Article Text

Abstract
Objective A subset of patients at the time of transcatheter mitral valve repair (TMVR) will have normal left atrial pressure (LAP) (<13 mm Hg) despite having severe mitral regurgitation (MR). The goal of this study was to determine clinical characteristics and outcomes in patients with normal LAP undergoing TMVR.
Methods A single-centre retrospective cohort of consecutive patients who underwent transcatheter edge-to-edge mitral valve clip and continuous LAP monitoring between 5/1/2014 and 5/1/2018 was analysed. One-year mortality was compared by Kaplan–Meier survival curves. Multivariable analysis was performed to identify predictors of normal LAP and 1 year mortality.
Results Of the 204 patients undergoing TMVR, 65% were men and the mean age was 81. Of these patients, 31 (15%) had normal LAP (mean LAP 10.5 mm Hg, mean V wave 16.5 mm Hg) and 173 had elevated LAP (mean LAP 19 mm Hg, mean V wave 32.5 mm Hg). The prevalence of severe MR was not different between groups, although the normal LAP group had significantly lower effective regurgitant orifice area and regurgitant volume. Other notable baseline characteristics including prior cardiac surgery, atrial fibrillation, hypertension, diabetes, congestive heart failure, body mass index, mechanism of MR and ejection fraction were similar between groups. However, there was an increased prevalence of chronic lung disease (CLD) (45.2% vs 17.3%, p<0.001) in the normal LAP group. On multivariate analysis, the only significant predictor of normal LAP was the presence of CLD (OR 4.79 (1.83–12.36), p=0.001) and 1-year mortality was significantly higher in the normal LAP group (32.3% vs 12.7%, p=0.006). After adjustment for comorbidities, normal LAP was no longer a predictor of 1-year mortality (RR 1.62 (0.64–4.06), p=0.32); however, CLD (RR 3.44 (1.37–8.67), p=0.01) remained a statistically significant predictor.
Conclusion Normal LAP at the time of TMVR is associated with a higher incidence of CLD which independently predicts increased 1-year mortality. In patients with CLD and apparently severe MR, measurement of LAP may help identify those with lower likelihood of benefit from TMVR.
- transcatheter mitral valve repair
- left atrial pressure
- mitral regurgitation
Statistics from Altmetric.com
Introduction
Transcatheter mitral valve repair (TMVR) reduces symptom burden, hospitalisations and improves quality of life for patients with severe symptomatic mitral regurgitation (MR) at high surgical risk.1–7 Continuous monitoring of left atrial pressure (LAP) during TMVR provides valuable insight into the immediate haemodynamic effects and post-procedural clinical outcomes. In the setting of severe MR, the LAP is typically elevated, and an acute intra-procedural reduction in LAP is associated with improved 6 min walk distance (6MWD) at 30 days.8 Conversely, an increase in LAP after TMVR portends an increased risk of rehospitalisation for heart failure.9
A subset of patients at the time of TMVR will have normal baseline LAP despite having severe MR.10 While it has been hypothesised that the normal LAP despite severe MR may reflect alterations in left atrial compliance, the clinical outcomes of these patients relative to patients with elevated LAP are unknown. We hypothesised that normal LAP may identify a group less likely to benefit from TMVR. The current investigation sought to determine clinical characteristics and outcomes in patients with normal LAP undergoing TMVR.
Methods
Patient population
A retrospective cohort of consecutive (18 and older) patients who underwent TMVR using the MitraClip system (Abbott, Illinois, USA) with continuous LAP monitoring via a dedicated monitoring catheter between May 1, 2014 and May 1, 2018 at Mayo Clinic (Rochester, Minnesota) was identified. Patients without direct LAP monitoring data were excluded from the analysis. All patients were evaluated using a heart team approach and counselled regarding potential risks of and alternatives to the procedure prior to providing informed consent. This retrospective study was approved by the Mayo Clinic Institutional Review Board.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
TMVR procedure and continuous LAP monitoring
Following transseptal puncture, an opening LAP measurement was recorded and served as the baseline LAP for the current investigation. As has been described previously, once transseptal access is obtained; two guidewires were advanced into the left superior pulmonary vein.11 The atrial septum was then dilated and a 4 French multipurpose catheter was advanced over one of the guidewires. The MitraClip steerable guiding catheter was then advanced over the second guidewire into the left atrium, and the multipurpose catheter pulled back into the left atrium. Following final MitraClip deployment and release a post-procedure LAP record was taken. Simultaneous aortic pressure measurements were taken with all LAP records and records were taken without breath holding manoeuvres. Mean LAP was measured during end-expiration at the mid-A wave or, in the case of atrial fibrillation, mid-C wave. The definition of normal mean LAP was pre-specified prior to any data collection or analysis as <13 mm Hg in accordance with the historical description by Braunwald et al.10 12 Elevated left atrial V wave was defined as >10 mm Hg above the mean LAP. All TMVR procedures were performed under general anaesthesia and with intra-procedural transesophageal echocardiographic guidance.
Definitions
Severity of MR was assessed by transthoracic and transesophageal echocardiography in all patients. Quantitation of MR using Proximal isovelocity surface area (PISA) and continuity methods was performed whenever technically feasible. Severe MR was defined in accordance with the published American Society of Echocardiography guideline document.13 Post-procedural MR severity was assessed via transthoracic echocardiography prior to hospital dismissal for all patients. Chronic lung disease (CLD) was defined as mild, moderate or severe according to published Society of Thoracic Surgeons (STS) criteria.
Statistical analysis
Population proportions were compared by the Pearson χ2 test. The Student’s t-test and Wilcoxon signed rank test were used to analyse means. Predictors of normal LAP were assessed by multivariate analysis with a multiple logistic regression model. Kaplan–Meier curves were generated to model 1-year survival and the curves were compared with a log rank test. Predictors of 1 year mortality were determined by a multivariable Cox proportional hazards model. All analyses were performed using JMP Pro V.14 (SAS Institute, Cary, North Carolina, USA)
Results***
Baseline characteristics
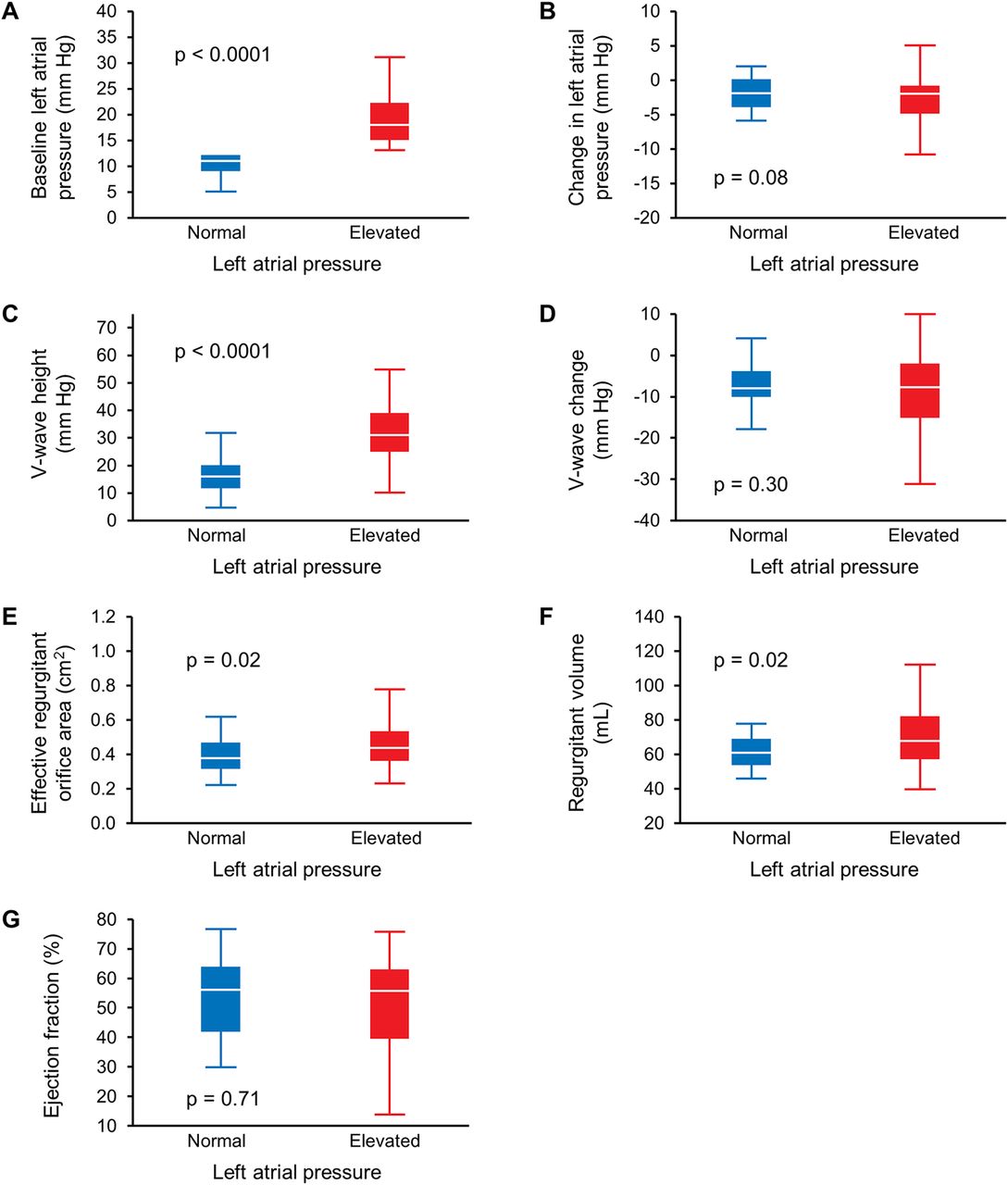
Of the 204 patients undergoing TMVR in the study, 31 (15.2%) had normal baseline LAP. Baseline characteristics according to opening LAP are displayed in table 1 with box plots of key continuous variables in figure 1. The mean age was 80% and 65.2% were men. The mean LAP was 10.5 mm Hg in the normal LAP group and 19 mm Hg in the elevated LAP group. Of the 31 patients with normal mean LAP, 6 (19.4%) had elevated V waves. At the time of baseline LAP assessment, the mean arterial pressure was slightly lower among the normal LAP group (67.6 mm Hg vs 71.8 mm Hg, p=0.02) although there was no difference in systolic blood pressure (105.8 mm Hg vs 108.9 mm Hg, p=0.24). Patients with normal LAP were more likely to have CLD (45.2% vs 17.3%, p<0.001) and less likely to have atrial fibrillation (45.2% vs 65.9%, p=0.03). After refining CLD according to severity, mild and moderate CLD tended to be more common in the normal LAP group although this did not reach statistical significance (p=0.07 for both), and severe CLD was significantly more prevalent among those with normal LAP (16.1% vs 5.8%, p=0.04).

Box plots of key continuous variables distributions of key continuous variables between groups are shown. (A) Baseline LAP, (B) absolute change in LAP, (C) baseline V-wave height, (D) absolute reduction in V-wave height, (E) effective regurgitant orifice area, (F) regurgitant volume and (G) ejection fraction. LAP, left atrial pressure.
Baseline characteristics
Quantitative measures of MR severity including effective regurgitant orifice area (0.40 cm2 vs 0.47 cm2, p=0.02) and regurgitant volume (62.3 mL vs 72.1 mL, p=0.02) were significantly lower in the normal LAP group. However, there was no difference between groups in the proportion of patients that were ultimately identified as having severe MR (71.0% vs 76.9%, p=0.48). Baseline mean New York Heart Association (NYHA) class was slightly lower in patients with normal LAP (2.9 vs 3.2, p=0.04) and 6MWD was longer (352 m vs 297 m, p=0.04). On multivariable logistic regression, the only statistically significant predictor of normal LAP was the presence of CLD (OR 4.75 (CI 1.83 to 12.36), p=0.001) (table 2).
Predictors of normal LAP by multivariable analysis
Clinical and procedural outcomes
The median follow-up duration in the overall cohort was 444 days. There was a trend towards greater reduction in LAP following TMVR in the elevated LAP group (-2.8 vs −1.9, p=0.08) (table 3). At 30 days, the median reduction in 6MWD trended towards less improvement in those with normal LAP (−3.6 m vs +25 m, p=0.11). At 1 year, there was no difference in residual MR severity (greater than moderate MR in 25.8% vs 33.0%, p=0.29), heart failure recurrence due to MR (9.7% vs 17.3%, p=0.29) or frequency of further mitral valve intervention (3.2% vs 6.9%, p=0.61). The 1-year mortality was significantly higher in the group with normal LAP (32.3% vs 12.7%, p=0.006). Among patients with normal LAP that died within 1 year, a cardiac cause of death was less likely (10.0% vs 50.0%, p=0.03). The five patients with 1-year mortality and unknown cause of death in the normal LAP group all had underlying moderate or severe CLD and two were on chronic home oxygen therapy. One patient in each group had a confirmed pulmonary cause of death.
Clinical and procedural outcomes
Predictors of mortality
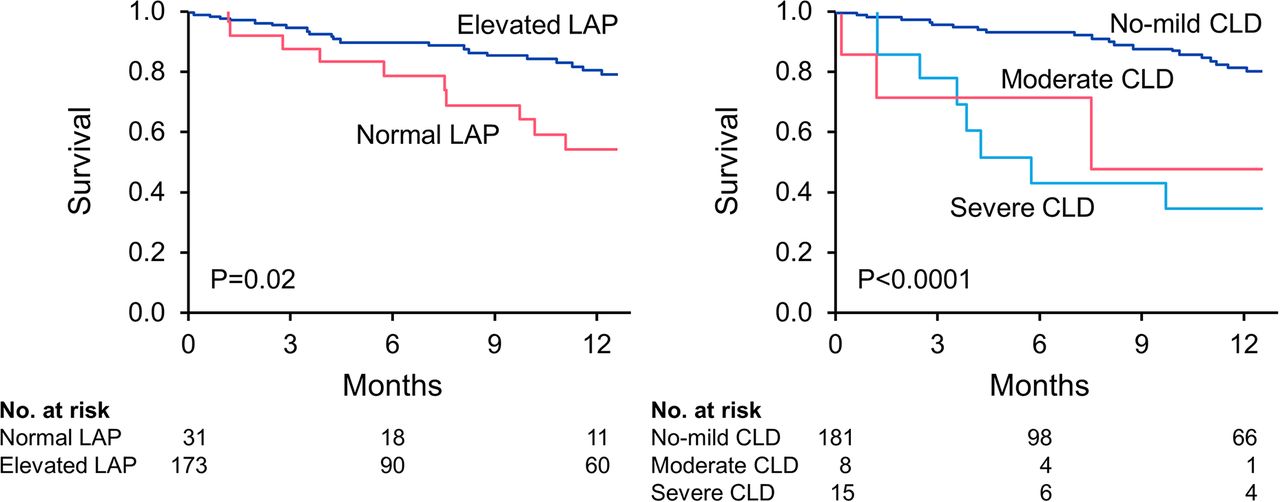
By univariate analysis, the patients with 1-year mortality were more likely to have normal LAP (HR 2.49 (1.18–5.25), p=0.03); however, on multivariable analysis this association was no longer significant (HR 1.62 (0.64–4.06), p=0.32) (table 4). The presence of CLD remained a strong predictor of mortality on multivariable analysis (HR 3.44 (1.37–8.67), p=0.01). When further refined according to severity, moderate and severe CLD remained significant predictors, while mild CLD was not. Kaplan–Meier survival curves grouped by LAP and severity of CLD both showed statistical significance (figure 2, p=0.02 and p<0.0001, respectively). Creatinine was also identified as an independent predictor of 1-year mortality on multivariable analysis (HR 1.51 (1.01–2.10), p=0.05).

{kind=link}
{kind=link}
One-year mortality according to baseline LAP and severity of CLD. Kaplan–Meier survival curves are displayed. (A) Higher mortality in patients with normal LAP (p=0.02). (B) Higher mortality in patients with moderate or severe CLD (p=<0.0001). CLD, chronic lung disease; LAP, left atrial pressure.
Predictors of 1-year mortality by multivariable analysis
Discussion
The current investigation is the first to characterise patients with normal LAP prior to TMVR. Normal LAP was present in 15% of patients with severe MR undergoing TMVR and was associated with (1) higher 1-year mortality than those with elevated LAP, (2) higher incidence of CLD and (3) a lower likelihood of cardiac cause of death. Although baseline severity of dyspnoea was less and exercise capacity greater in the normal LAP group, there was no significant difference in post-intervention NYHA class or heart failure recurrence between groups. These findings highlight the importance of LAP in the pathophysiology of severe MR, and support its use as a tool to identify patients most likely to benefit from TMVR. Furthermore, the association of normal LAP with CLD and the nearly threefold higher 1-year mortality in this group warrants careful evaluation of patients with advanced CLD to determine candidacy for TMVR.
Continuous LAP monitoring during TMVR allows for identification of the unique subset of patients with normal pre-intervention LAP.14 Historically, Braunwald et al defined this group as young patients having severe atrial enlargement and atrial fibrillation resulting from rheumatic mitral valve regurgitation. The modern cohort described in this study is quite distinct as it represents an older patient population only half of whom had atrial fibrillation, with neither of these variables identified as significant predictors of normal LAP. LAP often rises in the setting of severe MR as a result of increasing regurgitant volume according to the effective operating compliance of the atrium.15 Therefore, patients with less significant MR or higher atrial compliance will have relatively lower LAP. It is important to note that patients in this study underwent both transthoracic and transesophageal echocardiography prior to TMVR to quantitate the severity of MR. In review of MR severity based on these studies, no differences were identified between groups in left ventricular end-systolic diameter, concomitant valvular heart disease, left ventricular ejection fraction, presence of clinical heart failure or aetiology of MR. Despite lower quantitative parameters of MR in the normal LAP group (eg, regurgitant volume of 62±12 vs 72±21 mL, p=0.02), all patients in the study had quantitatively severe MR by echocardiography.
Since MR severity and therefore LAP are dynamic and directly affected by afterload, MR may still result in exertional dyspnoea even if the resting LAP is normal. However, if normal LAP is identified, further investigation into the presence and severity of CLD should be considered with careful attention to exclude artificially normal LAP due to systemic hypotension in the setting of anaesthesia. In our study, there was a small statistical difference (4.2 mm Hg) between mean arterial pressure in the normal and elevated LAP groups although this is unlikely to be clinically relevant (67.6 mm Hg vs 71.8 mm Hg, p=0.02). The veracity of the LAP measurements is further supported by the similar mean systolic blood pressures between groups (105.8 mm Hg vs 108.9 mm Hg, p=0.24) and the significant difference in V wave to systolic blood pressure ratio.
In current practice, TMVR is typically reserved for patients at increased risk for traditional open cardiovascular surgery as identified by the STS score. Since lung disease is a significant factor in increasing surgical risk, it is not surprising that our TMVR population has a relatively high prevalence of CLD (22%). In these patients, who often present with a chief complaint of dyspnoea, baseline pulmonary function tests are essential to screen for occult CLD. Despite the utility of pulmonary function testing in identifying CLD, determining the respective contributions of the pulmonary and cardiac systems to the presenting symptomatology can remain a challenge. Quantitation of MR by echocardiography may be limited by mitral annular calcification, multiple jets, very eccentric jets or concomitant aortic valve disease. Distinguishing pulmonary from cardiac dyspnoea is critically important in this population since the subset of patients with symptomatic pulmonary disease and asymptomatic grades 3–4 MR may not be expected to experience improvement in symptoms from TMVR. Nevertheless, clinical benefit can still occur in this population due to reduction in MR and its associated sequelae. The results of this study suggest that when alternative aetiologies of dyspnoea are present there is incremental diagnostic value in assessing the baseline LAP via haemodynamic catheterisation prior to making a decision regarding the appropriateness of TMVR. Furthermore, if the baseline LAP is normal, exercising the patient during haemodynamic catheterisation may unmask dynamic MR causing exertional symptoms despite normal resting LAP. This knowledge of the LAP will prove useful in the shared decision-making process when addressing post-procedural expectations and prognosis.
Limitations
All measurements of LAP were taken under general anaesthesia via direct transseptal access which limits the generalisability of the findings to pulmonary capillary wedge pressures taken under differing levels of sedation, especially given the exaggerated respirophasic effects of CLD on intra-pleural pressure. Although echocardiography demonstrated severe MR in all patients in the study, the possibility that some patients had less than severe MR cannot be definitively excluded. Additionally, the limited sample size of the normal LAP group decreases the power to detect significance in the multivariable models of LAP predictors and mortality predictors. As such, we cannot exclude that the remaining variables may be more minor predictors of mortality. Given the retrospective nature of this study performed at a tertiary referral centre, 1-year follow-up and cause of death information were incomplete. Of the 32 patients with 1-year mortality, 13 (40.6%) had unknown causes of death and the proportion of patients with unknown cause of death was similarly distributed between groups (p=0.47). Despite this limitation, it was clear that the normal LAP group was less likely to have a cardiac cause of death. Additionally, all five of the patients in the normal LAP group with unknown cause of death did have underlying moderate or severe CLD and two of these patients were on chronic home oxygen therapy. Thus, careful assessment of baseline LAP may aid in identification of patients that are less likely to benefit from TMVR due to limited life expectancy from other chronic organ failure.
Conclusion
Normal LAP at the time of TMVR is associated with a higher incidence of CLD which independently predicts increased 1-year mortality. In patients with CLD and apparently severe MR, measurement of LAP may help identify those with lower likelihood of benefit from TMVR.
Key messages
What is already known on this subject?
Continuous left atrial pressure (LAP) monitoring is a useful marker of procedural success during transcatheter mitral valve repair (TMVR). A subset of patients have normal LAP at the time of TMVR.
What might this study add?
Normal LAP prior to TMVR is associated with higher 1-year mortality and a higher incidence of chronic lung disease (CLD).
How might this impact on clinical practice?
If there is concern for alternative aetiologies of dyspnoea during work-up for TMVR, such as in patients with CLD, full characterisation of CLD with pulmonary function testing should be performed, and in selected patients right heart catheterisation may be indicated to assess the baseline LAP.
Footnotes
Contributors Study design: JS and ME. Data acquisition: JS and ME. Data analysis and interpretation: All authors. Manuscript drafting: JS and ME. Critical revision of manuscript: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The authors maintain deidentified participant data. All data relevant to the study are included in the article.