Article Text

Abstract
Valve stress echocardiography (VSE) can be performed as exercise stress echocardiography (ESE) or dobutamine stress echocardiography (DSE) depending on the patient’s clinical status, severity and type of valve disease. ESE combines exercise testing with two-dimensional grey scale and Doppler echocardiography during exercise. Thus, it provides objective assessment of symptomatic status (exercise test), as well as exercise-induced changes of a series of echocardiographic parameters (different depending on the valve disease type), which yield prognostic information in individual patients and help in a better treatment planning. DSE is useful in symptomatic patients with low-gradient aortic stenosis. It clarifies its severity and helps in assessing surgical risk in patients with severe disease and systolic dysfunction. It can be also used to test valve haemodynamics in asymptomatic patients with significant mitral stenosis unable to perform an exercise test or to test the left ventricle response, namely to test viability, in patients with ischaemic secondary mitral regurgitation. VSE has taught us that history taking, clinical examination and resting echocardiography give an ‘incomplete picture’ of the disease in patients presenting with a severe valve disease. Therefore, its use should be encouraged in such patients.
- echocardiography
- mitral Regurgitation
- mitral Stenosis
- aortic Stenosis
Statistics from Altmetric.com
Introduction
Functional testing at its inception was used to assess symptoms during exertion, and it has evolved to answer several clinical questions with the help of stress echocardiography.1 Valve stress echocardiography (VSE) helps refine diagnosis of severity, prognosis and management planning based on changes in various parameters induced by exercise or by dobutamine.2 3 The indications for VSE have expanded in parallel with the growing evidence for early intervention benefit in valvular heart disease.
Currently, there is extensive evidence that VSE can benefit decision-making for a wide range of patients being followed up in valve clinics or those with newly diagnosed valvular heart diseases.4 Consequently, the recently published European Association of Cardiovascular Imaging and the American Society of Echocardiography joint recommendations for the use of stress echocardiography in non-ischaemic heart disease address the use of stress echocardiography in valvular heart disease.5 VSE is recommended for the following clinical scenarios: corroborating the severity of valve disease with symptoms prior to intervention, detecting severe valve disease with left ventricular systolic dysfunction or other signs of haemodynamic compromise.4 For diagnosis of severe valve disease with symptoms, VSE is performed in two categories of patients: asymptomatic patients with severe valve disease with the aim to detect symptoms and symptomatic patients with non-severe valve disease with the aim to regrade valve disease severity. For diagnosis of severe valve disease with left ventricular systolic dysfunction, VSE is also performed in two categories of patients: patients with low-flow aortic stenosis with the aim to clarify aortic stenosis severity and patients with asymptomatic severe valve disease with the aim to detect subclinical left ventricular systolic dysfunction.6 7 Furthermore, other signs of haemodynamic compromise may be demonstrated with VSE in asymptomatic patients with severe valve disease.8 9 A simplified classification of VSE indications groups them into three categories: severe valve disease without symptoms, non-severe valve disease with symptoms and valve disease with low flow. A more detailed and comprehensive classification of VSE indications assigns them to the respective valve disease.
Methodology
Stress echocardiography with both dobutamine and exercise can be used for the assessment of valvular heart disease, depending on indication and on the aim of the test. Exercise testing can be performed with a treadmill; however, the postexercise rather than during exercise image acquisition in this case may result in peak exercise-related phenomena being underestimated or missed, and low workload-related phenomena cannot be assessed. Ideally, VSE should be performed with supine bicycle exercise to allow imaging throughout the test and particularly at low workload and at peak effort. Imaging at low workload allows assessment of contractile reserve and changes in global longitudinal strain, both helping to detect subclinical left ventricular systolic dysfunction. Furthermore, the increase in systolic pulmonary artery pressure from low workload has higher specificity for a pathological response as haemodynamic consequence of severe valve disease.
Dobutamine stress is the only currently recommended VSE modality for the assessment of low-flow, low-gradient aortic stenosis with reduced left ventricular ejection fraction.10 11 Dobutamine stress can be used as an alternative to exercise in low-flow, low-gradient aortic stenosis with preserved left ventricular ejection fraction and in the assessment of mitral stenosis severity. Dobutamine stress does not allow assessment of systolic pulmonary artery pressure and the assessment of mitral regurgitation severity.
Exercise echocardiography allows the assessment of exercise tolerance and symptoms together with the assessment of haemodynamic parameters under physiological stress. The exercise tolerance is compared with age-matched, sex-matched and weight-matched normals.12 Symptoms of shortness of breath are witnessed and can be occasionally found to be due to cardiac asthma—interstitial pulmonary oedema resulting in prolonged expiration and expiratory wheeze. Being symptoms-limited, the exercise test is usually terminated before development of alveolar pulmonary oedema with wet lungs; on the contrary, alveolar pulmonary oedema may be occasionally induced by dobutamine stress echo in the assessment of low-flow, low-gradient aortic stenosis or mitral stenosis. Exercise echocardiography allows the assessment of systolic pulmonary artery pressure response, of mitral regurgitation severity and of severe mitral regurgitation consequences. Exercise echocardiography allows the assessment of the true left ventricular contractile reserve, as a physiological phenomenon, rather than the left ventricular inotropic reserve, defined as the increase in ejection fraction in response to intravenous dobutamine infusion. Exercise echocardiography is used in the assessment of severe valve disease with no symptoms but also non-severe valve disease with symptoms and paradoxical low-flow aortic stenosis.
Parameters assessed depend on the VSE indication; thus, a specific protocol is used in each case, predefining necessary images and their order of acquisition appropriate for the aim of the test (figure 1).

Schematic representation of different parameters that may be acquired during exercise stress echocardiography in each type of asymptomatic severe heart valve disease. AR, aortic regurgitation; AS, aortic stenosis; Ch, chamber; E, early diastolic wave velocity; ESE, exercise stress echocardiography; LV, left ventricle; MG, mean pressure gradient; MR, mitral regurgitations; MS, mitral stenosis; PISA, proximal isovelocity surface area; SV, stroke volume; TAPSE, tricuspid annular plane systolic excursion; TTG, transtricuspid pressure gradient.
Clinical applications
The VSE clinical application depends on the valve disease in question and on the indication for the test (tables 1 and 2, figures 2–5).
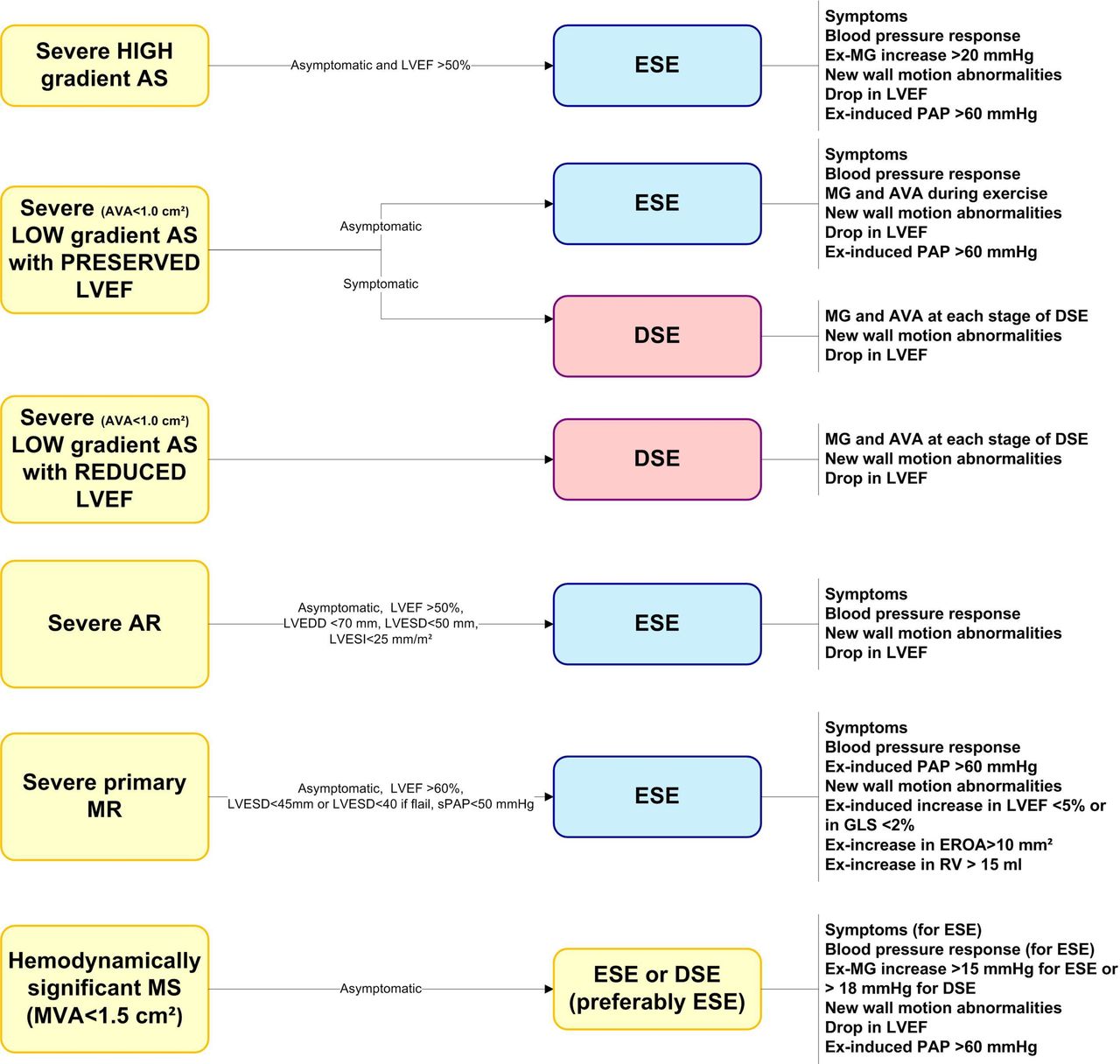
Summary of different valve stress echocardiography modalities and parameters to assess according to each type of heart valve disease. AR, aortic regurgitation; AS, aortic stenosis; AVA, aortic valve area; DSE, dobutamine stress echocardiography; EROA, effective regurgitant orifice area; ESE, exercise stress echocardiography; Ex, exercise; Ex-MG, mean pressure gradient during exercise; GLS, global longitudinal strain; LVEDD, left ventricle end diastolic diameter; LVEF, left ventricular ejection fraction; LVESD, left ventricle end systolic diameter; LVESI, left ventricle end systolic index; MR, mitral regurgitation; MS, mitral stenosis; MVA, mitral valve area; PAP, systolic pulmonary artery pressure; RV, regurgitant volume; sPAP, systolic pulmonary artery pressure.

Exercise stress echocardiography in an asymptomatic patient with severe AS. Rest echocardiographic evaluation confirms the presence of normal-flow, high-gradient severe AS in a patient with preserved left ventricular ejection fraction (>50%) and LV global longitudinal strain, and no pulmonary arterial hypertension (systolic pulmonary artery pressure <50 mm Hg). The patient stopped the test prematurely for leg pain (peak heart rate 102 beats per minute). Several parameters of poor outcome were identified during exercise: an increase in mean transaortic pressure gradient by 19 mm Hg, a rapid increase in LV filling pressure (as assessed by E/e’) and the development of pulmonary arterial hypertension, despite preserved LV contractile reserve (increase in global longitudinal strain (GLS)). AS, aortic stenosis; E, early diastolic wave velocity; LV, left ventricle; MG, mean transaortic pressure gradient; TTG, transtricuspid pressure gradient; Vel, velocity.

Exercise stress echocardiography in an asymptomatic patient with degenerative mitral regurgitation. At exercise the degree of mitral regurgitation increased moderately while the global longitudinal strain decreased, identifying the absence of contractile reserve. EROA, effective regurgitant orifice area; GLS, global longitudinal strain.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Exercise stress echocardiography in an asymptomatic patient with mitral stenosis and significant increase in mean mitral pressure gradient (MG).
Stress echocardiographic parameters in native valvular heart disease
Comparison of exercise versus dobutamine stress echocardiography
In case of asymptomatic severe valve disease, the test should be always performed with exercise stress to detect symptoms and haemodynamic consequences of the valve disease in physiological circumstances, reproducible in daily life. Furthermore, dobutamine stress is contraindicated in severe valve disease, particularly in high-gradient severe aortic stenosis. The administration of dobutamine in severe aortic stenosis can result in cardiogenic shock due to dobutamine-induced peripheral vasodilation with consequent systemic hypotension and concomitant acute pulmonary oedema. Exercise testing to detect symptoms is well established and recommended in all valve disease management guidelines, because symptoms are a class I indication for intervention, although having a subjective nature; furthermore, sedentary patients do not give themselves the opportunity to experience symptoms, and many active patients instinctively slow down their pace to avoid symptoms. In severe valve disease, given that the valve disease severity is already established, VSE image acquisition should begin with left ventricular views, tricuspid regurgitation for systolic pulmonary artery pressure estimation and other parameters suggestive of decompensation, for example exertion-induced mitral regurgitation in patients with aortic valve disease.
In case of symptoms but non-severe valve disease, the test performed with exercise stress allows corroboration of symptoms with exertion-induced changes. However, dobutamine can be used to assess inducible ischaemia as reason for symptoms or to regrade low-gradient aortic stenosis severity. Echocardiography is essential for diagnosis in this case, and the VSE image acquisition should begin with parameters of valve disease severity.
In case of low-flow aortic stenosis, exercise is recommended only if the ejection fraction is preserved and the patient is asymptomatic by history taking. The VSE image acquisition should begin with parameters of valve disease severity and flow reserve, which is the degree of blood flow increase in response to maximal stimulation, with left ventricular views acquired subsequently.
Aortic stenosis
Asymptomatic severe aortic stenosis
Severe aortic stenosis is not an indication for intervention in the absence of symptoms if the left ventricular ejection fraction is preserved. Exercise testing to detect symptoms is long well established in the follow-up of severe aortic stenosis in valve clinics for timing of intervention. The addition of echocardiography provides diagnostic and prognostic parameters.13 Classically, during treadmill exercise testing, ST depression on ECG and drop in systolic blood pressure are indications for intervention.14 15 The ST depression on ECG translates into induced regional myocardial hypokinesia during VSE. Left ventricular ejection fraction drop on exertion and inducible mitral regurgitation are also echocardiographic signs of haemodynamic compromise. Reduced global longitudinal strain at rest and on exertion suggests subclinical left ventricular systolic dysfunction.16 17 Furthermore, mean gradient increase by more than 20 mm Hg is a sign of adverse prognosis, suggestive of possible decompensation during follow-up.8 14
Symptoms despite non-severe aortic stenosis
In patients with non-severe aortic stenosis based on current classification criteria, symptoms should trigger stress testing to regrade aortic stenosis severity based on stress-induced changes of echocardiographic parameters and to detect signs of haemodynamic significance described for severe aortic stenosis.6 7
Classical low-flow, low-gradient aortic stenosis
Low-flow, low-gradient aortic stenosis with reduced left ventricular ejection fraction needs low-dose dobutamine VSE to assess the severity of aortic stenosis and the existence of flow reserve. At rest, because of low transvalvular flow as a result of reduced left ventricular ejection fraction, the echocardiographic assessment of aortic stenosis severity gives contradictory findings with calculated functional aortic valve area in the severe range and gradients in the moderate range. The diagnosis of aortic stenosis severity necessitates assessment of calculated functional aortic valve area and gradients in conditions of increased transvalvular flow as a result of dobutamine.18 19 Gradients increase with no or minimal increase in calculated functional aortic valve area suggest severe aortic stenosis. The assessment of aortic stenosis severity depends on the existence of flow reserve. In case of limited flow reserve, the projected aortic valve area can be used for diagnosis of severity.19 In case of no flow reserve, the assessment of aortic valve calcification with CT may help with the diagnosis.20 Caution is required in case of induced ischaemia with consequent drop in left ventricular ejection fraction; interpretation of findings at this stage as representing a higher flow state would lead to an erroneous diagnosis of non-severe aortic stenosis and lack of contractile reserve.21 To avoid missing the peak increase in flow, continuous acquisition is recommended.
Low-flow, low-gradient aortic stenosis with preserved left ventricular ejection fraction
Low-flow, low-gradient aortic stenosis with preserved left ventricular ejection fraction may benefit from dobutamine or exercise VSE to assess the severity of aortic stenosis, although caution ought to be exercised in patients with small hypertrophic hearts.18 22 An increase in gradients with minimal or no increase in calculated functional valve area during dobutamine stress points towards severe aortic stenosis physiology. Exercise testing allows concomitant assessment of exercise tolerance and symptoms. Often the test with dobutamine or exercise is terminated early due to heart failure symptoms as a result of diastolic dysfunction and intolerance of sinus tachycardia or development of atrial fibrillation.
Aortic regurgitation
In asymptomatic severe aortic regurgitation, exercise testing to detect symptoms is crucial because of the high mortality they portent.23 In both severe and non-severe aortic regurgitation, with or without symptoms, exercise VSE allows assessment of subclinical systolic dysfunction based on contractile reserve and on the global longitudinal strain at rest and at low workload exercise.24 25 Furthermore, it allows assessment of inducible ischaemia and of signs of left ventricular decompensation—ejection fraction drop and development of mitral regurgitation.26 The assessment of inducible ischaemia can be also performed with dobutamine.
VSE has no role in the assessment of aortic regurgitation severity; the aortic regurgitation appears less severe with tachycardia and consequent shortening of diastole.
Mitral stenosis
The assessment of mitral stenosis severity and haemodynamic consequences based on stress echocardiography is long well established.27 VSE has changed the way mitral stenosis is perceived and managed because mitral stenosis with valve area in the range of moderate is often demonstrated to have severe stress-induced rise in mean gradient and systolic pulmonary artery pressure28; this is mainly the case for rheumatic mitral stenosis, characterised by lack of valve compliance to flow. VSE is recommended to assess asymptomatic mitral stenosis prior to major surgery or planned pregnancy to predict haemodynamic reserve or likelihood of decompensation with increase in flow.29 Current guidelines recommend VSE for management planning to inform decision-making for balloon valvotomy in asymptomatic patient, and on the other hand proceed to intervention in symptomatic patients.11 12
Supine bicycle exercise VSE allows assessment of systolic pulmonary pressure rise at low workload and assessment of mean gradient rise at low workload and peak.30 Dobutamine VSE allows assessment of mean gradient rise.31 The threshold for severe rise in mean gradient is 15 mm Hg for exercise and 18 mm Hg for dobutamine VSE.
Mitral regurgitation
Primary mitral regurgitation
The role of supine bicycle exercise VSE in the assessment of asymptomatic severe primary mitral regurgitation is well established, and the test is recommended for surgical timing by the European Society of Cardiology (ESC)/European Association for Cardio-Thoracic Surgery (EACTS) valve disease management guidelines.11 The test is essential for an early repair strategy in degenerative mitral regurgitation, detecting symptoms, subclinical left ventricular systolic dysfunction or pathological systolic pulmonary artery pressure rise.32 33 Following a complete assessment at rest, images are acquired at low workload and at peak for systolic pulmonary artery pressure assessment and for assessment of the left ventricle. A rise in systolic pulmonary artery pressure to over 60 mm Hg is a harbinger of poor outcomes.34–37
The use of supine bicycle exercise VSE for the assessment of primary mitral regurgitation severity in symptomatic patients with moderate regurgitation at rest is underpinned by robust evidence.38–40 Primary mitral regurgitation, regardless of aetiology, can have a dynamic component, increasing on exertion and thus explaining the symptoms. The assessment of mitral regurgitation severity is mainly based on images acquired at low workload and intermediate level of exercise because mitral regurgitation quantification becomes more difficult at heart rate >115 beats per minute.
Secondary mitral regurgitation
Supine bicycle exercise VSE can be used for the assessment of secondary mitral regurgitation of ischaemic aetiology or due to non-ischaemic dilated cardiomyopathy. VSE can demonstrate an increase in secondary mitral regurgitation severity during exertion in patients with exertional symptoms not explained by the severity of mitral regurgitation and left ventricular systolic dysfunction at rest.41 However, often the severity of secondary mitral regurgitation decreases with exertion in patients with non-ischaemic dilated cardiomyopathy because of contractile recruitment; the decrease in severity confirms the secondary nature of the regurgitation and a good prognosis because of the existence of contractile reserve. In patients with coronary disease, an increase in mitral regurgitation severity during VSE suggests need for mitral valve repair at the time of surgical revascularisation.
Conclusion
The use of VSE is a fruitful complementary technique to assess patients with valve disease and adds important missing pieces to the puzzle. In our view, it enhances diagnostic accuracy and enables a better treatment planning. Exercise stress echocardiography is safe and should be encouraged especially in heart valve clinics to understand the complex response of the left ventricle and valve haemodynamics during exercise in asymptomatic patients. Dobutamine stress echocardiography has an undeniable role in severity assessment and risk stratification of patients with low-flow, low-gradient aortic stenosis and reduced left ventricular ejection fraction. It proved useful in the severity assessment of symptomatic patients with low-gradient aortic stenosis and preserved ejection fraction. Larger scale studies on the role of VSE in each type of severe valve disease are needed.
References
Footnotes
Contributors PL and MG wrote the first draft. TS, YYG, RD, CO, SM provided critical review and the figures (practical cases).
Competing interests CO is Senior Research Associate at the belgian Funds for Scientific Research (FRS-FNRS).
Provenance and peer review Commissioned; externally peer reviewed.