Article Text

Abstract
Objective This study assessed adult survival and morbidity patterns in patients who underwent atrial correction according to Mustard or Senning for transposition of the great arteries (TGA).
Methods In 76 adult patients with TGA (59% male) after atrial correction, long-term survival and morbidity were investigated in three periods: early (<15 years postoperatively), midterm (15–30 years postoperatively) and late (>30 years postoperatively).
Results The Mustard technique was performed in 41 (54%) patients, and the Senning technique was performed in 35 (46%) patients aged 3.1 (IQR: 2.1–3.8) and 1.0 (IQR: 0.6–3.1; p<0.01) years, respectively. Adult survival was 82% at 39.7 (IQR: 35.9–42.4) years postoperatively and exceeded 50 years in four patients. Supraventricular tachycardia (SVT) occurred in 51% of patients. The incidences of ventricular arrhythmia (0%, 8% and 13%; p<0.01), heart failure (0%, 5% and 19%; p<0.01) and surgical reinterventions (0%, 5% and 11%; p=0.01) increased from early to late follow-up. At last follow-up, RV function was depressed in 31 (46%) patients, and New York Heart Association functional class was ≥2 in 34 (48%) patients. Bradyarrhythmia, SVT and ventricular arrhythmia were associated with depressed RV function (OR: 4.47, 95% CI 1.50 to 13.28, p<0.01; OR: 3.74, 95% CI 1.26 to 11.14, p=0.02; OR: 14.40, 95% CI 2.80 to 74.07, p<0.01, respectively) and worse functional capacity (OR: 2.10, 95% CI 0.75 to 5.82, p=0.16; OR: 2.87, 95% CI 1.06 to 7.81, p=0.04; OR: 8.47, 95% CI 1.70 to 42.10, p<0.01, respectively).
Conclusions In adult patients with TGA, survival was 82% at 39.7 (IQR: 35.9–42.4) years after atrial correction. Morbidity was high and included SVT as most frequent adverse event. Ventricular arrhythmias, heart failure and surgical reinterventions were common during late follow-up. Adverse events were associated with depressed right ventricle function and reduced functional class.
- transposition of the great arteries
- complex congenital heart disease
Statistics from Altmetric.com
Introduction
In patients born with transposition of the great arteries (TGA), the introduction of the surgical atrial correction by Senning and Mustard has greatly improved survival.1 2 Atrial correction results in redirection of deoxygenated blood to the morphological left ventricle (LV) supporting the pulmonary circulation. Oxygenated blood is redirected to the morphological right ventricle (RV), which supports the systemic circulation and needs to overcome systemic pressure. Whereas atrial correction provides good short-term outcome, long-standing RV pressure overload increases the risk of long-term cardiac morbidity and mortality.3 Moreover, the extensive surgery within the atria increases the risk of atrial arrhythmias.4 Although the surgical technique has nowadays been replaced by the arterial switch technique, survivors of atrial correction still form a relevant part of the grown-up congenital heart disease (GUCH) population.3 Whereas some patients are in good functional class, long-term adverse events are frequent and include high prevalences of heart failure, arrhythmia and reinterventions.3–7 The present study aimed, first, to assess long-term outcome in association with clinical and surgical characteristics in our adult TGA population after atrial correction. Second, temporal patterns in the incidence of adverse events were investigated.
Methods
Study population
The study population comprised TGA patients with dextrotransposition who underwent atrial correction in the Leiden University Medical Centre (the Netherlands) and survived into adulthood. The Mustard technique was performed between 1965 and 1977, and the Senning technique was performed between 1962 and 1987. The original population was extensively described in a previous paper from our centre from 1994.8 All data were retrieved from hospital information systems. Complex TGA was defined as TGA plus a ventricular septum defect requiring closure or with pulmonary stenosis. All-cause mortality was registered through the national death registry. Cause of death was investigated through case record review and the Dutch registry of patients with congenital heart disease (CONCOR) registry.9 All postoperative cardiac adverse events were registered, including those occurring during childhood and categorised as bradyarrhythmia, supraventricular tachycardia (SVT), ventricular arrhythmia, heart failure (during an acute admission or at the outpatient clinic) and need for surgical reinterventions.10 11 Functional class at last follow-up was graded 1–4 according to the New York Heart Association (NYHA). Systemic RV function at last follow-up was visually classified as normal to mildly depressed, depressed or severely depressed using transthoracic echocardiography.10 Written consent was obtained from patients for data retrieval from other hospitals. The study was conducted in accordance with the Declaration of Helsinki.
Statistical analysis
Not-normally distributed continuous variables are expressed as median (IQR). Categorical data are presented as frequencies and percentages. Differences between patients after the Mustard and Senning technique were assessed using the Mann-Whitney U test and χ2 test, for continuous and categorical data, respectively. Kaplan-Meier curves for survival after atrial correction and freedom from adverse events were drawn. Survival curves were checked for proportionality of hazards, and a log-rank test was used to compare survival between patients who underwent the Mustard procedure after 1 year and the other groups combined. To investigate the association between patient characteristics and both mortality as well as adverse events, univariable Cox regression analysis was performed to calculate HRs and 95% CIs. Adverse events were categorised in three periods: early (<15 years postoperatively), midterm (15–30 years postoperatively) and late (>30 years postoperatively), and incidences were assessed using the χ2 test. Binary logistic regression analysis was performed to investigate the association between adverse events and functional capacity and RV function by calculating ORs and 95% CI. Variables with p value <0.15 in the univariable analysis were entered in multivariable models. P values <0.05 were considered statistically significant. Statistical analysis was performed using SPSS for Windows (V.23.0).
Results
Adult population
In total, 91 patients with TGA reached adulthood after atrial correction. Clinical outcome data could not be obtained in 15 patients. These patients could not be reached (n=2), denied consent (n=1), did not undergo cardiac follow-up beyond adulthood (n=2) or died after reaching adulthood while the last treating physician could not be retrieved (n=10). Therefore, the study population comprised 76 adults (54% male). Patient characteristics of the total population and the study population are presented in table 1. There were no relevant differences between both groups. In the study population age at atrial correction was 2.4 (IQR: 0.9–3.7) years and complex TGA was present in 25 (33%) patients. Forty-one (54%) patients underwent the Mustard, and 35 (46%) patients underwent the Senning technique. Table 1 presents patient characteristics for both procedures. The Senning procedure was performed at younger age (1.0 (IQR: 0.6–3.1) vs 3.1 (IQR: 2.1–3.8)) years, p<0.01), was less frequently preceded by open surgical atrial septectomy according to Blalock-Hanlon (23% vs 68%, p<0.01) after the introduction of the balloon septectomy by Rashkind and was more frequently performed under cardioplegia (66% vs 2%, p<0.01) as compared with the Mustard procedure. Moreover, complex TGA (43% vs 24%, p=0.09) appeared more frequent in patients who underwent the Senning procedure.
Baseline and surgical characteristics of the population
Survival
Survival was 82% at 39.7 (IQR: 35.9–42.4) years after atrial correction. In four (5%) patients, follow-up extended more than 50 years (three patients after Mustard and one patient after Senning procedure). Eleven out of 76 adult patients died. Causes of death were heart failure in five (7%) patients, sudden cardiac death in three (4%) patients, subarachnoid haemorrhage in one (1%) patient, meningioma in one (1%) patient and cause of death was unknown in one (1%) patient. From all patient and surgical characteristics, only higher age at atrial correction (HR: 1.20/year, 95% CI 1.01 to 1.43, p=0.04) was associated with all-cause mortality after correction for complex TGA (table 2). Specifically, patients who underwent the Mustard procedure after the age of 1 year had the worst survival characteristics (survival for Mustard procedure after the age of 1 year: 73% vs survival of the other groups combined: 97%, p=0.03, figure 1).
HRs for mortality in adults after atrial correction for transposition of the great arteries
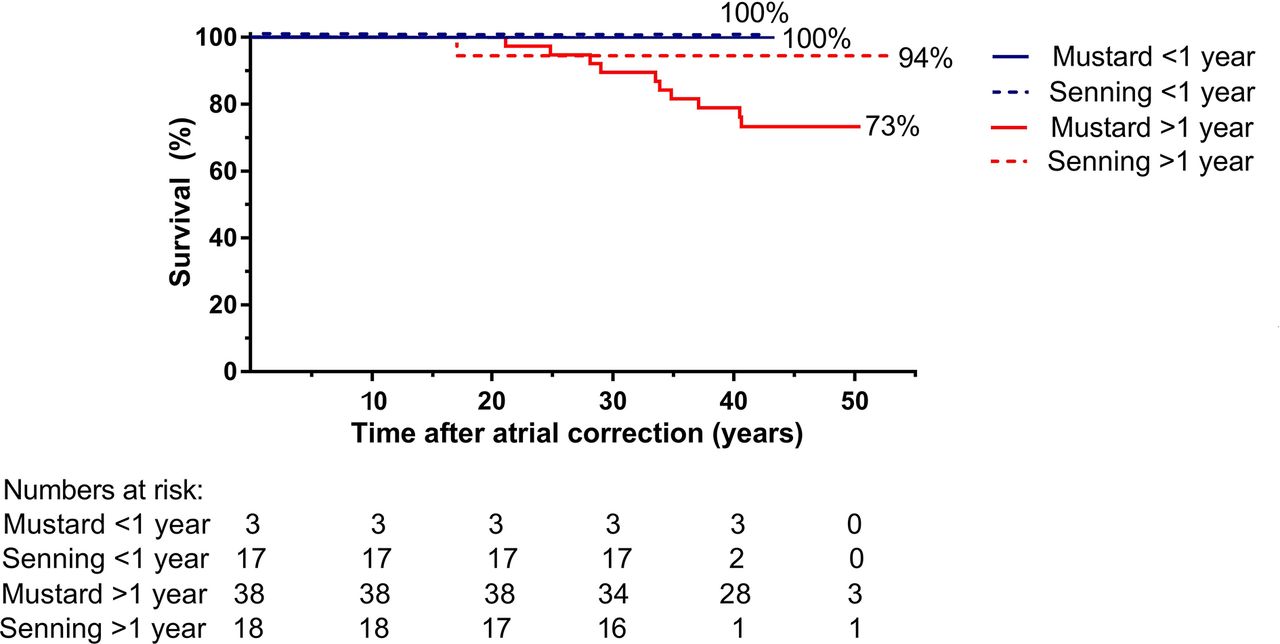
Survival curves of adult survivors of atrial correction for transposition of the great arteries.
Clinical outcome
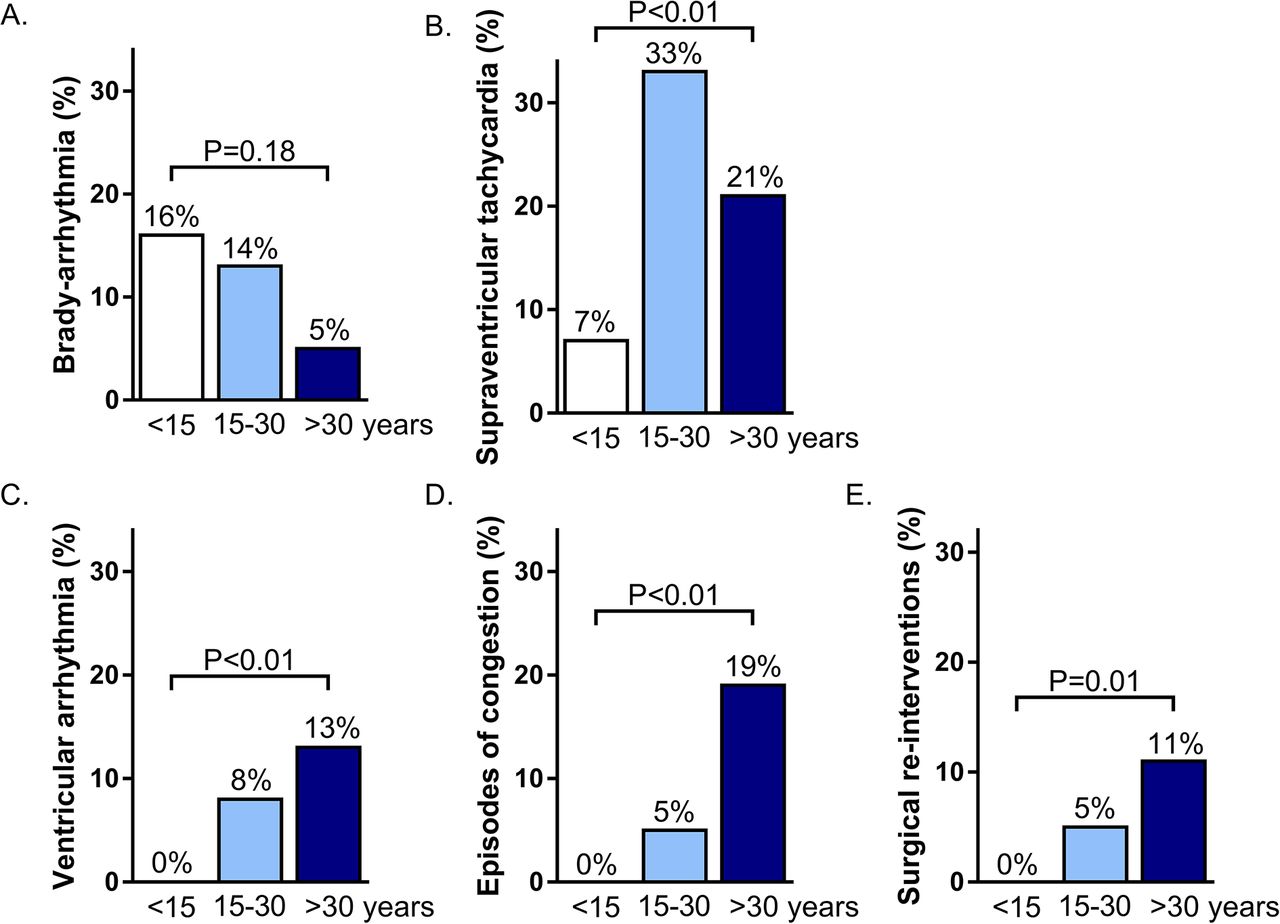
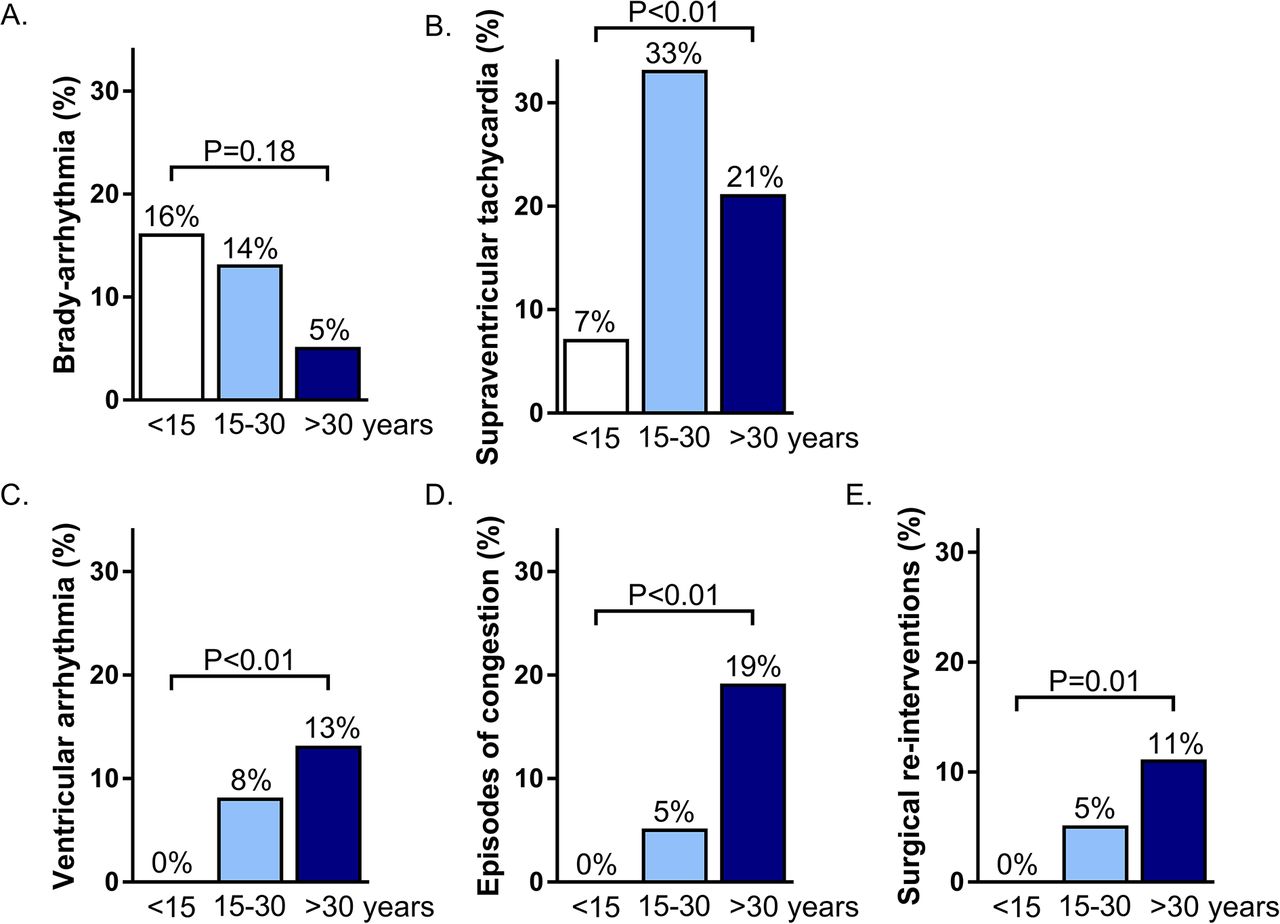
Figure 2 depicts survival curves for freedom of adverse events. Figures 2 and 3A show the highest incidence of bradyarrhythmia in the first 15 years after surgery (incidence 16%, 14% and 6% for early, midterm and late postoperatively, respectively, p=0.18). In total, 24 (32%) patients developed bradyarrhythmia after 16.6 (IQR: 6.9–25.9) years follow-up (sick sinus syndrome in 22 patients, chronotropic incompetence in 2 patients). No baseline characteristics were related to the development of bradyarrhythmia (table 3). The most frequent adverse event was SVT in 38 (51%) patients. As presented in figures 2 and 3B, SVT already occurred early after atrial correction and freedom from SVT progressively declined during follow-up. Age at atrial correction was associated with increased risk for SVT (HR: 1.18/year, 95% CI 1.05 to 1.32, p<0.01; table 3). Ventricular arrhythmia developed in 15 (20%) patients after 33.4 (IQR: 28.8–38.0) years follow-up (non-sustained ventricular tachycardia in eight patients, ventricular fibrillation in five patients, sustained ventricular tachycardia in one patient and premature ventricular contractions in bigeminy in one patient). Only age at atrial correction (HR: 1.31/year, 95% CI 1.12 to 1.53, p<0.01) was independently associated with ventricular arrhythmia, after correction for complex TGA. Treatment for arrhythmia involved device implantation in 29 (39%) patients (pacemaker in 24 patients, internal cardiac defibrillator in 11 patients and both in six patients; see table 4). An ablation procedure was performed in 12 patients for atrial tachycardia, in one patient for premature ventricular contractions in bigeminy and in one patient for ventricular tachycardia. A His bundle ablation was performed in two patients. Moreover, 17 (23%) patients developed heart failure after 33.7 (IQR: 29.8–42.9) years of follow-up. Age at atrial correction (HR: 1.21/year, 95% CI 1.00 to 1.46, p<0.05) and prior surgical septectomy (HR: 3.20, 95% CI 1.04 to 9.89, p=0.04) were independently associated with heart failure.
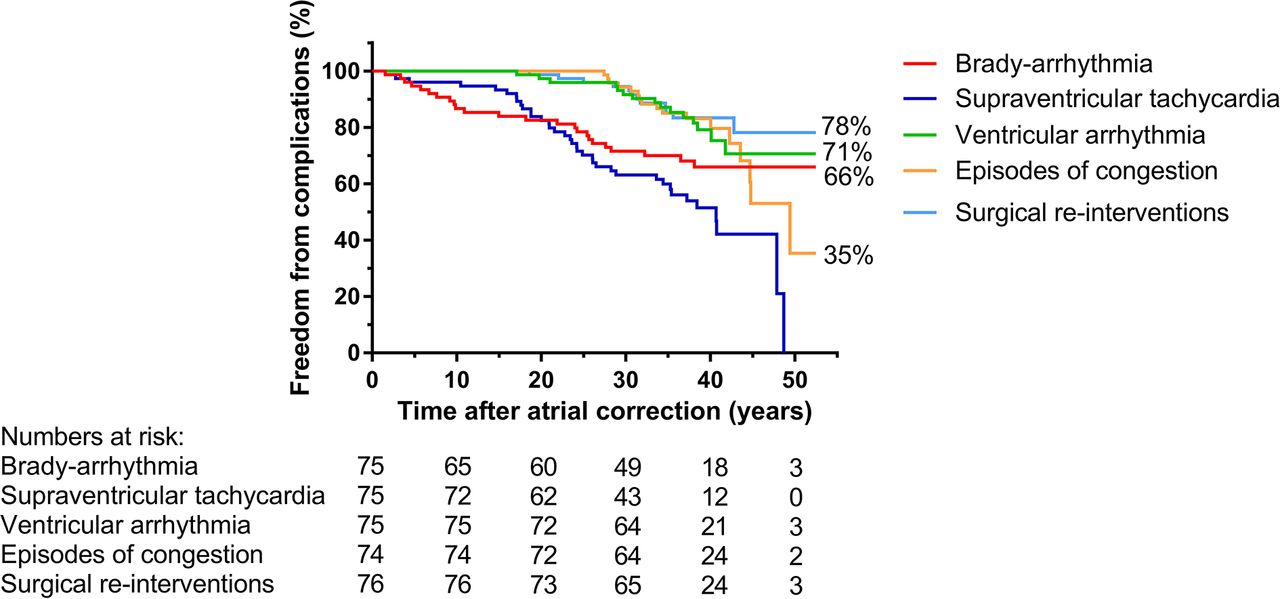
Survival curves for freedom from adverse events in adults after atrial correction for transposition of the great arteries.
{kind=link}
{kind=link}
{kind=link}
Incidence of adverse events stratified per time period of development after atrial correction.
Univariable and multivariable binary logistic regression analysis for the development of adverse events in adults after atrial correction for transposition of the great arteries
Details on device therapy
Surgical reinterventions
Surgical reinterventions included systemic atrioventricular valve repair or replacement for severe regurgitation in 11 patients (six patients after Mustard procedure, five patients after Senning procedure). Baffle revision for stenosis was performed in four patients (all after Mustard procedure) and for leakage in three patients (two patients after Mustard procedure, one patient after Senning procedure). Time between atrial correction and reintervention was 30.9 (25.8–34.7) years. Only higher age at atrial correction was associated with the need for reinterventions (HR: 1.49/year, 95% CI 1.22 to 1.83, p<0.01).
Interestingly, figures 2 and 3 show that the incidences of ventricular arrhythmia, heart failure and need for surgical re-interventions follow a comparable course after atrial correction, low incidences in the early postoperative period that increasingly rise during further follow-up.
Current clinical status
At last follow-up, 34 (48%) patients were in NYHA functional class II or higher. A history of SVT (OR: 2.87, 95% CI 1.06 to 7.81, p=0.04) and ventricular arrhythmia (OR: 8.47, 95% CI 1.70 to 42.10, p=0.01) were associated with NYHA functional class II or higher, after adjusting for follow-up duration (table 5). Systemic RV function at last-follow-up was categorised as normal to mildly depressed in 36 (54%) patients, depressed in 27 (40%) patients and severely depressed in 4 (6%) patients. A history of bradyarrhythmia (OR: 3.74, 95% CI 1.26 to 11.14, p=0.02), SVT (OR: 3.69, 95% CI 1.19 to 11.43, p=0.02) and ventricular arrhythmia (OR: 14.40, 95% CI 2.80 to 74.07, p<0.01) were all associated with depressed RV function, after adjusting for follow-up duration.
ORs for impaired functional capacity and RV function in adults after atrial correction for transposition of the great arteries
Discussion
The main findings of this study were: (1) survival was worst in patients who underwent the Mustard procedure after the age of 1 year; (2) higher age at atrial correction was associated with increased risk of SVT, ventricular arrhythmia and heart failure and the need for surgical reinterventions during follow-up; (3) SVT was the most frequent adverse event after atrial correction; (4) the type of adverse events evolved as follow-up duration after TGA increased with more frequent bradyarrhythmia early postoperatively followed by higher incidences of ventricular arrhythmia, heart failure and surgical reinterventions during further follow-up; and (5) these long-term sequelae after atrial correction were associated with worse functional capacity and depressed RV function at last follow-up.
Survival
In the current study, adult survival after atrial correction was 82% after 39.7 (IQR: 35.9–42.4) years. In previous studies, with shorter follow-up durations compared with the present study, similar survival characteristics were demonstrated: Cuypers and colleagues: survival 68%, 39 years after birth in a single-centre study of 68 patients, Moons and colleagues: survival 79.3%, 30 years postoperatively in 283 early survivors in a multicentre study and Horer and colleagues: survival 84% in 81 hospital survivors 20 years postoperatively from a single centre.3 5 6 To the best of our knowledge, the present study is the first to report survival data on patients with TGA with follow-up exceeding 50 years after atrial correction. This study therefore highlights that these patients will remain a relevant part of the GUCH population for the upcoming years, even though the surgical technique has nowadays been largely replaced by the arterial switch procedure.
Temporal patterns in adverse outcome
Patients with TGA are prone for the development of long-term sequelae after atrial correction. Higher age at atrial correction was associated with SVT, ventricular arrhythmia, heart failure and need for surgical reinterventions during long-term follow-up. Cuypers and colleagues found a similar association between age at surgery and development of heart failure in Mustard patients and hypothesised that a prolonged presence of cyanosis may have affected the ventricular myocardium negatively.3 During the era of atrial correction, the treatment strategy evolved into performing atrial correction at younger age.3 8 This is reflected in our data showing younger patients who underwent the Senning procedure, which was mostly performed in a later time period as compared with the Mustard procedure.8 12 Moreover, patients who underwent the Mustard procedure after the age of 1 year had the worst survival.
The present study showed that the type of adverse events evolved during follow-up after atrial correction. The incidence of bradyarrhythmia was highest in the first 15 years postoperative. This is in line with findings by Cuypers and colleagues who concluded that sinus node disease appeared primarily a problem in the earlier decades after atrial correction (prevalence 32% in the 1990 cohort aged 14.1 years, 60% in the 2001 cohort aged 25.8 years and 51% in the 2012 cohort aged 35.8 years).3 The incidence of SVT in our study steadily increased during follow-up, and all patients with follow-up exceeding 50 years had experienced SVT. Other studies showed a high burden of SVT in this population as well.3–5 In a study by Moons and colleagues the development of atrial flutter increased with longer postoperative follow-up.5 The development of SVT can be partly related to surgical atrial scar tissue, as these arrhythmia present less frequently in patients with congenitally corrected TGA.4 Dos and colleagues found that atrial tachyarrhythmia were independently associated with increased mortality risk in patients with TGA after atrial switch.13 This emphasises the need for re-establishing and maintaining sinus rhythm through medical therapy and ablation procedures in this population.
The incidence of ventricular arrhythmia, heart failure and surgical reinterventions appeared to increase simultaneously and progressively during long-term follow-up. Development of these long-term sequelae after atrial correction was associated with worse functional capacity and depressed systemic RV function at last follow-up. Previous studies have described RV functional decline during long-term follow-up after atrial correction and its implications. Cuypers and colleagues found that the prevalence of normal RV function on echocardiography in a cohort of Mustard patients decreased from 69% to 2% in 22 years (<0.001).3 Impaired echocardiographic RV function was associated with increased risk of heart failure and ventricular arrhythmia in a study by Kalogeropoulos and colleagues.14 Schwerzmann and colleagues showed that impaired systemic RV ejection fraction was associated with increased risk for ventricular arrhythmia and sudden cardiac death in patients after the Mustard procedure.7
Clinical implications
This study is the first to describe follow-up in patients with TGA exceeding 50 years after atrial correction. The present survival tendency indicates that these patients will remain a relevant part of the GUCH population in the upcoming years. Patients who underwent the Mustard procedure after the age of 1 year had the worst prognosis. The incidences of heart failure, ventricular arrhythmia and surgical reinterventions increased during follow-up. Furthermore, bradyarrhythmia, SVT and ventricular arrhythmia were associated with worse functional capacity and depressed systemic RV function at last follow-up. Based on this tendency, the incidence of adverse events will presumably further increase as follow-up after atrial correction extends. It can be postulated that long-standing RV overload causes a vicious cycle of increased oxygen demand, RV ischaemia, vulnerability for ventricular arrhythmia and decreased cardiac output in these patients, comparable with the sequelae of LV heart failure in the general population.
Frequent follow-up visits are essential for timely diagnosis and treatment of adverse events and can aid in the prevention of worsening RV dysfunction and severe arrhythmia. However, treatment strategies for LV failure unfortunately do not appear as successful in systemic RV failure. Medical therapy forms the cornerstone of treatment in LV heart failure, but no convincing evidence is yet available for its use in systemic RV failure.15–17 Tricuspid valve surgery is performed, analogous to mitral valve surgery in LV heart failure, to overcome valve insufficiency and worsening of systemic ventricular dilatation, but good survival rates are only obtained in patients operated before development of systemic RV failure.11 18 First results show a potential benefit of cardiac resynchronisation therapy in patients with systemic RV failure.19 20 Ultimate treatment options consist of heart transplantation in a selected population or potentially ventricular assist device implantation.16 21
Limitations
Some limitations should be considered. First, during the era of atrial correction, advances in surgical techniques have resulted in an evolving population; the Mustard technique was initially more frequently used, while the Senning technique subsequently gained preference. The Raskind technique for balloon atrial septectomy and the use of cardioplegia were introduced, and the age at atrial correction decreased, which is reflected in the difference between patients after the Mustard and Senning procedure.3 8 11 These developments make it difficult to independently assess the individual impact of clinical and surgical characteristics on outcome. Furthermore, all patients were individually approached to retrace the hospital of follow-up. Unfortunately, in some patients who died long ago, the follow-up data could not be retrieved or where incomplete. Although these patients did not differ in terms of baseline characteristics, this may have biased our results.
In conclusion, adult survival after atrial correction for TGA was 82% and was most markedly reduced in patients who underwent the Mustard technique after the age of 1 year as compared with early-operated patients or patients who underwent the Senning technique. Long-term morbidity was high and included SVT as most frequent adverse event, while the incidences of heart failure, ventricular arrhythmia and surgical reinterventions increased during long-term follow-up. Bradyarrhythmia, SVT and ventricular arrhythmia were associated with depressed RV function and worse functional capacity at last follow-up.
Key messages
What is already known on this subject?
In patients with transposition of the great arteries (TGA), atrial correction provides good short-term outcome. However, long-standing systemic right ventricular (RV) overload increases the risk of long-term cardiac morbidity and mortality.
What might this study add?
In adult patients with TGA, survival was 82% at 39.7 (IQR: 35.9–42.4) years after atrial correction. Morbidity was high and included supraventricular tachycardia as most frequent adverse event.
The incidence of ventricular arrhythmias, heart failure and surgical reinterventions increased during late follow-up. Adverse events were associated with depressed RV function and reduced functional class.
How might this impact on clinical practice?
Regular follow-up after atrial correction is essential for timely diagnosis of adverse events and prevention of worsening RV dysfunction and severe arrhythmia.
References
Footnotes
Contributors All authors have contributed significantly to the submitted work and approved submission of the manuscript. LEC: conception and design of the research, acquisition of data, statistical analysis and interpretation of the data, drafting the manuscript, critical revision of the manuscript for important intellectual content and final approval of the manuscript. HWV, TEZ and MJS: conception and design of the research, analysis and interpretation of the data, critical revision of the manuscript for important intellectual content and final approval of the manuscript. PK, MRMJ, ERH, KZ and MGH: conception and design of the research, acquisition of data, analysis and interpretation of the data, drafting the manuscript, critical revision of the manuscript for important intellectual content and final approval of the manuscript. RWCS: conception and design of the research, acquisition of data, analysis and interpretation of the data, supervising the work, drafting the manuscript, critical revision of the manuscript for important intellectual content and final approval of the manuscript.
Funding The Department of Cardiology receives unrestricted grants from Biotronik (Berlin, Germany), Boston Scientific (Marlborough, Massachusetts) and Medtronic (Minneapolis, Minnesota).
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was approved by the LUMC ethical committee.
Provenance and peer review Not commissioned; externally peer reviewed.