defects) or patients with an incomplete dataset were excluded. The remaining patients were divided into two groups according to the treatment type.
The Norwood procedure was carried out using cardiopulmonary bypass employing short periods of hypothermic circulatory arrest combined with isolated cerebral perfusion and insertion of modified BT shunt (the ‘Sano’ modification with right ventricle to pulmonary artery conduit was not used in any patient). Inclusion criteria for the hybrid procedure during the study period were preoperative asphyxia, low birth weight (<2.5 kg), restrictive interatrial septum, and certain anatomical variances (eg, hypoplastic left pulmonary artery), as these patients had a poor outcome in the historical Norwood population before the beginning of the hybrid programme. The procedure was performed as described previously by our group.6 Bilateral branch pulmonary artery banding was performed via midline sternotomy with two pieces of cut polytetrafluoroethylene sutured in place over the branch pulmonary arteries to an external diameter of 3 mm to prevent band migration. A balloon expandable premounted Genesis PSS stent (Cordis, Corp, Miami, Florida, USA), sized at 1–2 mm greater than the diameter of the arterial duct, was deployed via direct catheterisation of the pulmonary artery.
If indicated, transcatheter balloon atrial septostomy was also performed either at the time of the procedure, or later if required. In cases where an intact or severely restrictive interatrial septum had been diagnosed antenatally, elective caesarean section was performed in an adjacent operating theatre, and immediate surgical septectomy performed on cardiopulmonary bypass at 28°C with very brief circulatory arrest and venous inflow occlusion but no cardioplegic arrest.6
A total of 139 patients fulfilled the selection criteria. None had to be excluded for incomplete data. One hybrid patient died at 1 week of age due to an autosomal recessive metabolic disorder (Zellweger syndrome, undiagnosed at the time of surgery) and was excluded from further analysis. Of the 138 remaining patients, 113 (82%) had been diagnosed antenatally with HLHS. A preponderance of males was noted (n=94, 68%).
Risk adjustment via the modified Aristotle score
The Aristotle and Risk Adjustment for Congenital Heart Surgery (RACHS) scoring systems were designed to risk adjust outcomes in congenital heart disease surgery, taking into account the procedure performed and/or patient complexity. The RACHS score has been shown to be a more powerful predictor of overall mortality9; however, the comprehensive Aristotle score, which also takes into account key variables such as birth weight, prematurity, and major extra-cardiac abnormalities, has been shown to be a superior predictor of 30 day postoperative mortality.10
Originally designed by consensus opinion from a group of experienced cardiothoracic surgeons to compare surgical outcomes across centres,11 the Aristotle score has two forms: the basic score simply assigns a numerical value (from 1.5–15) for the procedure being undertaken, based on the anticipated technical difficulty and the potential for morbidity and mortality. For the Norwood procedure, this value is 14.5; there is currently no value assigned for the hybrid procedure. The comprehensive Aristotle score further adjusts for the complexity of the individual patient by taking into account numerous patient specific, ‘procedure independent’ characteristics, and has been shown to be a good predictor of surgical mortality even when used without the basic score values.12 Thus, to compare the preoperative status of each patient, a modified procedure independent Aristotle score was calculated retrospectively from the medical records. A number of scoring criteria in the comprehensive score were excluded: ‘left ventricular function’, as this is not applicable in HLHS; ‘elevated lung resistance’, as this is not routinely measured in patients before the initial palliation, and ‘surgical factors’, as these were not directly relevant or comparable. In total, 26 clinical perioperative factors were considered for scoring counting between 0.5–4.0 points (theoretical maximum score 39.0 in a single patient); 42 additional comorbidities were also included counting between 0.5–4.0 points (theoretical maximum 43.0 points).
Follow-up
All patients were followed up until 1 year of age, with deaths reported as occurring within four periods:
-
Early post stage I death: death at primary procedure or within 30 days
-
Interstage death: all deaths between the initial and the second procedure
-
Early post stage II death: death at second stage procedure or within 30 days
-
Late post stage II death: death occurring from after 30 days post second stage up to 1 year of age.
Statistics
Unadjusted bivariate comparisons were performed using Student's t tests and Fisher's exact tests as appropriate. Thirty day outcomes between the Norwood and hybrid groups were compared after adjustment for Aristotle scores using multivariable logistic regression. Survival up to 1 year of age was compared in two ways: (1) in unadjusted form via the log rank test using Kaplan-Meier plots; (2) after adjustment for modified Aristotle score via Cox proportional hazards regression. Data were analysed using the Stata statistical software package (Stata Statistical Software: Release 12. College Station, StataCorp LP, Texas, USA).
Results
Of the 138 patients with HLHS fulfilling the inclusion criteria, 111 underwent the Norwood procedure and 27 the hybrid procedure. The average age at operation was 6.0 days for the Norwood group (median 4 days, range 0–56 days), and 5.3 days for the hybrid group (median 4 days, range 0–19 days; p=0.68) (figure 1A). Five of 27 hybrid procedures were performed on day 1 of life. In each case a restrictive or intact interatrial septum had been diagnosed antenatally; the hybrid procedure was performed immediately after birth by caesarean section in theatres and included surgical septectomy with a bypass time of 34–83 min and a circulatory arrest time of 4–12 min. Of the remaining 22 hybrid patients eight required transcatheter atrial septostomy, either at the primary procedure (two patients) or subsequently (six patients, range 1–21 days postoperatively). One of these had an atrial stent placed 53 days after the hybrid procedure. Fourteen hybrid patients did not require any intervention to enlarge the atrial communication. In contrast, one of 111 Norwood procedures (19% vs 1%; p<0.001) was performed on day 1 of life (again due to restrictive atrial physiology). A modified BT shunt of diameter 3.5–4.0 mm was used in all Norwood cases (3.5 mm: n=87; 4mm: n=34). One of them underwent atrial septal stenting 89 days after the Norwood operation. Extracorporeal membrane oxygenation (ECMO) was not utilised on any patient postoperatively.

(A) Age (in days) of patients in each group at the time of their primary procedure. Three patients in the Norwood group had operations performed at >20 days of age: two patients were diagnosed following postnatal collapse at 34 and 56 days respectively; one patient born at 32 weeks with a birth weight of 1.67 kg had primary palliation delayed until day 52 of life. (B) The number of patients in each group attracting specific modified comprehensive Aristotle scores. *Forty-three patients in the Norwood group attracted a score of zero (not charted).
The modified comprehensive Aristotle score was calculated for each patient retrospectively. All categories in which more than one patient from either group attained a score are documented in table 1.
Frequency of patient characteristics attracting Aristotle scores
The mean Aristotle score was 1.8 (median 1, range 0–12.5) for the Norwood group, and 4.1 (median 4, range 0–11) for the hybrid group. Figure 1B demonstrates the range of scores obtained in each group and the number of patients achieving each score. There was a significantly higher mean modified comprehensive Aristotle score in the patients in the hybrid group compared with the Norwood group (p<0.001).
Early and interstage mortality
Neither unadjusted nor Aristotle adjusted mortality differed between the groups for early (<30 days) or interstage mortality. Of the 111 patients in the Norwood group, 31 (27.9%) died within 30 days of surgery compared to 9/27 (33.3%) of the patients in the hybrid group. The absolute early mortality risk difference was 5.4% (95% CI −14.2% to +25.0%, p=0.64). After adjustment for Aristotle score, the odds ratio (OR) for early death among the hybrid patients was 1.08 (95% CI 0.41 to 2.84, p=0.87).
Similarly, the interstage death rate among Norwood and hybrid patients was 10/80 (12.5%) and 3/18 (16.7%), respectively, providing an absolute interstage mortality risk difference of 4.2% (95% CI −14.5% to +22.8%, p=0.70). After adjustment for Aristotle score, the OR for interstage death among hybrid patients was 1.06 (95% CI 0.23 to 4.87, p=0.94).
One intraoperative death occurred in each group; both are included in the above numbers. In the hybrid case this was one of the five patients who underwent surgical septectomy immediately after birth. Two of the remaining four hybrid patients who underwent this approach died before 3 days of age, with two surviving to Fontan completion.
Interstage interventions
Additional interventions were performed in six patients in the hybrid group (22%) and six patients in the Norwood group (5%). One Norwood patient required transcatheter balloon dilation of the left pulmonary artery, 14 days postoperatively before stage II, and one hybrid patient underwent stenting of the left and right pulmonary artery at 180 days postoperatively, before combined stage I and II. Three Norwood patients had stents placed in stenosed BT shunts at 17, 20, and 58 days after surgery, and one patient who had an additional classical BT shunt on the first postoperative day needed stenting of the innominate artery on day 114 after Norwood. Four hybrid patients required transcatheter re-stenting of the arterial duct due to restenosis either at the proximal or distal end, at 21 days after the hybrid procedure (two patients), 91 days after the procedure, or due to stent migration on day 3 after the hybrid procedure. One patient of each group received an interatrial stent as described above.
Early stage 2 survival
Three of 70 (4.3%) Norwood patients who underwent stage II died within 30 days of the procedure compared to two of the 15 (13.3%) hybrid patients who underwent the combined stage I and II procedure, yielding a risk difference of 9.0% (95% CI −8.8% to +26.9%, p=0.22).
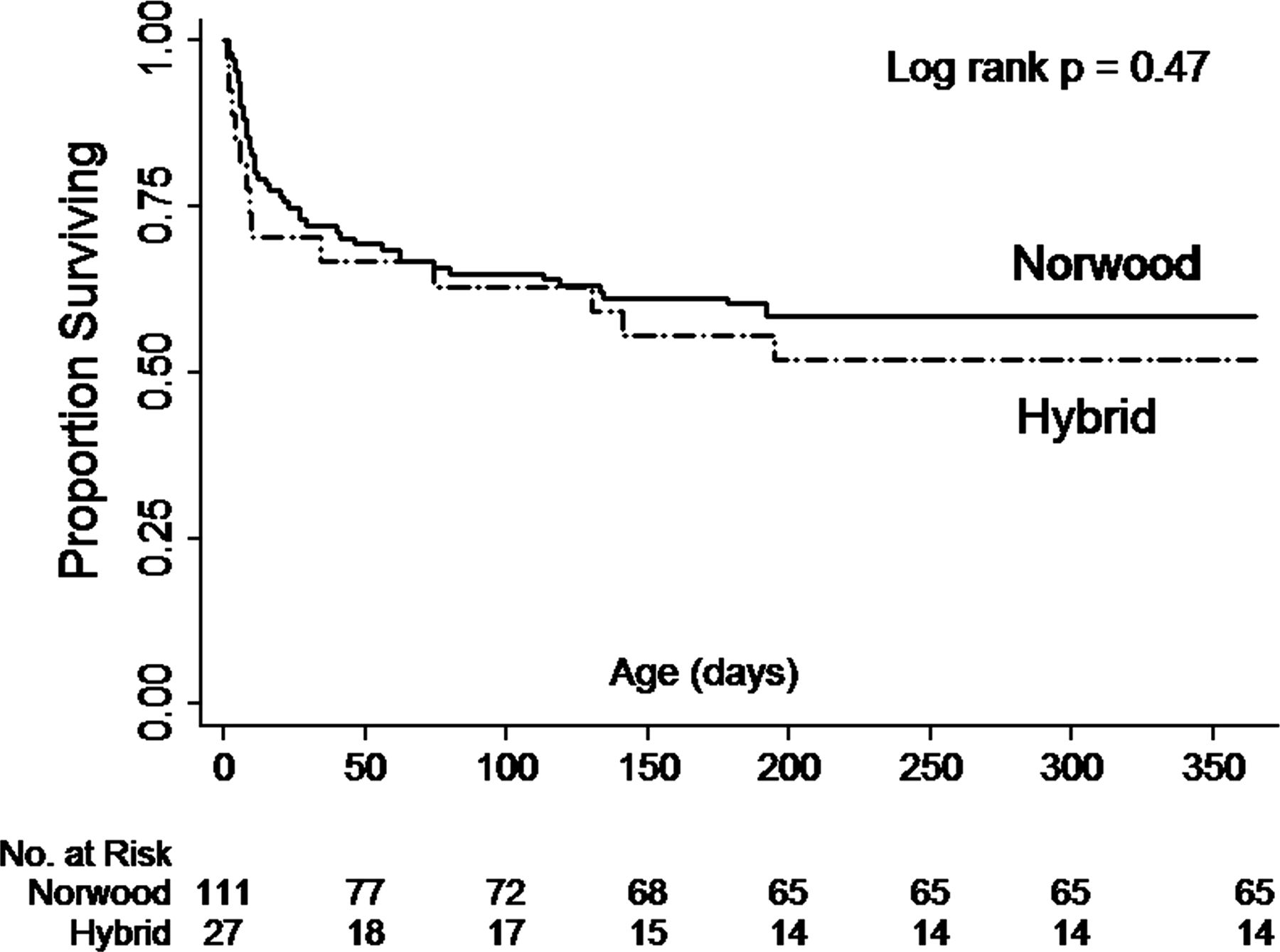
A Kaplan–Meier diagram depicting survival for both groups is shown in figure 2. The overall 1 year survival for the Norwood and hybrid groups was 58.6% and 51.9%, respectively, giving a risk difference of 6.7% (95% CI −14.3% to +27.7%, p=0.47, log rank test). This lack of difference persisted in the Cox proportional hazards analysis after adjustment for Aristotle score, yielding a hybrid HR for mortality of 1.09 (95% CI 0.56 to 2.11, p=0.80).

{kind=link}
{kind=link}
Kaplan–Meier diagram showing the survival until 1 year. All patients who survived until 1 year had received conversion to a partial cavopulmonary anastomosis.
Survival to Fontan procedure
Fifty-three Norwood and eight hybrid patients underwent Fontan completion. There was no mortality after this operation. Eight Norwood and six hybrid patients are awaiting Fontan completion.
Subgroup analysis: high Aristotle score
As a series of sensitivity analyses, we recalculated the early and late risk differences on the subgroup of patients with the highest modified comprehensive Aristotle scores only (those in the top quartile, with a score ≥3.5), encompassing the Norwood (n=22) and hybrid (n=15) groups. This did not yield any systematic differences in mortality. The 30 day mortality rate for the Norwood and hybrid subgroups was 36.4% and 40%, respectively, yielding an absolute early mortality risk difference of 3.6% (95% CI −28.2% to +35.5%, p=1.0). Similarly, the 1 year mortality rate for the Norwood and hybrid groups was 50.0% and 53%, respectively, yielding an absolute early mortality risk difference of 3.3% (95% CI −29.4% to +36.1, p=1.0).
Discussion
The specific risks associated with circulatory arrest, cardiopulmonary bypass and cardiotomy are obviated by the use of the hybrid procedure instead of the traditional Norwood procedure.7 ,8 In unstable patients with significant comorbidities, the hybrid procedure potentially offers a lower risk alternative to the Norwood procedure, and some units, including our own, utilise the procedure exclusively for such patients. This approach appears to have merit. By using a modified comprehensive Aristotle score we have demonstrated that the outcomes of the Norwood and hybrid procedures in patients with HLHS were comparable, despite the hybrid cohort having more preoperative risk factors, such as lower birth weight, and undergoing earlier intervention.
Our data add to that growing body of encouraging results from the small number of centres offering the hybrid procedure.7 ,13 However, there continues to be wide variation between centres both in terms of patient selection and the precise technique used. While the patients in the hybrid group in our series were of significantly lower birth weight and higher risk overall, our data show no clear ‘cut-off’ Aristotle score or other preoperative risk factor which could be directly associated with improved outcome; hence the hybrid procedure must continue to be compared with the contemporary outcomes of the Norwood procedure and its modifications.
In our series, total mortality before stage II in both the Norwood and hybrid cohort was high (37% and 44%, respectively). We are a quaternary referral centre covering a large geographical area, and results for the Norwood procedure in our centre from 2007–2010 are comparable to those of other UK centres14 (data for the hybrid procedure are not routinely collected). Other international reports have comparable outcomes for the Norwood procedure, although there are differences in the 30 day mortality and the further interstage mortality.15 A series from Kiel, Germany showed low perioperative mortality, but overall interstage mortality comparable to our series.16 Results reported by the US Paediatric Heart Network showed a similar mortality rate to that presented in our study.5 Our hybrid mortality rate is comparable to this unselected cohort of patients undergoing the Norwood procedure in these reports; however, it should be noted that the hybrid may be performed differently in other centres. For example, the stenting of the arterial duct can be performed percutaneously17 or via direct pulmonary artery access as in our centre. The use of a ‘reversed’ BT shunt to address the issue of retrograde aortic arch malperfusion has also been described.18
While it is clear that patients undergoing surgery for HLHS have an important interstage mortality risk, the precise reasons for this are unclear,1 and perioperative management varies considerably between centres. The recent introduction of interstage home surveillance programmes for infants with HLHS has shown that regular monitoring of somatic growth, transcutaneous oxygen saturations, and earlier timing of intervention can reduce the total interstage mortality.19 During the study period, we did not have such a monitoring programme in place. This practice is currently under review.
An alternative approach to primary palliation of HLHS, consisting of pulmonary arterial banding with medical support of the arterial duct with intravenous prostaglandin and later conversion to Norwood, was not yet published during our study period and has not been adopted in our institution.20 However, owing to the complexity of the combined stage I and II, and to reduce the problems associated with branch pulmonary artery stenosis, we have recently changed our management strategy to an intermediate stage I operation beyond the neonatal period following the hybrid procedure. Analysis of the implications of this approach is ongoing and does not apply to the cohort in this paper.
Following the hybrid procedure without subsequent conversion into stage I, a more complex second stage is required, in which the reconstruction of ventricular outflow, usually performed during the Norwood procedure, is performed simultaneously with superior cavopulmonary anastomosis (combined stage I and II). While the numbers in our series were small, we could show no appreciable difference in early mortality beyond the stage II procedure, in keeping with other published data.21
The prophylactic use of mechanical ventricular assistance devices (VADs) after stage I palliation is controversial22 and is not offered in our centre. The use of postoperative ECMO has been associated with an increased mortality and morbidity.23 This may be due in part to ECMO being generally reserved for use as a ‘bridge to recovery’ in unstable patients following surgery, as is the policy in our centre. In our series there was one intraoperative death in each group; however, all other patients were successfully weaned off bypass (if used) in the operating theatre, and no patients required postoperative ECMO.
The treatment of HLHS with primary orthotopic heart transplantation is not routinely offered in the UK, not least due to the extreme scarcity of suitable donor organs in this age group. It remains an option for patients in whom surgical palliation has failed.24 At the time of publication, only one of our 111 Norwood patients has undergone cardiac transplantation 8 months after stage II.
Finally, in long term survivors of HLHS the burden of long term neurodevelopmental deficits is high. The association between congenital heart disease and abnormal structural25 and functional26 brain development is well described and multifactorial; however, cardiopulmonary bypass with deep hypothermic circulatory arrest during surgery has been strongly implicated.27 There is evidence to suggest that children with congenital heart disease may have a unique vulnerability in the neonatal period.28 To date, no studies have examined the potential advantages of postponing the first bypass-dependent stage from the early neonatal period to later in infancy.
Study limitations
This is a retrospective single institution study. Nevertheless, the number of patients allowed an appropriate statistical comparison of patients undergoing either hybrid or conventional Norwood procedures using the modified comprehensive Aristotle score. Alternative scoring systems such as RACHS were not felt to be appropriate, as the procedure independent variables are reflected in greater detail in the comprehensive Aristotle score.
Conclusion
A hybrid approach to high risk patients with HLHS produces comparable early and 1 year mortality risks to lower risk patients undergoing the Norwood procedure. Prospective studies are needed to establish whether the hybrid procedure is a viable alternative to the Norwood in all HLHS patients, in terms of both mortality and long term morbidity.
Key messages
-
What is already known on this subject?
-
Hybrid treatment for neonates with hypoplastic left heart (HLHS) is offered as an alternative first step of staged surgery for high risk patients. The comprehensive Aristotle score was designed for risk stratification for children undergoing surgery for congenital heart disease.
-
How might this impact on clinical practice?
-
Applying a hybrid approach to high risk patients (as estimated with the comprehensive Aristotle score) with HLHS produces a comparable early and interstage mortality risk to lower risk patients undergoing the Norwood procedure.
-
How might this impact on clinical practice?
-
The hybrid procedure might be an alternative treatment option not only for high risk patients, but for unselected neonates with HLHS.
References
Footnotes
-
Competing interests None.
-
Ethics approval Institutional board of the Evelina Children's Hospital (ECH), London, on the 15th October 2009.
-
Provenance and peer review Not commissioned; externally peer reviewed.