Article Text

Abstract
Objectives Postoperative atrial fibrillation (AF) following coronary artery bypass graft surgery (CABG) is significantly associated with reduced survival, but poor characterisation and inconsistent definitions present barriers to developing effective prophylaxis and management. We sought to address this knowledge gap.
Methods From 2002 to 2010, 11 239 consecutive patients without AF underwent isolated CABG at five sites. Clinical data collected for the Society of Thoracic Surgeons (STS) Database were augmented with details on AF detected via continuous in-hospital ECG/telemetry monitoring to assess new-onset post-CABG AF (adjusted for STS risk of mortality); time to first AF; durations of first and longest AF episodes; total in-hospital time in AF; number of in-hospital AF episodes; operative mortality; stroke; discharge in AF; and length of stay (LOS).
Results Unadjusted incidence of new-onset post-CABG AF was 29.5%. Risk-adjusted incidence was 33.1% and varied little over time (P=0.139). Among 3312 patients with post-CABG AF, adjusted median time to first AF was 52 (IQR: 48–55) hours; mean (SD) duration of first and longest events were 7.2 (5.3,9.1) and 13.1 (10.4,15.9) hours, respectively, and adjusted median total time in AF was 22 (IQR: 18–26) hours. Adjusted rates of operative mortality, stroke and discharge in AF did not vary significantly over time (P=0.156, P=0.965 and P=0.347, respectively). LOS varied (P=0.035), but in no discernible pattern.
Conclusions Each year, ~800 000 people undergo CABG worldwide; >264 000 will develop post-CABG AF. Onset is typically 2–3 days post-CABG and episodes last, on average, several hours. Effective prophylaxis and management is urgently needed to reduce associated risks of adverse outcomes.
- coronary artery disease surgery
- atrial fibrillation
- epidemiology
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is a common complication of cardiac surgery associated with poorer short-term and long-term outcomes, including mortality and stroke.1–5 No large study (>10 000 patients), incorporating the necessary clinical details to comprehensively describe the incidence and characteristics (timing, frequency and duration) of these AF episodes following coronary artery bypass graft surgery (CABG), has previously been conducted. Such work is a necessary precursor to research that will elucidate the associations between the characteristics of post-CABG AF and adverse outcomes, which will, in turn, guide clinical practice to effectively manage these patients’ risks.
Reported incidence of postoperative AF varies widely between studies (from 10% to 65%),6 7 due partly to inconsistencies in the cardiac surgeries included, the inclusion/exclusion of patients with a history of AF, and the definitions and means of detecting AF used.8–10 The data available regarding the characteristics of postoperative AF— timing of onset, duration, and frequency of episodes—are very limited, and the studies that have reported such characteristics have been small (ranging from <100 patients to ~1500 patients).11–13 Larger studies14 15 have relied on national or regional databases that do not contain the detailed clinical data necessary to address these aspects of post-CABG AF.
A further gap in the current evidence base exists with respect to how the incidence and characteristics of post-CABG AF might be changing over time, both as the demographics of the CABG population have changed with increased use of percutaneous coronary intervention,16–18 and as emphasis has been placed on use of strategies such as preoperative β-blocker administration to prevent development of post-CABG AF.19 20
The aim of the present large multicentre study is to provide a comprehensive and rigorous picture of new-onset post-CABG AF as experienced by the population of patients undergoing isolated CABG within the context of the contemporary prophylaxis and/or management, not to assess the impact of such clinical measures on its incidence, characteristics, or association with adverse outcomes.
Methods
Study setting and design
This is a large multicentre observational study which included 11 239 consecutive patients without a history of AF who underwent isolated CABG between 1 January 2002 and 31 December 2010 at Baylor University Medical Center (Dallas, Texas), The Heart Hospital Baylor Plano (Plano, Texas), Emory University (Atlanta, Georgia), University of Virginia (Charlottesville, Virginia), or Washington University (St. Louis, Missouri). Patients were excluded if they had a history of AF, preoperative endocarditis and/or a ventricular assist device.
The study was approved by the institutional review board for each centre; all waived the requirement for informed consent from included patients.
Study data
Data regarding patient and operative characteristics (listed in tables 1 and 2) routinely collected for the Society of Thoracic Surgeons (STS) Database were augmented with detailed data regarding new-onset post-CABG AF events detected via continuous in-hospital ECG/telemetry monitoring and documented by a physician in the medical record.
Patient characteristics by development of new-onset atrial fibrillation (AF)
Study population characteristics by year
Outcomes of interest
Primary outcome measure
The primary outcome measure was the adjusted incidence of new-onset post-CABG AF, defined as any episode detected via continuous in-hospital ECG/telemetry monitoring and documented by a physician in the chart, regardless of duration or need for treatment.
Secondary outcomes
Secondary outcomes included time (in hours) from end of CABG surgery to first AF episode; duration (in hours) of the first AF episode; duration (in hours) of the longest AF episode; total time (in hours) spent in AF during hospitalisation; and total number of post-CABG AF episodes experienced during hospitalisation. Operative deaths (as defined by the STS21: (1) death during CABG or (2) any in-hospital death during a continuous post-CABG stay or (3) any death within 30 days of post-CABG discharge), stroke, discharge in unresolved AF, and length of stay (LOS) were also assessed.
Statistical analysis
Patient characteristics were assessed as percentages for categorical variables and means (±SD) or medians (IQR) for continuous variables, overall and by year. We compared these characteristics between those who developed AF and those who did not using Χ2 tests for categorical variables and Wilcoxon rank-sum tests for continuous variables. Unadjusted incidence of new-onset post-CABG AF and the other outcomes were calculated overall and by year.
Generalised estimating equations models, adjusted for STS risk of mortality21 and time of operation (incremental month starting from January 2004 (month 24) to December 2010 (month 108)), were used to estimate risk-adjusted rates for each outcome, accounting for patient and site variability.22 Appropriate link functions were used depending on the study outcomes and their distributions. Adjusted rates were not estimated for years 2002–2004 as the STS risk of mortality had not yet been developed. To avoid assuming a linear association among the covariates and the outcomes of interest and to avoid the bias inherent with categorisation, restricted cubic spline functions23 were used to model all continuous covariates, applying 5 knots for the STS risk of mortality score and 7 knots for time of operation. The covariates used in the models had no missing values.
Model estimates were used to compute (together with associated P values): the adjusted incidence, timing, duration and number of episodes of new-onset post-CABG AF; operative death; stroke and discharge in unresolved AF. Plots depicting adjusted incidence of new-onset post-CABG AF, operative mortality, stroke, discharge in unresolved AF, and (LOS) over time were produced. A sensitivity analysis that excluded Emory and Washington was conducted for each AF model since these centres did not contribute patients in the initial years of the study.
All analyses were performed using SAS 9.4 (SAS Institute, Cary, North Carolina, USA).
Patient involvement
This was an observational study that sought to describe the incidence and characteristics of a common complication of CABG. No patients were involved in setting the research question or selecting the outcome measures, nor were they involved in the design and implementation of the study, and there are no plans to involve patients in dissemination.
Results
The overall unadjusted incidence of post-CABG AF was 29.5% (3312/11 239). Table 1 shows the clinical and demographic characteristics of the study population, according to whether or not they developed AF. Of note, substantial differences in the unadjusted post-CABG AF incidence were observed between the participating sites. Table 2 shows the patient and surgical characteristics by year.
Table 3 shows the patient outcomes by year. While unadjusted incidence of post-CABG AF decreased significantly from 35.0% in 2002 to 26.2% in 2010 (P=0.006), no similar decrease in the risk-adjusted incidence was observed (P=0.139; see figure 1). The risk-adjusted mean number of AF episodes per patient did differ significantly between years (P=0.005), increasing from 2004 to 2008, but decreasing again in 2009 and 2010.
Summary of outcomes by year

Adjusted probability of new-onset post-coronary artery bypass graft surgery (CABG) over time. Society of Thoracic Surgeons risk-adjusted time trend and corresponding P value showing the probability of new-onset post-CABG atrial fibrillation (AF) over the study period. The thick black line represents the point estimate, with the shaded grey area representing the 95% CI.
Among the 3312 patients who experienced at least one episode of post-CABG AF, the overall risk-adjusted median (IQR) time to first AF event was 52 (48,55) hours; this decreased significantly from 59 (56,63) hours in 2004 to 50 (45,55) hours in 2010 (P=0.007). Risk-adjusted duration of first AF event, longest AF event, and total time in AF all peaked in 2006 and reached their lowest points in 2010, but the difference over time was only significant for duration of the longest AF event (P values of 0.109, 0.035 and 0.320, respectively).
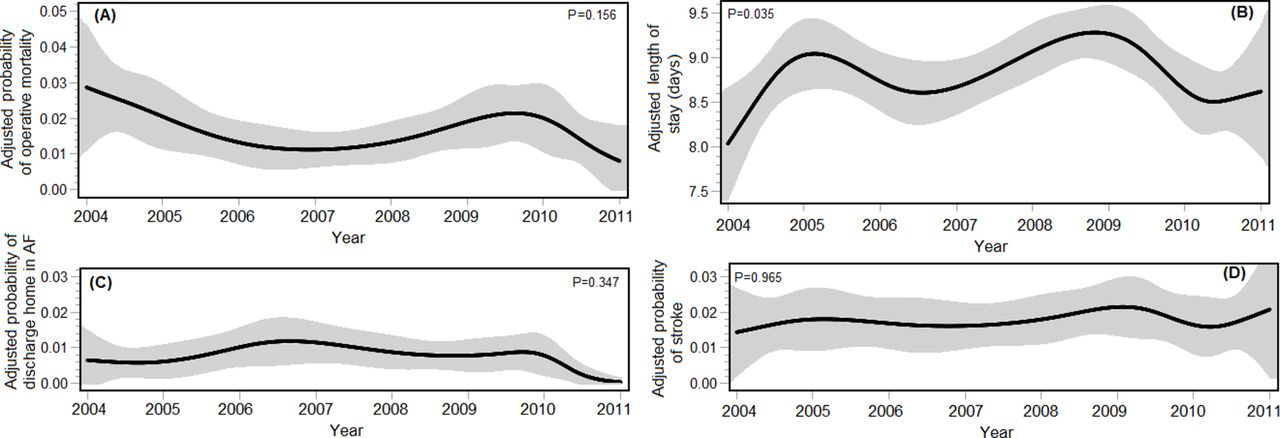
Risk-adjusted operative mortality, stroke and discharge with AF did not differ significantly over the study period (P=0.156, P=0.965 and P=0.347, respectively; see figure 2), while LOS varied marginally over time (P=0.035), but with no discernible pattern (see figure 2). In sensitivity analyses excluding Emory and Washington sites, trends were very similar to the main analysis.
{kind=link}
{kind=link}
Adjusted probability of operative mortality, stroke, being discharged in unresolved atrial fibrillation (AF), and adjusted length of stay (LOS) over time. Panels show the Society of Thoracic Surgeons risk-adjusted time trends and corresponding P values showing adverse post-coronary artery bypass graft surgery outcomes over the study period: (A)probability of operative mortality; (B) LOS; (C) probability of discharge home in unresolved AF and (D) probability of stroke. The thick black lines represent the point estimate, with the shaded grey areas representing the 95% CIs.
Discussion
Statement of principal findings
Our results provide a detailed characterisation of new-onset AF following isolated CABG (examining frequency, duration and timing, as well as incidence) from a large multicentre study that both looked specifically at new-onset AF following isolated CABG (to avoid distortion from possible significant confounders related to concomitant surgery or a history of AF) and included all documented post-CABG AF events detected via continuous in-hospital ECG/telemetry monitoring, regardless of duration or need for treatment. After adjustment for patient characteristics, the incidence of post-CABG AF remained relatively constant in this large, geographically diverse, study cohort from 2004 to 2010, and occurred at an overall rate of 33.1%. Among patients who developed post-CABG AF, we found that the first episode typically occurred between the second and the third day after CABG, and lasted 7.2 hours. The cumulative median time these patients spent in AF before discharge was 22 hours, with the longest individual AF event lasting, on average, approximately 13 hours.
Comparison with the literature
The 29.5% unadjusted incidence and 33.1% risk-adjusted incidence of postoperative AF we observed are consistent with the 10–40% range frequently cited for CABG,10 24 25 but provide convincing evidence that true incidence is towards the high end of this range. The observed risk-adjusted median time to first event of 52 hours following surgery is likewise consistent with previous observations that post-CABG AF onset tends to peak on days 2–3 post surgery.12 26 In contrast, the risk-adjusted mean/median duration of the first (7.2 hours) and longest AF events (13.1 hours), and the total time spent in AF (22 hours) among patients who had at least one episode of post-CABG AF appear short compared with the findings from a small study conducted in 299 CABG patients (reporting unadjusted average duration for short-lived AF at 4.3±3.0 hours and for recurrent/prolonged at 34.4±58.3 hours)27 and long compared with those from another small prospective study in 81 elective CABG patients (reporting a median duration of 2.25 min).13 However, these studies applied different inclusion criteria and definitions of AF13 27 from ours, making it unsurprising that results should differ.
The patterns observed over time in our study cohort with respect to comorbidities, age, body habitus, ejection fraction, and use of elective CABG are similar to those reported for isolated CABG patients from 2000 to 2009 in the national STS Adult Cardiac Surgery Database,28 indicating that our results are likely generalisable to US CABG patients. We also saw similar patterns of decreasing unadjusted operative mortality and stroke.28 Our findings regarding the incidence of new-onset post-CABG AF are less consistent, with the national cohort showing lower incidences, as well as small but statistically significant increases in both unadjusted and adjusted incidences,28 in contrast to the decreasing or stable rates we observed. At least some of the differences are likely attributable to the different definitions of AF used: the STS Database applies the definition of ‘atrial fibrillation/flutter requiring treatment',29 which we have previously shown to miss ~20% of patients who develop new-onset post-CABG AF.30 Their findings of statistical significance despite small actual changes in either the unadjusted or the risk-adjusted incidence may be explained by the very large study population (~1.5 million patients)—dwarfing even the 11 239 for which we collected data.
Meaning of the study: possible explanations and implications for clinicians and policymakers
The detailed data presented here regarding frequency, timing, and duration of all episodes of new-onset AF following isolated CABG provide an important substrate for examining how this common complication relates to poorer short-term and long-term outcomes. Previous studies have provided some evidence that adverse outcomes may only be more likely in patients with recurrent postoperative AF,31 and that these patients have longer hospital stays and experienced greater infectious, renal ,and neurological complications than those with a single episode.32 However, the small size of most previous studies, combined with the inconsistency in the definitions of AF used, and the frequent inclusion of patients with a history of AF and/or undergoing concomitant or other cardiac surgeries have prevented conclusive results from being drawn. The database established for this study will provide the necessary cohort size and inclusive definition of AF to answer these and many other questions. In the meantime, the current results provide useful details regarding the in-hospital course that patients who develop post-CABG AF can be expected to follow, enabling clinicians to make better informed decisions about management. For example, the evidence that the risk-adjusted onset and the duration of the first AF episode are 53 hours post-surgery and >7 hours, respectively, indicate both the opportunity and the value of starting pharmacological prophylaxis immediately post-surgery for any high-risk patients in whom this was not initiated prior to surgery.
Strengths and weaknesses of the study
This was a large multicentre observational study conducted at high-volume academic and/or specialty cardiac centres. As such, the results may not be generalisable to all settings in which CABG is performed—that is, low-volume programmes. However, the similarities in the patterns of patients’ characteristics and the use of elective CABG between our study cohort and the isolated CABG patients in the national STS Adult Cardiac Surgery Database28 provide reassurance that our cohort was representative of US patients undergoing this surgery. Generalisability to other countries, where demographics and/or surgical practices may differ, is, of course, more limited. We also do not, unfortunately, have information regarding the use of CABG-related protocols (eg, institutional policies regarding preoperative prophylactics) to determine the generalisability of the participating sites to other settings in this sense. Such information would also enable investigation of the causes underlying the substantial differences in unadjusted post-CABG AF incidence observed between the participating sites.
Other critical strengths include our study’s size (>11 000 patients); the inclusion of only isolated CABG patients and exclusion of patients with a history of AF; and the collection of detailed clinical data, which enabled comprehensive risk adjustment for patient clinical characteristics, assessment of the characteristics of AF episodes and the definition of AF as any episode detected via continuous in-hospital ECG/telemetry monitoring and documented by a physician in the chart (thus avoiding the exclusion of short, transient events). Basing the determination of AF on treating physician documentation made data collection for our very large cohort feasible; requiring independent assessment by study-team cardiologists of whether AF occurred would have severely limited our cohort size.
Unanswered questions and future research
The most important unanswered questions that future research needs to address are the relationships between the characteristics of post-CABG AF and survival. Such studies will enable a rigorous assessment of risk profiles among patients who develop post-CABG AF, enabling the development and implementation of tailored management plans. Future research also needs to include assessment of the impact of prophylaxis and management strategies on both the incidence and the characteristics of post-CABG AF, and how this, in turn, affects long-term outcomes. For example, while it has been shown that patients who develop secondary AF (ie, following events such as surgery, infection, acute myocardial infarction, thyrotoxicosis, acute alcohol consumption, acute pericardial disease, pulmonary embolism or other acute pulmonary disease) have similar long-term risks for stroke and mortality as patients who develop primary AF,33 the question remains open as to whether post-discharge management strategies such as arrhythmia surveillance or adherence to general AF management principles (including anticoagulation) improves outcomes for these patients. Given that >264 000 of the estimated 800 000 people worldwide undergoing CABG each year34 will develop post-CABG AF (based on the 33.1% incidence we observed), such information is urgently needed to develop effective prophylactic and management strategies.
Key messages
What is already known on this subject?
Studies examining atrial fibrillation (AF) following coronary artery bypass graft surgery (CABG) vary widely in the definition of AF used and the inclusion of patients undergoing concomitant surgeries and/or with a history of AF; as a result, there is substantial uncertainty regarding the actual risk associated with CABG.
Comprehensive data on the characteristics of post-CABG AF— timing, frequency and duration— are lacking.
What might this study add?
This multicentre study, encompassing >11 000 isolated CABG patients without a history of AF and describing any physician-documented episode of AF detected via continuous in-hospital ECG/telemetry monitoring, found an overall risk-adjusted incidence of 33.1%.
On average, the first AF episode occurred 52 hours post-CABG, lasting 7.2 hours; longest AF episode and total time spent in AF averaged at 13.1 and 22 hours, respectively.
The detailed data on post-CABG AF characteristics will provide the substrate for investigating their associations with survival, enabling assessment of risk profiles among post-CABG AF patients and development of tailored post-discharge management plans.
How might this impact on clinical practice?
These results provide useful details regarding the in-hospital course of patients who develop post-CABG AF, enabling better informed decisions about management.
References
Footnotes
Contributors GF (guarantor): conception and design of the study, data acquisition, analysis and interpretation, drafting and critically revising it for important intellectual content, approval of the version to be published and agreement to be accountable for all aspects of the work. RJD, GA, VHT: conception and design of the study, data acquisition and interpretation, revising the draft critically for important intellectual content, approval of the version to be published and agreement to be accountable for all aspects of the work contributed. BDP: data analysis, drafting the manuscript, approval of the version to be published and agreement to be accountable for all aspects of the work contributed. TKP: data acquisition and interpretation, revising the draft critically for important intellectual content, approval of the version to be published and agreement to be accountable for all aspects of the work contributed. HN: data interpretation, revising the draft critically for important intellectual content, approval of the version to be published and agreement to be accountable for all aspects of the work contributed. DMS: data acquisition, revising the draft critically for important intellectual content, approval of the version to be published and agreement to be accountable for all aspects of the work contributed. BdG: drafting the manuscript, data interpretation, approval of the version to be published and agreement to be accountable for all aspects of the work contributed. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. GF affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Funding This work was funded by National Institutes of Health/National Heart Lung Blood Institute (R01HL103683) and in part by the Bradley Family Endowment to the Baylor Health Care System Foundation and The Baylor Health Care System Cardiovascular Research Committee (Dallas, Texas).
Competing interests None declared.
Ethics approval Baylor Research Institute Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Study data contain individual identifiers; interested researchers will need to obtain waivers of informed consent and of authorisations for use and disclosure of this identifiable information from the institutional review boards at the participating sites before data can be shared for secondary research purposes.