Article Text

Abstract
Objectives The objective of this study was to determine the prevalence of atrial fibrillation (AF) in a tertiary care centre, to describe the comorbidity profile of hospitalised patients with AF, and to evaluate the appropriateness of their maintenance antithrombotic management.
Methods In a cross-sectional, descriptive study, all consenting hospitalised patients from 36 wards in a University hospital (excluding critical care units, psychiatric, maternity and paediatric wards) received an ECG on a single day. Also their charts were reviewed for key demographic and clinical data. For patients with AF, all factors and comorbidities comprising thromboembolic (CHA2DS2-VASc) and bleeding risk (HAS-BLED) were listed. The appropriateness of long-term anticoagulant therapy was assessed according to the 2010 international guidelines (CHA2DS2-VASc score 0=aspirin or no antithrombotic treatment; 1=aspirin or oral anticoagulant treatment (OAC); ≥2=OAC). The response rate was 79.7%, that is, an ECG was performed in 636 of 812 eligible hospitalised patients.
Results AF was present on ECG in 58 patients reflecting a 9.1% hospital point prevalence (95% CI 6.9% to 11.3%). Of the remaining 587 participants, 49 had a history of AF. Hence, 107 AF cases were identified, yielding a total prevalence of 16.8% (95% CI 13.9% to 19.7%). Patients with AF were detected in every hospital zone, with highest prevalence rates in zone ‘thorax’ (29.3% (95% CI 22.2% to 36.4%)) and ‘internal medicine’ (21.7% (95%CI 14.8% to 28.6%)). Patients with AF were older than patients without AF (78.7±10.3 years versus 62.7±15.9 years; p<0.001). The most common associated comorbidities were hypertension (63.6%) and valvular heart disease (58.9%). Most patients with AF were at high risk for stroke (CHA2DS2-VASc-score ≥2 in 92.5%). Overall, only 51.3% of all patients did receive appropriate anticoagulant long-term management, while 31% were undertreated and 17.7% were possibly overtreated.
Conclusions This hospital-based study revealed high AF prevalence rates (16.8%). Patients with AF were present in all hospital zones and almost all patients were at high risk for stroke. Anticoagulation management was likely inappropriate in 48.7%, indicating the need for better guideline implementation initiatives to guarantee hospital-wide optimised care for patients with AF.
Statistics from Altmetric.com
Introduction
There is increasing evidence about the prevalence of atrial fibrillation (AF), highlighting the burden of AF as an evolving epidemic.1–9 At the end of the 20th century, the overall prevalence in the general population was reported to be around 1–2%. Nowadays, overall prevalence numbers range from 2.3% to 3.4%.1 ,3 ,5 ,9 AF prevalence is strongly dependent on age, increasing from <0.5–1% at age 40–50 years to over 6–15% in adults 80 years or older.3 ,8 Moreover, this population will further increase in the future as society ages and due to accumulation of predisposing conditions.4–8
Preventive healthcare and optimal guideline-based treatment management are needed to reduce AF-associated morbidity, mortality, unplanned hospitalisations and emergency room visits.10 Since AF is correlated with significant morbidity, including increased risk of stroke and heart failure, it consequently has a major impact on healthcare systems.11–13 Interdisciplinary AF expert programmes, likely with strong involvement of specialised nurses and providing evidence-based care are suggested to improve implementing and adapting personalised AF management.10 ,14 ,15 Nurse-coordinated care leads to a higher relative efficacy with respect to prevention of cardiovascular mortality and hospitalisations.14 AF expert programmes can be organised to focus on patients with AF referred to the outpatient clinic and on hospitalised patients.10 Hence, concerning the last, knowing prevalence, characteristics and medication management will help to establish and refine the need and scope of such programmes.
To our knowledge, no quantitative data exist on the overall prevalence of AF and its distribution in a whole hospital setting. Hospitalised patients are likely older and have more comorbidities. By consequence, it can be anticipated that AF prevalence in a hospital setting is higher compared with the community. Hospital-based epidemiology studies mainly reported on cohorts from cardiology departments or a combination of primary care patients and those attending a hospital as inpatients or outpatients.16–20
The main aims of this study were to determine the point-prevalence of AF, that is, measured on a single day, in a tertiary care centre, and to gain insight in the profile of hospitalised patients with AF. We also wanted to evaluate the appropriateness of the maintenance of antithrombotic management of the hospitalised patients with AF since antithrombotic therapy has proven mortality reduction benefits but is also related to iatrogenic bleeding if used inappropriately.11
Methods
Study population
A cross-sectional, descriptive ECG-based study was conducted at the University Hospitals Leuven, Belgium on Tuesday 13 March 2012. The study covered 36 wards situated in seven different hospital zones: thorax (nine wards); internal medicine (seven wards); abdomen (seven wards); oncology (six wards); locomotor system (three wards); reproduction and growth (three wards); and sensory system (one ward). Psychiatric, maternity and paediatric wards were excluded from patient recruitment, as well as outpatient clinic services and critical care units. The latter units were excluded because AF often transiently occurs in critically ill patients. Patients hospitalised in the selected wards were included if they were ≥18 years old and had given verbal consent. Patients were also excluded if they were source-isolated or not Dutch-speaking.
Definitions
Point prevalence was defined as ‘all patients diagnosed with AF on ECG at the time of measurement’. Overall prevalence was defined as ‘all patients diagnosed with AF on ECG and/or known with AF as evidenced from their medical history’.
Procedure
The day before the study, all hospitalised patients of the 36 eligible wards received a brochure with information about AF and the planned study. At the day of measurement and after obtaining verbal informed consent, a resting six-lead body surface ECG (leads I, II, III, aVL, aVF, aVR) was performed in all consenting patients. The ECG recordings were performed in a sitting or lying position, and were stored digitally. The full data collection was done within an 8 h period. Subsequently, AF prevalence was determined through analysis of all stored ECG traces by a certified cardiologist and clinical nurse specialist. Traces showing atrial flutter were also included and classified under ‘AF’, since in essence both arrhythmias are very similar concerning risk factors, consequences and management.21
Variables and measurement
Full demographic and clinical data of patients with AF were retrieved from hospital records, while a smaller data set was compiled for all participating patients. Demographic variables included gender, age, weight, height and the calculated body mass index. Belgian population data from the Belgian Federal Public Service Economy were used for age comparison. The type of AF (first diagnosed; paroxysmal; persistent; permanent) was based on the definitions of the European Society of Cardiology guidelines for the management of AF.11 For patients with AF, all risk factors and comorbidities comprising the thromboembolic risk score ‘CHA2DS2VASc’ (Congestive heart failure/LV dysfunction (EF ≤40%); Hypertension (defined as systolic blood pressure ≥140 mm Hg); Age ≥75;Diabetes mellitus; Stroke/Transient Ischaemic Attack (TIA); Vascular disease, Age 65–74, Sex category (female gender)) and bleeding risk score ‘HAS-BLED’ (Hypertension (defined as systolic blood pressure >160 mm Hg); Abnormal renal and liver function; Stroke; Bleeding tendency or predisposition; Labile INRs (if taking Vitamin K Antagonists); Elderly (age >65); Drugs (concomitant aspirin, NSAID) or alcohol abuse or excess (>4/day)) were listed. Congestive heart failure was defined as heart failure with reduced EF (≤40%) or patients with recent decompensated heart failure requiring hospitalisation, irrespective of EF.12 Vascular disease was defined as patients with a history of ischaemic heart disease, complex aortic plaque and peripheral arterial disease (PAD), including prior revascularisation, amputation due to PAD or angiographic evidence of PAD. Patients with abnormal renal function were those with a history of acute or chronic kidney disease and a serum creatine of ≥2.26 mg/dL, chronic dialysis or after kidney transplantation. Other comorbidities listed were ‘valvular heart disease’ (defined as any mitral or aortic valvular disease graded on echocardiography as ≥2/4 for regurgitation or ≥ moderate for stenosis), ‘chronic obstructive pulmonary disease’ and a history of thyroid disease.
The CHA2DS2-VASc-score was used to assess the appropriateness of anticoagulant therapy according to the international guidelines.11 As the study was conducted before publication of the 2012 focused update, the 2010 guidelines were used.12 Based on these recommendations, appropriate treatment for patients at low risk for thromboembolic complications (CHA2DS2VASc=0) is no antithrombotic treatment or aspirin treatment, for patients with intermediate risk (CHA2DS2VASc=1) it is aspirin or oral anticoagulation (OAC) treatment, and for high-risk patients (CHA2DS2VASc≥2) OAC treatment is indicated. Drugs prescribed as maintenance therapy including OAC therapy, platelet inhibitors, rate and rhythm control therapy were all recorded.
Statistical analysis
Descriptive statistics for continuous data included mean and SD for normally distributed data, and median and IQR (Q1–Q3) for non-normally distributed data. Categorical data are presented as absolute frequencies and percentages. Logistic regression was used to correct for age in testing gender differences. Differences were tested with two-tailed t tests and χ2 tests. P values <0.05 were considered statistically significant. All analyses were performed using SPSS V.21.0.
Patient anonymity was guaranteed and the data were only used for the present study.
Results
AF prevalence
The 36 included hospital wards comprised a total of 991 beds. At the day of measurement, 887 (89.5%) beds were occupied (figure 1). Seventy-five (8.5%) patients had exclusion criteria (age, language, isolation), leading to 812 eligible patients, 66 (8.1%) of which refused participation (reasons: ‘pain’, ‘fatigue’, ‘on telemetry’, ‘already ECG taken’ or ‘no consent’ without specific reason); 21 (2.6%) were not able to give permission; and 78 (9.6%) were absent after three ward visits. Hence, 647 patients participated (response rate =79.7%). Non-assessable ECGs were recorded in 11 participants, leading to a study population of 636 patients.

Flow diagram showing patient recruitment and analysis, leading to estimates of AF point prevalence and AF prevalence. IC, informed consent; AF, atrial fibrillation.
AF and atrial flutter were detected in 52 and 6 patients, respectively, reflecting a hospital point prevalence of 9.1% (95% CI 6.9% to 11.3%). Only one new diagnosis of AF was made among those patients. Of the remaining 578 participants, 49 (8.5%) had a medical history of AF based on chart review. Hence, 107 AF cases were identified, yielding a total prevalence of 16.8% (95% CI 13.9% to 19.7%).
Patients with AF were detected in every hospital zone, with prevalence rates of 29.3% (95% CI 22.2% to 36.4%) in zone ‘thorax’; 21.7% (95% CI 14.8% to 28.6%) in ‘internal medicine’; 11.6% (95% CI 5.2% to 18%) in ‘oncology’; 7.6% (95% CI 3.1% to 12.1%) in ‘abdomen’, 7.5% (95% CI 0.4% to 14.6%) in ‘reproduction and growth’; and 5.8% (95% CI 0% to 12.1%) in ‘locomotor system’. In zone ‘sensory system’ a prevalence of 33.3% (95% CI 2.3% to 63.7%) was measured, but it only concerned three out of nine patients. Almost half of the patients with AF were hospitalised in zone ‘thorax’ (43%) followed by ‘internal medicine’ (28%), ‘oncology’ (10.3%) and ‘abdomen’ (9.3%).
Characteristics of patients with AF
Hospitalised patients with AF were significantly older than patients without AF (78.7±10.3 years vs 62.7±15.9 years; p<0.001) (table 1). Most patients with AF, 72.9%, were 75 years or older. AF prevalence was slightly higher in men (19.1%) than in women (14.3%), which was statistically significant when corrected for age (p=0.031; OR=1.678; 95% CI 1.049 to 2.684).
Characteristics of hospitalised patients with and without atrial fibrillation
Among patients with AF, the most common type was permanent AF (48.6%), followed by paroxysmal (24.3%) and persistent AF (20.6%). Only six patients (5.6%) had a single episode of AF (one=new; five=known from before). Of patients with atrial flutter on the index ECG, only one patient did not have a history of AF.
Age distribution of patients with AF
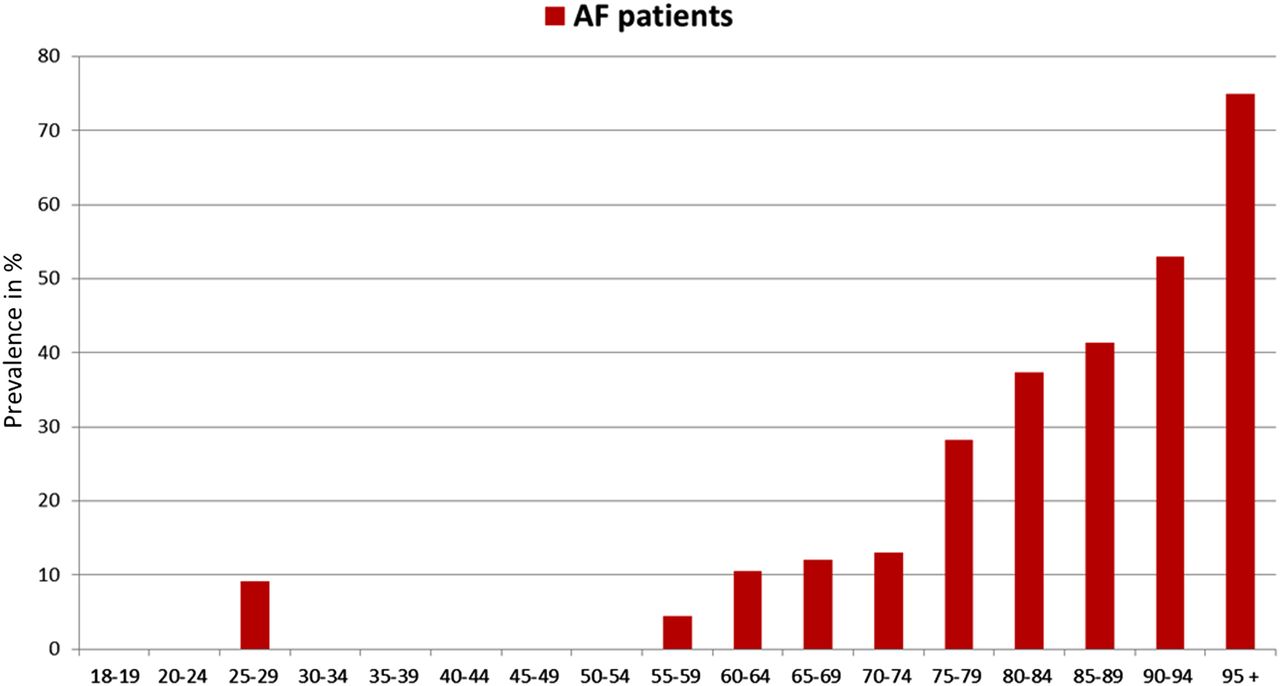
Figure 2 depicts AF prevalence by age group, showing increasing prevalence with age. AF prevalence was 13% in age stratum 70–74 years, nearly tripled to 37.3% in those aged 80–84 years, and was >50% in nonagenarians.
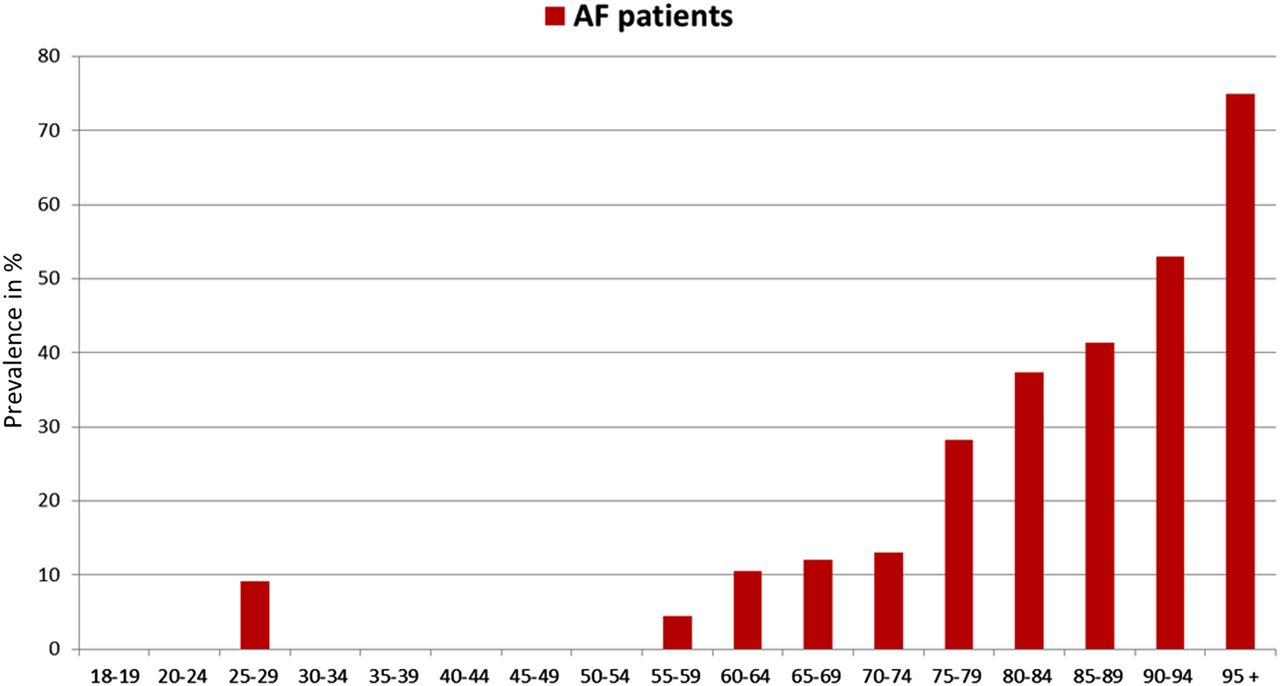
Prevalence of atrial fibrillation (AF) by age group in a study population of 636 hospitalised patients. Prevalence percentages are given per age group.
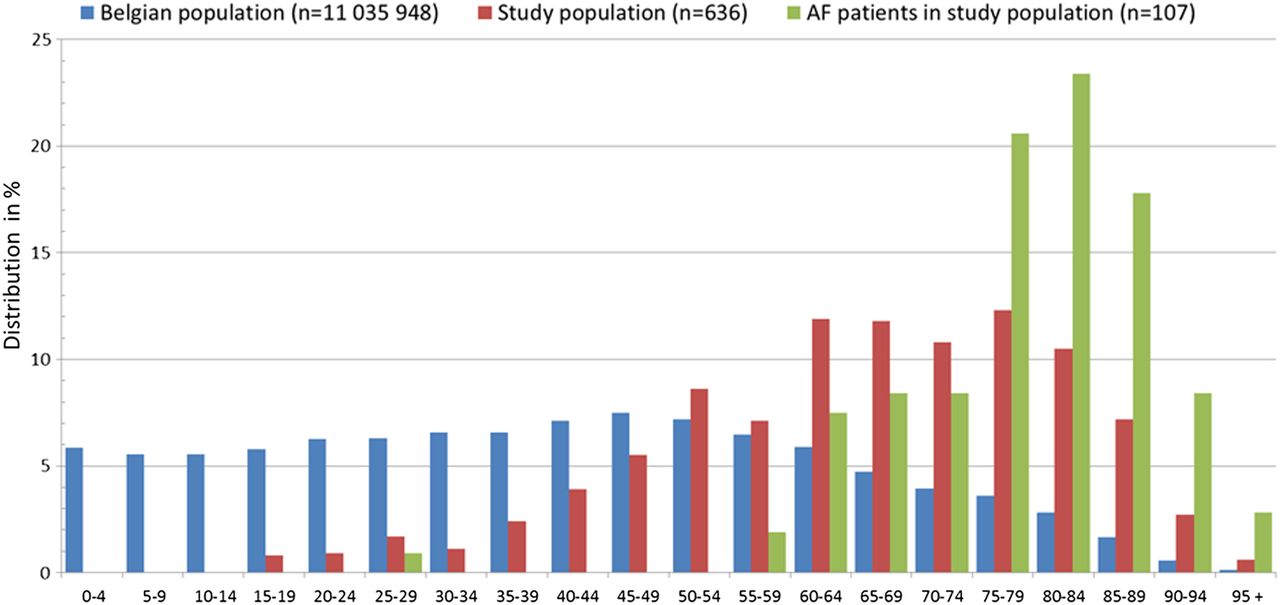
Figure 3 compares the age distributions of all patients in our study, of those with AF, and of the general Belgian population (Status: 1 January 2012; Statistics Bureau Belgium, Department Population). The hospital population in this tertiary care setting is prominently older compared with the Belgian population. Moreover, the distribution of hospitalised patients with AF is shifted towards the oldest age groups.
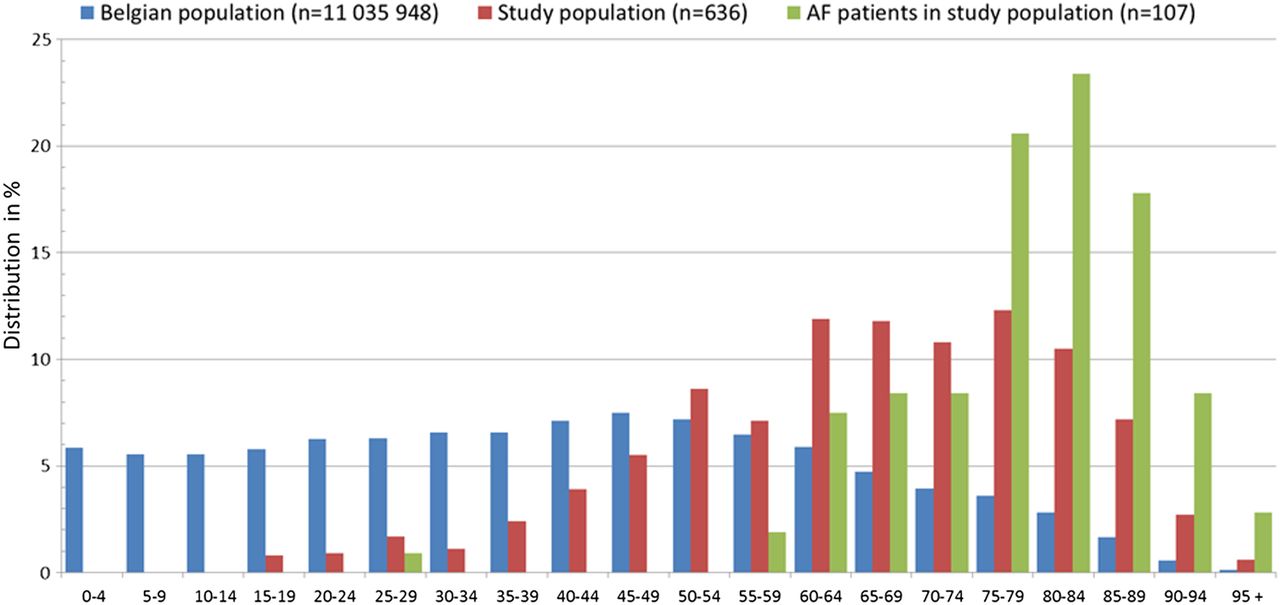
Age distribution of different populations. AF, atrial fibrillation.
Comorbidities of patients with AF
The most common associated comorbidities in patients with AF (figure 4) were hypertension (63.6%), valvular heart disease (58.9%) (electronic supplementary file 1), overweight (body mass index ≥25;54.2%), kidney disease (46.7%; mostly chronic renal impairment), vascular disease (41.1%), congestive heart failure (32.7%) and diabetes (25.2%). A stroke history was reported in 14% and 7.5% had a history of a transient ischaemic attack. No significant differences in comorbidity profile were found between men and women.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of comorbidities in patients with atrial fibrillation (AF). BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; HT, hypertension; KD, kidney disease; LD, liver disease; TD, thyroid disease; TIA, transient ischaemic attack; VD, vascular disease; VHD, valvular heart disease.
Stroke risk factors and medication strategy
Table 2 summarises stroke and bleeding risk profiles of patients with AF. The mean CHA2DS2-VASc-score was 4.1±1.7. Only 2 (1.9%) patients had a low risk (CHA2DS2VASc=0), 6 (5.6%) an intermediate risk (CHA2DS2VASc=1) and 99 (92.5%) a high risk (CHA2DS2VASc≥2) for stroke. The mean HAS-BLED score was 2.5±1.1 and 52% had a high bleeding risk (HAS-BLED≥3).
Stroke and bleeding risk factors and other comorbidities
In table 3 the anticoagulation regimen of patients with AF is plotted versus CHA2DS2-VASc-score. One of the two patients with low risk for stroke was possibly overtreated by receiving anticoagulation therapy (AC). All but one patient with intermediate risk for stroke (n=5; 83.5%) received appropriate treatment (aspirin (n=1; 16.5%) or AC (n=4; 67%)). In the group with high risk for stroke 49 patients (49.5%) received appropriate long-term AC; 32 (32.4%) were undertreated with aspirin therapy alone (n=16), double antiplatelet therapy (n=8) or no AC (n=8); and 18 (18.1%) were possibly overtreated with a combination of anticoagulants and antiplatelet agents. Of the 32 undertreated patients with high risk for stroke, 9 were hospitalised in zone internal medicine, 4 in abdomen, 3 in oncology and 16 in thorax, while only 4 were hospitalised in a non-surgical cardiovascular ward.
Anticoagulant treatment strategy in hospitalised patients with AF per specialty, according to CHA2DS2-VASc-score
Overall, only half of the hospitalised patients with AF (n=55; 51.3%) did receive an appropriate AC, while nearly a third (n=33; 31%) were undertreated and a fifth (n=19; 17.7%) were possibly overtreated. Of all patients receiving AC (n=72), 56 patients were on OAC. Within the group of patients receiving OAC (n=56), 1 was treated with rivaroxaban (1.8%), 6 with dabigatran (10.7%) and 49 took a vitamin K antagonist (87.5%).
Reasons for not providing AC to patients at moderate to high risk for stroke were: ‘fall risk’(n=6;18.2%);‘postoperative AF’(n=5; 15.2%);‘history of bleeding’(n=4; 12.5%);‘palliative care’(n=3; 9.1%);‘patient refusal’(n=3; 9.1%);‘non-adherence’ (n=3; 9.1%);‘age’(n=2; 6.1%); ‘haemophilia B’(n=1; 3.0%); ‘thrombopenia’(n=1; 3.0%) and ‘Hydrea therapy for thrombocytosis’(n=1; 3.0%). Sometimes more than one reason was given, while in 10 patients (30.3%) no reasons were found. A valuable reason for possible overtreatment was found in 12 patients (63.2%) (‘coronary disease’(n=9; 47.4%);‘endoprosthesis’(n=3; 15.8%)), while reasons were unclear or invalid in 7 patients (36.8%) (‘reason unclear’(n=3; 15.8%),‘valve replacement’(n=2; 10.5%);‘pulmonary embolism’(n=2; 10.5%)).
Discussion
The purpose of this cross-sectional study was to assess the point and overall prevalence of AF in a hospitalised population. We also investigated the appropriateness of patients’ longer-term anticoagulant treatment. The main finding was a remarkable high point and overall prevalence of AF, with almost all patients with AF being classified as high-risk patients for stroke. Unfortunately, only half of them were strictly treated in conformance with the anticoagulation guidelines.
An AF point prevalence of 9.1% and especially an overall prevalence of 16.8% in a hospital population is considerably higher than the current estimates of the overall prevalence of 2.3–3.4% in the general population.1 ,3 ,5 ,9 ,22 There have been prior reports on AF prevalence in hospitalised patients but none of these were measured in a hospital-wide setting: some were restricted to only cardiovascular patients or those with acute medical admissions (with rates ranging, respectively, between 8–14%16 ,19 and 2.8–10.4%17 ,18), while others combined inpatients and outpatients.20 Our study included patients hospitalised in all hospital zones (including those without cardiovascular expertise in the medical team), and surprisingly detected patients with AF in every zone.
As expected, AF prevalence in our study steeply increased with age3 ,5 ,6 ,22 and was most prevalent in the 75+ years age group as is also seen in the general population.2 ,22 However, the age-stratified prevalence was also substantially higher than in the general population, with rates of 12% in patients aged 65–69 years to 37% in patients aged 80–84 years (compared with 5% to 15%, respectively, in community-based studies4 ,8 ,9 ,20). This indicates that the higher AF prevalence in a hospital population is due to a higher average age than the general population (as was shown in figure 3), and to a higher prevalence of AF-promoting comorbidities. Hospital populations are known to contain patients with more than one comorbid disease, further increasing with age.23 In the present study, most AF-related comorbidities were in line with prior insights: hypertension is by far the most common AF-related condition. Furthermore, also valvular disease, vascular disease, congestive heart failure and diabetes were common (figure 4), in line with prior findings.3 ,4 ,9 ,23 ,24 However, we found a higher prevalence of chronic kidney disease (35%) and thromboembolic antecedents (14%), compared with 8–17% and 6–8%, respectively, in other studies.4 ,24 A possible explanation again could be the older age distribution in our hospital population as both conditions are clearly related to ageing.23
The present study recorded suboptimal pharmacological antithrombotic treatment of patients with AF when evaluated based on their CHA2DS2-VASc-score, confirming the gap between evidence-based care and real-life practice.16 ,25 Hospitalised patients have a high risk for stroke (93% in our sample had a CHA2DS2-VASc-score≥2). Most overtreatment (63.2%) could be explained by a reasonable explanation (like a recent acute coronary syndrome), while underuse could not be explained in 33.3%. Our study confirms observations from the Euro Heart Survey that more patients are undertreated than overtreated.25 Another study in stable outpatients with AF with high risk for stroke found that 41% was undertreated, which is even higher than in the hospitalised patients with AF of the present study (31%).26 Undertreatment of high-risk patients is still a major problem in the implementation of guideline-recommended antithrombotic management in AF. The Euro Heart Survey authors also demonstrated that undertreatment leads to adverse outcomes much more commonly than overtreatment. Our study found that 87.5% of the undertreated high-risk patients were hospitalised in non-cardiac wards, indicating that non-adherence to the guidelines is a bigger problem in those wards than in non-surgical cardiac wards. The reasons for undertreatment in the present study indicate that physicians’ clinical judgement incorporates factors beyond those included in the CHA2DS2-VASc-score, like ‘fall risk’, ‘postoperative AF’, ‘palliative care’, ‘non-adherence’, ‘high age’ or ‘comorbidity’ that are considered as contraindications for OAC. According to Nieuwlaat et al27 other possible factors contributing to this undertreatment could be knowledge deficit of the guidelines; distraction by other medical problems, no management by an AF specialised physician or the absence of an OAC monitoring outpatient clinic. All underscore the need for a more structured and hospital-wide decision support system.
Indeed, the above-described findings of our study illustrate that hospital-wide support to deliver optimal guideline-based treatment to patients with AF is needed, especially in non-cardiac wards. Education on stroke prevention for patients with AF should focus on the importance of tailoring antithrombotic therapy according to patient's risk profile. Extra improvement might be achieved by integrating stroke risk stratification guidelines in supporting information technology27 with automatic alerts that highlight patients with AF. This can remind physicians to evaluate the risk profile and antithrombotic therapy, even if patients are hospitalised for other reasons. Structural support by interdisciplinary AF expert programmes relying on specialised nurses may be very important for hospitals to guarantee hospital-wide optimised care for patients with AF as comorbidity.10 ,14 ,15 This is the case in at least 16% of the hospital population. This prevalence may further increase due to the aging population and increasing complexity of hospitalised patients. Early recognition of AF, management to prevent stroke and other AF-related morbidity, management of underlying diseases, proper measures perioperatively or during intercurring events, and proper follow-up will become increasing challenges. There is growing evidence and general acceptance for similar hospital-wide services for other conditions, like diabetes, decubitus, stroke and geriatric support.28–31 The AF prevalence rate that we recorded is even higher than the reported 11% prevalence of diabetes among hospital inpatients,28 underscoring the need for similar services for patients with AF.
Limitations
First, although already high AF prevalence rates were measured, we still may have underestimated the real prevalence given a response rate of 79.3%, the reliance on chart review for documentation of a known history of AF, and the exclusion of patients hospitalised in critical care units. Literature reports of AF prevalence in non-cardiac surgical intensive care units range from 5% to 10%, in medical intensive care units from 6% to 26% and after cardiac surgery from 10% to 65%.32 Second, as the present study only collected data at one single tertiary care centre, the generalisability of the results to other hospital settings is unclear. A tertiary hospital might see more patients with AF, as hospitalised patients might have more comorbidities and more severe illnesses leading to AF compared with other hospitals. Furthermore, the particular position of a tertiary hospital within healthcare environment and the structure of the hospital itself might also influence the prevalence of AF. As the prevalence on a single day might vary over time, this can also comprise the generalisability, although the large sample size makes the assessment relatively robust. Third, guideline adherence to rate and rhythm control were not explored in the present study. Finally, this study did not evaluate the comorbidity profile in the large group of patients without AF. Therefore, differences with the hospital population with AF could not be evaluated.
Conclusion
This ECG-based evaluation of nearly the whole patient population in a tertiary care centre on a single day revealed clearly high AF prevalence rates, with a point prevalence of 9.1% and an overall prevalence of 16.8%. Patients with AF were present in all hospital zones, and almost all patients with AF were at high risk for stroke. Anticoagulation management was likely inappropriate in half of those. Overtreatment was often justifiable but undertreatment of high-risk patients is still a major problem, even in a hospital population. Our results highlight the need for new strategies to improve the implementation of guideline-recommended management to guarantee hospital-wide optimised care for patients with AF. Which structured support system(s) would best attain such goal requires further research. We hope that our observations stimulate such endeavours.
Key messages
What is already known on this subject?
-
Atrial fibrillation (AF) is known as an evolving epidemic, however, no quantitative data exist on the overall prevalence of AF and its distribution in a hospital setting across all wards. It can be anticipated that the prevalence of AF in a hospital setting, with likely older patients who have more comorbidities, is higher compared with the community.
What might this study add?
-
This ECG-based evaluation of nearly the whole patient population in a tertiary care centre on a single day revealed a high point prevalence of 9.1% and an overall prevalence of 16.8%. Patients with AF were present in all hospital zones, and almost all patients with AF were at high risk for stroke (CHA2DS2-VASc-score≥2). Only 51.3% of all patients did receive anticoagulant long-term management conforming with the European Society of Cardiology (ESC) guidelines, while 31% were undertreated and 17.7% were possibly overtreated.
How might this impact on clinical practice?
-
The findings of this study illustrate that hospital-wide support to deliver optimal guideline-based treatment to patients with AF is needed, especially in non-cardiac wards. Early recognition of AF, management to prevent stroke and other AF-related morbidity, management of underlying diseases, proper measures perioperatively or during intercurring events, and proper follow-up are all growing challenges.
Acknowledgments
The authors thank all the participants, as well as all nurses of the 36 included hospital wards for hosting the research team. The authors especially thank the many master students in nursing science for their help with the data collection, and Mrs M Tillekaerts and Mr K Schoonjans for their logistic support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All coauthors contributed to conception and design, revising the manuscript critically for important intellectual content and final approval of the version to be submitted.
-
Funding Publication of this article was not funded. DB received partial research fellowship funding through the University Hospitals Leuven. HH received unconditional research grants through the University of Leuven from St Jude Medical, Medtronic, Biotronik and Boston Scientific.
-
Competing interests HH was holder of the AstraZeneca Chair in Cardiac Electrophysiology, University of Leuven. HH is a member of the scientific advisory board of Biosense Webster, St Jude Medical, Siemens Medical Solutions, Boehringer-Ingelheim, Bayer and Sanofi-Aventis, and acted as speaker for Bayer, Boehringer-Ingelheim, Daiischi-Sankyo, BMS-Pfizer, Biotronik, Merck and Sanofi-Aventis.
-
Ethics approval This study was conducted with the approval of the Medical Ethics Committee of the University Hospitals Leuven, Belgium.
-
Provenance and peer review Not commissioned; externally peer reviewed.