Article Text

Abstract
Objective To assess late outcome after transcatheter aortic valve implantation (TAVI) up to 6 years and to analyse its predictive factors with a particular emphasis on functional status. Very few data exist on the long-term results of TAVI, and these data are crucial for decision making.
Methods Between October 2006 and December 2009, 123 consecutive patients were discharged alive after TAVI in our institution. Mean age was 82±8 years, and 88% of patients were highly symptomatic in New York Heart Association (NYHA) class III–IV.
Results Follow-up was complete in 122 patients (99%). The overall 6-year survival rate was 31%±5%, the majority of deaths being non-cardiac. Predictive factors of late mortality were the presence of lower limb arteritis (p=0.009), a higher Charlson comorbidity index (p=0.03) and post-TAVI paraprosthetic aortic regurgitation ≥2/4 (p=0.01). Late outcomes according to Valve Academic Research Consortium-2 criteria were analysed, and the 5-year event-free survival rate was 28%±4%. Finally, the rate of good functional results, defined as survival in NYHA class I or II, was 32%±5% at 5-year follow-up. In the survivors, the EQ-5D questionnaire further confirmed the benefit in terms of quality of life.
Conclusions About one-third of patients discharged alive after TAVI were alive at 6-year follow-up, and the survivors exhibited good functional results assessed by NYHA class and quality-of-life standardised evaluation.
Statistics from Altmetric.com
Introduction
Degenerative aortic stenosis (AS) affects elderly patients who often have a number of comorbidities. Transcatheter aortic valve implantation (TAVI) is indicated for patients unsuitable for surgery and should be considered in cases of high surgical risk.1 ,2 In this particular population, TAVI significantly reduces mortality compared with natural history.3 Long-term results are a crucial contribution to decision making. However, few studies reported follow-up results over 3 years after TAVI.4–6
The aim of this study was therefore to analyse long-term outcome up to 6 years after TAVI and its predictive factors, as well as focusing on late functional results based on the New York Heart Association (NYHA) class and quality of life (QoL).
Methods
Population
This study is a prospective single-centre registry of consecutive patients who were referred to our institution from October 2006 to December 2009 with severe AS responsible for cardiac symptoms (NYHA class II or higher, syncope or angina), and who were considered to be unsuitable or at high risk for surgery after evaluation by the Heart Team according to the guidelines.1 ,2 Because the aim of this paper was to evaluate long-term outcomes after TAVI, we only included in these analyses the patients who were discharged alive.
Index hospitalisation
As for description of the population, lower limb arteritis was defined as claudication or previous or planned intervention on the limb arteries. We used the age-adjusted Charlson comorbidity index to assess patients’ comorbidities. The variables of the Charlson comorbidity index are detailed in online supplementary table S1.
Both the Edwards SAPIEN and the Medtronic CoreValve System were used in the study. The Edwards SAPIEN was used from the beginning of our experience while the Medtronic CoreValve System was available only from November 2008. Patients were selected for either transfemoral or transapical approach on the anatomy of iliofemoral arteries. Transfemoral access was favoured as the first approach, but transapical access was also used. Moreover, one patient benefited from subclavian access and one patient from retroperitoneal access.
Transthoracic echocardiographic examinations were systematically performed at baseline and at day 7 after TAVI by experienced echocardiographers. The severity of aortic regurgitation (AR) was graded from 0 to 4 using an integrative approach as recommended by guidelines.2 ,7 ,8
After TAVI, patients were treated with aspirin and clopidogrel for 3 months, followed by a single antiplatelet therapy, which was continued lifelong. When oral anticoagulation was indicated, patients were treated with a vitamin K antagonist and only one antiplatelet agent.
Follow-up
Follow-up was conducted through clinical visits, phone contact with the referring cardiologist or general practitioner or direct phone contact with the patient. Data were prospectively entered in a computerised database. Follow-up was concluded in December 2013. Patients were considered lost to follow-up if they were still alive but their last contact was before January 2013. Follow-up was complete in 122 patients (99.2%). The median follow-up was 3.6 years, IQR (2.6–4.7), and maximum follow-up reached 6 years.
The performance of echocardiographic examinations during follow-up was left to the discretion of patients’ cardiologists.
QoL follow-up was assessed using the EuroQol with EQ-5D questionnaire and a visual analogical scale.9
Endpoints
The events taken into account during follow-up were death, NYHA functional class III or IV, stroke, severe bleeding and hospitalisation for congestive heart failure or prosthetic dysfunction according to the Valve Academic Research Consortium-2 (VARC-2) criteria.10
Clinical events occurring during follow-up were combined in the following endpoints: (1) overall survival, (2) survival considering only cardiovascular-related death, (3) event-free survival according to VARC-2 criteria and (4) good functional results defined as survival in NYHA functional classes I or II.
The cause of death was classified as cardiac or non-cardiac. If the cause remained unknown, it was specified in the events table, but considered to be cardiovascular related for the cardiovascular survival analysis according to the VARC-2 criteria.10
Statistical analysis
Quantitative variables were expressed as mean±SD. Qualitative variables were expressed as percentages.
The univariate analysis of factors associated with in-hospital mortality used t test for quantitative variables and χ2 test for qualitative variables. Before conducting t tests, the normal distribution of the variables using a Kolmogorov–Smirnov test was verified. All the variables with p<0.10 were included in a multivariate logistic regression using a backward selection procedure with p<0.05.
Survival curves were obtained with Kaplan–Meier estimates. Comparisons between survival curves were obtained using a log-rank test. The univariate analysis was performed using a Cox model on the 40 variables of table 1. Only the factors that were statistically significant in the final multivariate Cox regression model were reported in the tables. Proportional hazard assumption was assessed by including interactions with log-time in the final Cox models and from the graphical analysis of Schoenfeld residuals.
Baseline and periprocedural characteristics of the population
Predictive factors of late results identified by univariate analysis with p<0.10 were included in a multivariate Cox analysis with backward selection using a threshold of p<0.05.
The results were considered significant when two-sided p values were <0.05. All analyses were performed with the SPSS statistical software package (SPSS V.19, Chicago, Illinois, USA).
Results
Between October 2006 and December 2009, 141 patients consecutively underwent TAVI in our institution, of whom 18 (13%) died during hospitalisation. We identified two independent predictive factors of early mortality: approach other than transfemoral (mainly transapical route) (adjusted OR 5.9, 95% CI (1.9 to 19.0); p=0.003) and severe bleeding after the procedure (adjusted OR 7.0, 95% CI (2.0 to 24.1); p=0.002). Since the aim of the paper was to evaluate long-term results, we then performed all analyses on the 123 surviving patients. Of them, 4 underwent TAVI in 2006, 12 in 2007, 56 in 2008 and 51 in 2009.
The mean age of the population was 82 years, and most patients were highly symptomatic with 88% in NYHA class III or IV. The baseline and periprocedural characteristics of the population are described in table 1.
More than 90% of procedures used the Edwards SAPIEN prosthesis, and 68% of the approaches were transfemoral.
Immediate results
Successful deployment of the valve was achieved in all 123 patients. However, six patients experienced an AR ≥3/4 for which five benefited from balloon postdilatation and one underwent implantation of a second valve (valve-in-valve) during the same procedure due to a too low positioning of the first valve. At the end of the procedure, AR was ≤2/4 in all but one patient. Severe vascular complications occurred in 17 patients (14%) and severe bleeding in 11 (9%). Four patients (3%) suffered from stroke after the procedure but during the index hospitalisation.
Mean aortic valve gradient was 50±15 mm Hg before TAVI. At day 7, mean aortic valve gradient was 11±4 mm Hg, paraprosthetic AR was ≥2 in 12 patients (10%) while mitral regurgitation ≥2 was present in 14 patients (11%) (table 1).
Long-term survival
During follow-up, 77 patients died (63%). The cause of death was cardiac in 25 patients (33%), the majority being due to congestive heart failure (n=13). The other cardiac causes were sudden death (n=6), myocardial infarction (n=2), pulmonary embolism (n=1), stroke (n=1), infective endocarditis (IE) (n=1) and aortic dissection (n=1). The cause of death was non-cardiac in 44 patients (57%) and unknown in 8 patients (10%). Thus, the cardiac deaths as defined by VARC-2 criteria finally accounted for 43% of all deaths.
As illustrated in figure 1, the 6-year survival rate was 31%±5%. The respective survival rates at 1, 2, 3, 4 and 5 years were 84%±3%, 73%±4%, 56%±4%, 46±5% and 37%±5%.

Overall survival at 6-year follow-up after transcatheter aortic valve implantation in patients discharged alive.
In univariate analysis, we identified nine predictive factors of late death after TAVI (table 2), seven being preprocedural and two postprocedural variables (see online supplementary figure S1). No procedural variable (type of valve and access) impacted the late results in this study.
Predictive factors of late death
The multivariate analysis identified three predictive factors of late death after TAVI (table 2): the presence of lower limb arteritis (p=0.009), a higher Charlson comorbidity index (p=0.03) and post-TAVI paraprosthetic AR ≥2/4 (p=0.01).
Finally, the survival rate without cardiovascular death was 66%±5% at 6 years.
Events during follow-up
The events are detailed in table 3 according to the vital status of patients.
Events occurring during follow-up after TAVI
The majority of patients (78%) had to be rehospitalised, mostly due to non-cardiac causes (56%). Three patients had IE 4, 19 and 29 months, respectively, after TAVI. The causative microorganism was Streptococcus bovis in one case and methicillin-sensitive Staphylococcus aureus in the other two cases. No patient required reintervention. One patient died from septic shock due to his IE, while the other two deaths were not related to IE.
Late permanent pacemaker implantation was necessary in 15% of the patients. The only independent predictive factor of pacemaker implantation was the use of a CoreValve prosthesis (adjusted HR 4.0, 95% CI (1.3 to 12.2); p=0.016). Late strokes occurred in 16 patients (13%), either ischaemic (12 patients) or haemorrhagic (4 patients), and 7 (44%) were fatal. Cumulative major stroke rates at 6 years were 16%±4%. There was no difference in the rate of strokes according to the presence or absence of atrial fibrillation (16.2%±7.0% and 17.0%±5.0%, respectively, p=0.42) (figure 2). We identified three independent predictive factors of stroke after TAVI: older age (adjusted HR 1.2, 95% CI (1.0 to 1.3); p=0.003), previous cerebrovascular accident (adjusted HR 3.8, 95% CI (1.1 to 12.5); p=0.03) and higher creatinine level (adjusted HR 1.01, 95% CI (1.00 to 1.01); p=0.0001).
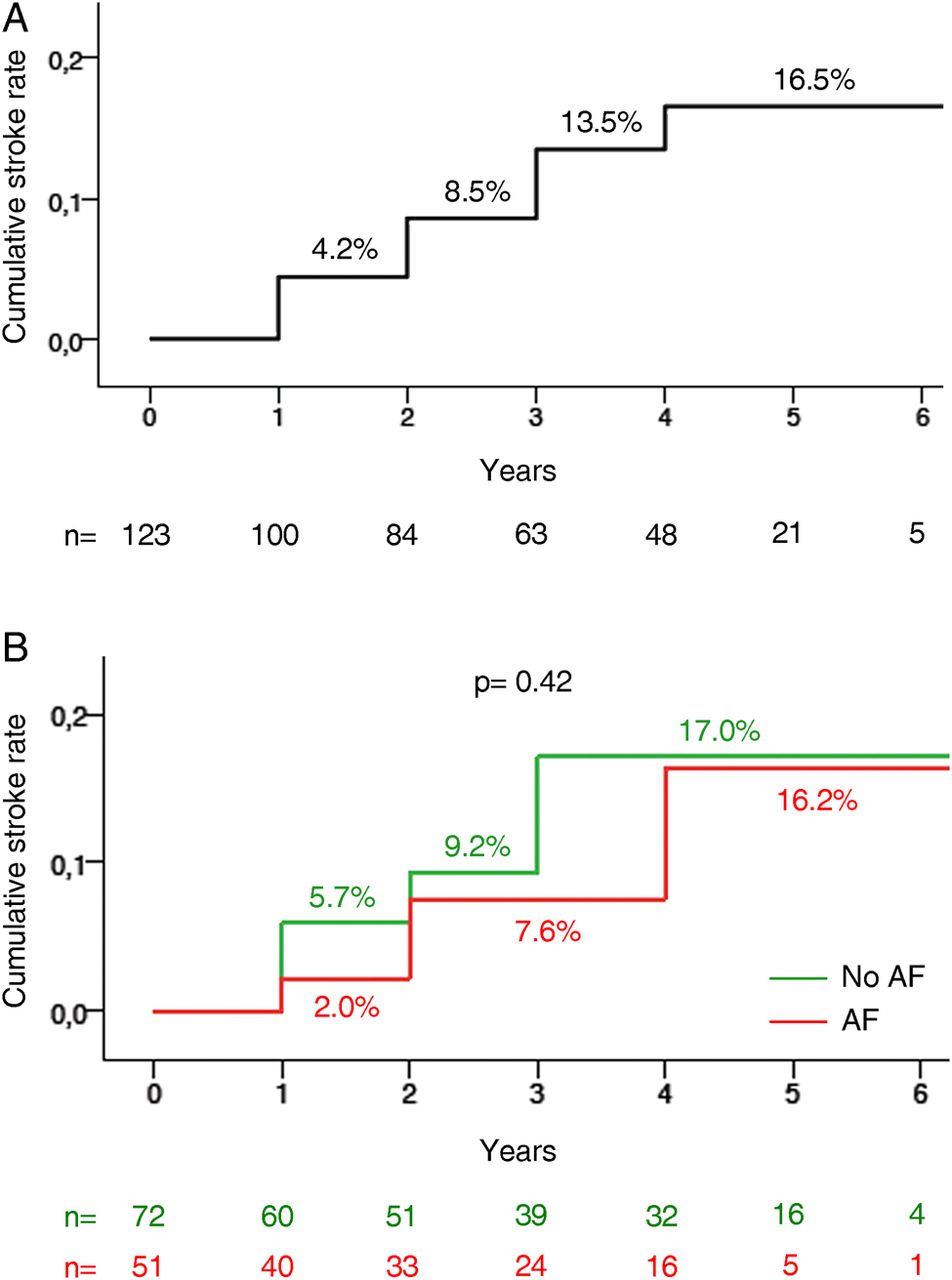
Cumulative rates of major stroke at 6 years after transcatheter aortic valve implantation. (A) Overall population. (B) Cumulative rates of stroke according to the presence or absence of atrial fibrillation (AF).
Functional status
Among the 45 survivors at last follow-up after TAVI, 33 patients (73%) were in NYHA functional class I or II. The evolution of the NYHA class before and after the procedure is illustrated in figure 3. The rate of good late functional results, defined as survival in NYHA class I or II at last follow-up, was 32%±5% at 5 years.

New York Heart Association (NYHA) class before and at last follow-up after transcatheter aortic valve implantation among the 45 survivors.
In univariate analysis, we identified seven predictive factors of poor late functional results, five being preprocedural and two postprocedural variables (see online supplementary table S2).
In multivariate analysis, three factors were predictive of poor late functional results after TAVI (see online supplementary table S2): the presence of lower limb arteritis (adjusted HR 1.90, 95% CI (1.07 to 3.37); p=0.03), a higher postprocedure systolic pulmonary artery pressure (PAP) (adjusted HR 1.02, 95% CI (1.00 to 1.04); p=0.03) and postprocedure paraprosthetic AR ≥2/4 (adjusted HR 2.32, 95% CI (1.18 to 4.56); p=0.01).
In 41 out of the 45 survivors (91%), the EQ-5D questionnaire and the visual analogical scale of QoL were performed. The QoL assessment was not feasible in five patients because of neurological impairment or refusal. According to this questionnaire, 33% of patients could walk easily, 76% had no problem with self-care, 50% had no difficulties in performing their usual activities, 50% were pain free and 50% were neither anxious nor depressed. According to the visual analogical scale of QoL, with the best imaginable state being 100 and the worst state being 0, the mean score was 64±12 in our population.
VARC-2 criteria
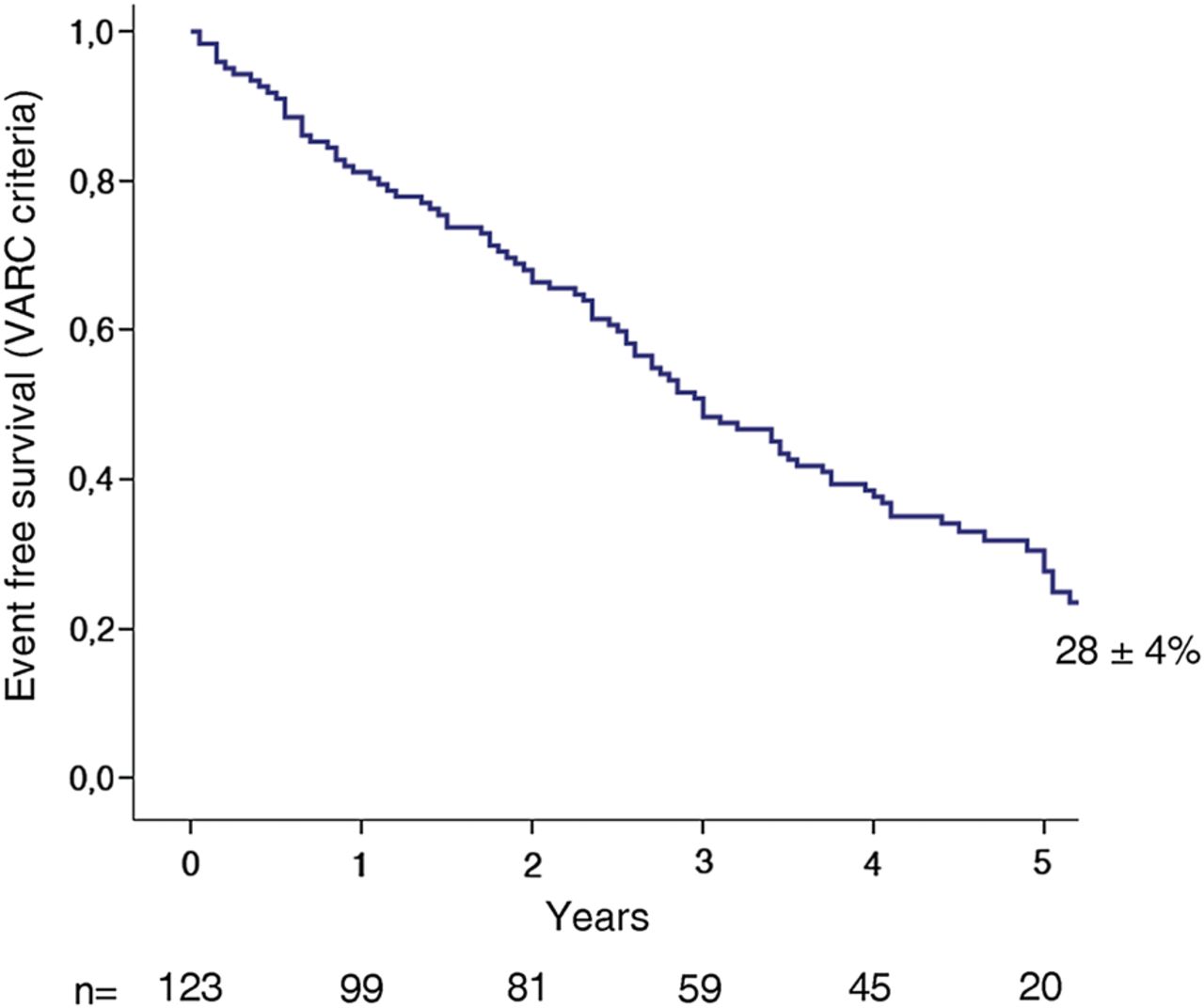
At 5-year follow-up, 28%±4% of patients were alive, in NYHA class I or II, and were free from stroke, major bleeding and hospitalisation for congestive heart failure or prosthetic dysfunction (figure 4). In univariate analysis, we identified seven predictive factors of late results, four being preprocedural and three postprocedural variables (see online supplementary table S3). In multivariate analysis, we identified two predictive factors of late events according to the VARC-2 criteria (see online supplementary table S3): a higher Charlson comorbidity index (adjusted HR 1.13, 95% CI (1.03 to 1.25) per one-unit increase; p=0.01) and postprocedure paraprosthetic AR ≥2/4 at day 7 (HR 2.32, 95% CI (1.19 to 4.53); p=0.01).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Event-free survival (events defined according to the Valve Academic Research Consortium-2 (VARC-2) criteria as death, New York Heart Association III–IV, stroke, haemorrhage, hospitalisation for congestive heart failure or aortic prosthesis dysfunction) at 5-year follow-up in patients discharged alive after transcatheter aortic valve implantation.
Valve-related dysfunction
At last follow-up, five patients had prosthetic dysfunction, of whom two died: one patient had stenosis (mean gradient of 23 mm Hg) at 1.3 years and died 7 months later from unknown cause, while the other had intraprosthetic AR grade 4 at 2.0 years due to IE and died from haemorrhagic shock 4 months later. Among the survivors, two patients had stenosis (mean gradient of 20 mm Hg at 5.0 years' follow-up in the first case, and 25 mm Hg at 3.2 years in the second case), and one patient had intraprosthetic AR grade 3 at 4.8 years' follow-up. No patient required reintervention for valve failure. All prosthetic dysfunction occurred on Edwards SAPIEN devices, which represented >90% of the valves implanted in this study.
Discussion
The present study, reporting the longest follow-up after TAVI, shows that almost one in three patients, surviving after TAVI, were still alive at 6 years. In most cases, late death was non-cardiac. Furthermore, among the survivors, three out of four patients were in NYHA class I or II, with good QoL, showing the durability of the improvement of functional status after TAVI. The main predictive factors of late outcome were lower limb arteritis, Charlson index, paraprosthetic AR ≥2/4 and post-TAVI systolic PAP.
Long-term survival
All-cause survival at 6 years was 31%±5%. The interim survival was consistent with previous reports.5 ,6 The linearity of the curve suggests a constant mortality rate over time. This continuous attrition is largely due to the weight of comorbidities, as attested by the fact that more than half of the deaths were related to non-cardiac causes. This is consistent with the 6-year cardiovascular survival rate of 66%±5%.
Predictive factors of late mortality
It is necessary to identify patients suffering from severe coexisting conditions that may preclude any durable benefit from TAVI. The predictors of late death after TAVI were lower limb arteritis, Charlson comorbidity index and paraprosthetic AR ≥2/4.
The Charlson index is a strong independent predictive factor of survival.11 ,12 Its impact on late mortality in the present series further illustrates the weight of comorbidities in survival after TAVI. Although lower limb arteritis is included in the Charlson comorbidity index, its additional prognostic value in our series suggests a high negative impact of atherosclerosis. Both lower limb arteritis and Charlson comorbidity index are non-modifiable factors, but they should be given particular consideration in the analysis by the Heart Team. We found in this study that a Charlson comorbidity index >5 was associated with a poor late prognosis after TAVI. The decision to perform TAVI is of course multifactorial with an integrative approach, but a high Charlson index may lead to reconsideration.
Paraprosthetic AR ≥2/4 was the only postprocedural factor related to late survival in multivariate analysis in our series. The level of severity at which paraprosthetic AR has an adverse prognostic value remains debated. It has been suggested that mild paraprosthetic AR was benign and well-tolerated,13 whereas it has been identified as an adverse prognostic factor by others.14 Such discrepancies may be partly due to the difficulties in echocardiographic quantification. In a recent meta-analysis on AR post-TAVI, on 12 926 patients across 45 individual studies, there was a clear association between paraprosthetic AR and increased 1-year mortality for moderate AR, whereas this association was less robust for mild AR.15 There is now a large body of evidence with regards to the association between at least moderate AR (grade ≥2/4) and mid-term mortality after TAVI.14–16 Our results confirm these findings, which rely on shorter follow-up.
Functional status
Several studies have shown a significant improvement in functional status and QoL after TAVI.3 ,17–19 A strength of the present study is to confirm the improvement in NYHA class at a longer follow-up. One out of three patients indeed exhibits good functional results 5 years after TAVI.
Lower limb arteritis and postprocedural AR ≥2/4 were associated with poor late functional results in multivariate analysis. Pulmonary artery pressure at day 7 was the third factor associated with late functional results.
Pulmonary hypertension reflects advanced stages of cardiac disease and has been reported as a marker of mid-term and long-term mortality after TAVI.6 ,20–23 In this series, persistence of pulmonary hypertension after TAVI affected late functional results. This further emphasises the negative impact of late referral of high-risk patients with severe AS. This trend for late referral was attested by the fact that only 12% of the patients in our population were in NYHA class II and only 30% had an aortic valve area >0.8 cm2. These characteristics are consistent with other published cohorts.5 ,6 However, this late referral may be partly explained by the fact that the study concerned the beginning of our TAVI programme (2006–2009), with restrictive inclusion criteria and selection of very high-risk and symptomatic patients.
VARC-2 criteria
We report for the first time long-term event-free survival according to the VARC-2 criteria. More than one in four patients were free from any major events at 5-year follow-up, underlining the sustained good results after TAVI. Post-TAVI paraprosthetic AR was consistently associated with survival, good functional results and event-free survival according to VARC-2 criteria. These findings reinforce the adverse prognostic value of at least moderate paraprosthetic AR for most events occurring during long-term follow-up after TAVI.
Study limitations
This single-centre series included a limited number of patients, and larger studies are needed to confirm the predictive factors of late outcomes. However, it allowed for a homogeneous follow-up. This study took place at the beginning of the TAVI programme in our institution, which may have influenced patient selection and procedural parameters and therefore long-term results. The diagnosis of frailty was mainly subjective based on the evaluation of the Heart Team. We chose not to include this parameter since it might have introduced some inaccuracy in the analysis.
The vast majority of patients received the Edwards SAPIEN, the CoreValve being available only at the end of 2008.
Echocardiographic examination was not standardised during follow-up. We thus chose not to specifically analyse changes in valvular function over time.
Conclusion
This series, with the longest follow-up so far, provides encouraging information on survival in patients discharged alive after TAVI. Our results show a sustained improvement in functional status in most patients. This finding is corroborated by objective assessment of QoL, which represents a major goal in this elderly population. Predictive factors of late results underline the need for careful assessment of comorbidities using the Charlson index and confirm the main impact of paraprosthetic AR ≥2/4 on long-term results. Follow-up has to be pursued in existing TAVI cohorts in order to further improve patient selection.
Key messages
-
What is already known on this subject?
-
The results of transcatheter aortic valve implantation (TAVI) have been widely studied, but follow-up is limited to mid-term and seldom over 3 years.
-
What might this study add?
-
This study reports a 6-year overall survival rate of 31%±5% after TAVI. It also includes functional results, indices of quality of life and late outcome according to Valve Academic Research Consortium-2 criteria, with their predictive factors.
-
How might this impact on clinical practice?
-
Long-term outcome after valvular intervention plays an important role in decision making. The identification of predictive factors associated with late outcome contributes to the improvement of patient selection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
-
Competing interests DH is a proctor for Edwards Lifesciences and Medtronic. BI has received consultant fees from Abbott, Boehringer Ingelheim, Valtech, and speaker's fees from Edwards Lifesciences. PN is a consultant for Medtronic and a proctor for Edwards Lifesciences. AV is on the advisory board for Medtronic and receives speaker's fees from Edwards Lifesciences. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
-
Patient consent Obtained.
-
Ethics approval The local review committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.