Article Text

Abstract
Aims: To evaluate whether short-axis function plays a part in determining left ventricular (LV) geometric and functional improvement after cardiac resynchronisation therapy (CRT).
Methods and results: 39 patients who received CRT were enrolled. 2D speckle tracking echocardiography was performed at baseline and three months after CRT to assess mean systolic circumferential (ϵ-circum), radial (ϵ-radial) and longitudinal (ϵ-long) strain and torsion. Responders of reverse remodelling (n = 21) had higher baseline mean ϵ-circum than non-responders (p<0.05), who also had improvement in mean ϵ-circum and mean ϵ-radial (both p<0.05) after CRT. Also, the increase in mean ϵ-circum correlated with increase in ejection fraction (r = 0.57, p<0.001) and decrease in mid-cavity width (r = −0.52, p = 0.001). A baseline mean ϵ-circum of ⩾6.5% predicted a gain in ejection fraction ⩾5%, with a sensitivity of 73% and a specificity of 71%. The baseline ϵ-long was not different between the two groups, and remained unchanged after CRT. The torsion did not improve in responders, but was worsened in non-responders (p<0.05).
Conclusions: The improvement of LV short-axis function but not long-axis function or torsion contributes to the improvement in LV global function and geometry at three-month follow up. A relatively preserved mean ϵ-circum of ⩾6.5% might be useful to predict favourable responses after CRT.
Statistics from Altmetric.com
Cardiac resynchronisation therapy (CRT) is an established therapy for patients with advanced chronic heart failure with electromechanical delay as illustrated by a prolonged QRS duration. Clinical data have suggested the beneficial role of CRT on symptoms, functional capacity, cardiac function and prognosis.1–5 Despite the favourable reverse remodelling response with reduction of left ventricular (LV) volume and gain in global ejection fraction, there were few reports on improvement of myocardial function after CRT.3 The change of global LV systolic function can be attributed to alteration in longitudinal and circumferential shortening. The long-axis function is determined by the contraction of longitudinal myocardial fibres located in subepicardial and subendocardial layers,6 7 while the short-axis function is a composite action of both longitudinal and circumferential fibres. Recently, a third component of myocardial function, LV torsion, has been described.8 Torsion occurs during the twisting and shortening of LV fibres as the longitudinal fibres are actually aligned in an oblique manner which run in opposite directions for epicardial and endocardial layers.9–11
Two-dimensional (2D) speckle tracking is a new echocardiographic technology that is based on grey scale B-mode images and hence allows angle independent assessment of myocardial function.8 10–12 This tool enables detection of myocardial deformation from continuous frame-by-frame tracking of natural acoustic markers, which is based on searching for their new location in the subsequent frame,13 and hence allows the assessment of myocardial deformation in different directions including longitudinal strain (ϵ-long), circumferential strain (ϵ-circum), radial strain (ϵ-radial) and torsion (Tor).10–12 However, whether CRT may have different impact on the long-axis, short-axis or torsion components of myocardial function, as well as their relation to changes in global LV function or LV geometry have not been previously explored. We hypothesised that when LV remodelling reached a stage of LV cavity dilatation with loss of short-axis function, heart failure could be reaching its late stage beyond its ability to reverse after CRT. This study aimed to investigate whether there was improvement in various components of myocardial function after CRT by using 2D speckle tracking technology; and whether preservation of short-axis function was an important determinant of improvement in global ejection fraction and LV reverse remodelling after CRT.
METHODS
Patients
This study consisted of 39 heart failure patients and 39 age-matched and gender-matched normal controls. Forty-one patients who fulfilled the current criteria for CRT were recruited consecutively and followed up for three months after the therapy, two of whom were excluded from the study because of the inadequate image quality for quantitative analyses. They had symptomatic heart failure with New York Heart Association (NYHA) class III or IV despite optimal pharmacological therapy, systolic dysfunction with ejection fraction <35% and electromechanical delay with QRS duration >120 ms (table 1). Biventricular devices were implanted as previously described.3 The atrioventricular interval was optimised using Ritter’s method.14 Clinical and echocardiographic assessment were performed before and three months after CRT. At the end of three months, the patients who had a reduction of LV end-systolic volume (LVESV) of ⩾15% were defined as responders to LV reverse remodelling, whereas non-responders were those with <15% decrease in LVESV. The study protocol was approved by the ethics committee and written informed consents were obtained from all the patients.
Echocardiography
LV volumes and ejection fraction were assessed by biplane Simpson’s equation. In the apical four-chamber view, the LV end-systolic and end-diastolic length and mid-cavity width were measured. The LV end-systolic and end-diastolic sphericity index was then calculated by the ratio of LV length to mid-cavity width to assess the change in geometry in relation to cardiac remodelling.15 As previously described, tissue Doppler imaging was performed to measure systolic dyssynchrony of longitudinal movement by using the dyssynchrony index—that is, standard deviation of the time to peak systolic velocity in ejection phase among the 12 LV segments (Ts-SD).16 Significant dyssynchrony was defined as Ts-SD ⩾33 ms.16–18
Two-dimensional images of basal, mid and apical short-axis views, as well as apical four-chamber, two-chamber and three-chamber views were captured using a high frame rate (50–80 frames per second). Offline analysis was performed using a customised software (EchoPac-PC SW-only, Version 6.0.0, Vingmed-GE, Horten, Norway). When a cardiac cycle with a good quality image was selected, the endocardial border was first traced manually at end-systole. A region of interest for speckle tracking was then defined automatically between the endocardium and epicardium borders to approximate the myocardium, while manual adjustment was allowed for optimal inclusion of LV wall. An 18-segmental LV model was preset in the speckle tracking modality by the software—that is, there were six evenly divided segments in each of the three long-axis or short-axis views. The data were processed and accepted automatically by the system for individual segment when the data quality was adequate and myocardial strain curves would then be generated. Out of 4212 attempted segments in this study, less than 5% were rejected and hence excluded from analysis.
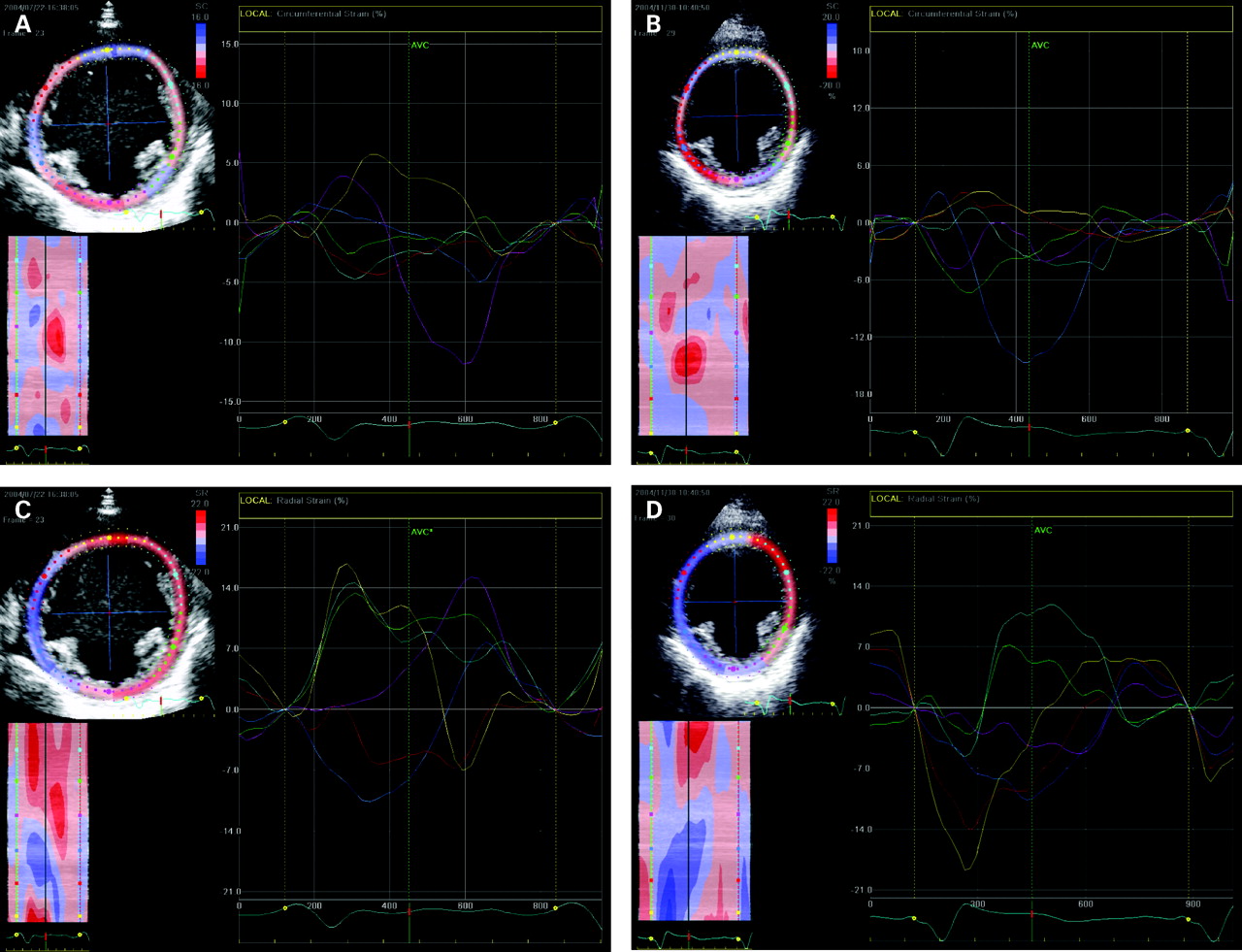
In the three short-axis planes, segmental ϵ-circum and ϵ-radial were measured, whereas rotation (Rot) was only calculated in the basal and apical segments. The amplitude of the individual component in each segment was measured during the systolic phase, which was denoted by the aortic valve closure (AVC) timing marker. This time marker was obtained by Doppler signals at the LV outflow tract before the start of strain analysis. Therefore, the peak with the largest amplitude in the systolic phase was chosen for the measurement. In case there was no peak existing before the AVC marker (for example, in occurrence of post-systolic shortening) the point where the tracing intercepted at the AVC line would be taken instead. As for rotation, when viewed from apex, normally the base rotates clockwise with a negative tracing, whereas the apex rotates counterclockwise with a positive tracing (fig 1A). The Tor is a net-difference of LV rotation between basal and apical planes stated in the unit of degree. The ϵ-circum is negative while ϵ-radial is positive, both expressed as percentage (fig 1B and 1C). If an individual tracing became opposite to the normal direction as aforementioned (for example, ϵ-circum turned positive instead of negative), it would be labelled as “paradoxical tracing”. Parameters of torsion and short-axis myocardial function were calculated as follows:

Tor: net-difference between basal and apical mean Rot
Mean ϵ-circum: mean circumferential systolic strain of the 18 LV segments
Mean ϵ-radial: mean radial systolic strain of the 18 LV segments
Torsion-(No): number of paradoxical tracing for rotation in six basal and six apical segments
ϵ-circum-(No): number of paradoxical tracing for circumferential strain in the 18 LV segments
ϵ-radial-(No): Number of paradoxical tracing for radial strain in the 18 LV segments.
Similarly, the ϵ-long which is negative normally was measured segmentally in the three apical views (fig 1D). Parameters of long-axis myocardial function were calculated as follows:
Mean ϵ-long: mean longitudinal systolic strain of the 18 LV segments
ϵ-long-(No): number of paradoxical tracing for longitudinal strain in the 18 LV segments.
Reproducibility of strain measurements using 2D speckle tracking
In 10 randomly selected subjects, the analyses were repeated a few days apart by the same observer on the same 2D loop and the same cardiac cycle. In addition, the analyses were performed by a second independent observer. The intraobserver and interobserver variabilities were 8.2% and 9.8% for Tor, 5.9% and 9.4% for mean ϵ-circum, 6.1% and 8.1% for mean ϵ-radial, as well as 2.3% and 3.1% for mean ϵ-long, respectively.
Statistical analysis
A paired or unpaired t test was performed for comparison of parametric variables where appropriate. Pearson correlation analysis was used to examine the relationship between changes in myocardial function and degree of LV reverse remodelling. In addition, receiver operating characteristics (ROC) curves were analysed for parameters of short-axis myocardial function in predicting LV reverse remodelling and improvement of ejection fraction after CRT. The χ2 test was used to compare the response rate among different groups. Parametric data were presented as mean (SD). A p value <0.05 was considered statistically significant.
RESULTS
Reduction of LV myocardial function in patients with congestive heart failure
Before device implantation, the heart failure patients showed a marked reduction of short-axis and long-axis myocardial function and torsion when compared with the control group. The mean ϵ-long (−7.6% (3.3%) vs −20.0% (2.3%)), mean ϵ-circum (−7.1% (2.6%) vs −19.5% (3.4%)), mean ϵ-radial (10.6% (6.3%) vs 43.6% (9.6%)) and torsion (6.8 (4.2) vs 16.2 (5.5) degrees) were decreased significantly to 38%, 35%, 25% and 42% of the normal values, respectively (all p<0.001). When the corresponding individual LV plane (basal, mid, apical) was compared between the two groups, the measured parameters were all significantly reduced in patients with heart failure (all p<0.001).
Changes in individual component of myocardial function after CRT
At three months after CRT, LV reverse remodelling and improvement of global systolic function were evident by the reduction of LV end-diastolic (LVEDV) and end-systolic volumes and gain in ejection fraction (all p<0.001) (table 2). Mitral regurgitation was markedly reduced (p = 0.001). For LV geometry, the reduction of mid-cavity width was greater than that of cavity length, resulting in the improvement of both end-diastolic and end-systolic sphericity indices (both p<0.05) (table 2). With respect to LV myocardial function, the mean ϵ-circum and the mean ϵ-radial were improved with decrease in ϵ-circum-(No) and ϵ-radial-(No) (all p<0.05) (table 2). Interestingly, there was a worsening of the torsion (p<0.05) with a trend of increase in torsion-(No). In contrast to short-axis function, long-axis function as illustrated by the mean ϵ-long failed to show any improvement despite a favourable change in LV global systolic function after CRT (table 2).
In exploring the relation between the improvement of short-axis strain and that of LV global function or geometry, it was found that the changes of mean ϵ-circum and mean ϵ-radial correlated significantly with reduction of LVESV, increase in LV ejection fraction and decrease in LV end-systolic mid-cavity width (table 3).
Differential changes in myocardial function between responders and non-responders of reverse remodelling
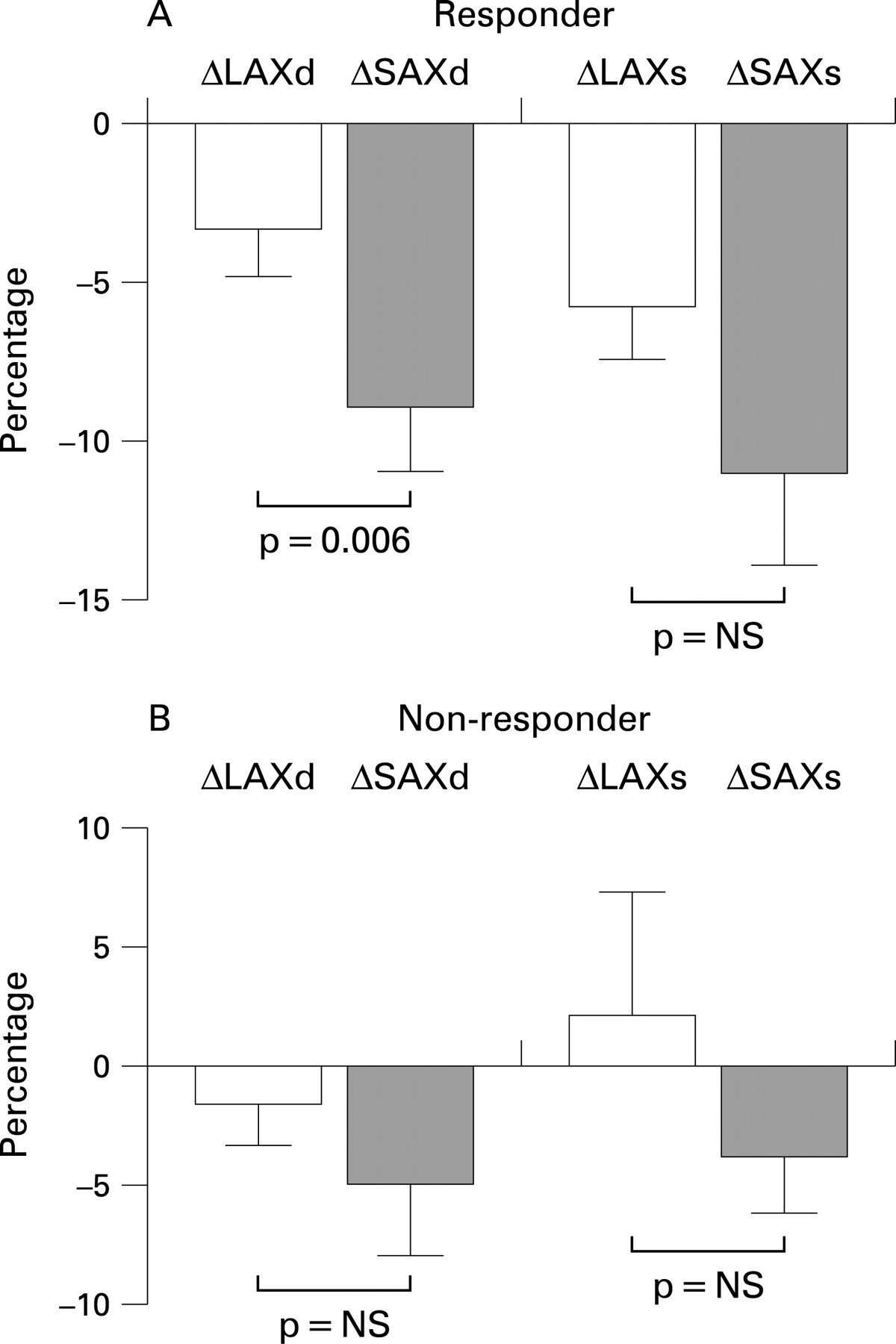
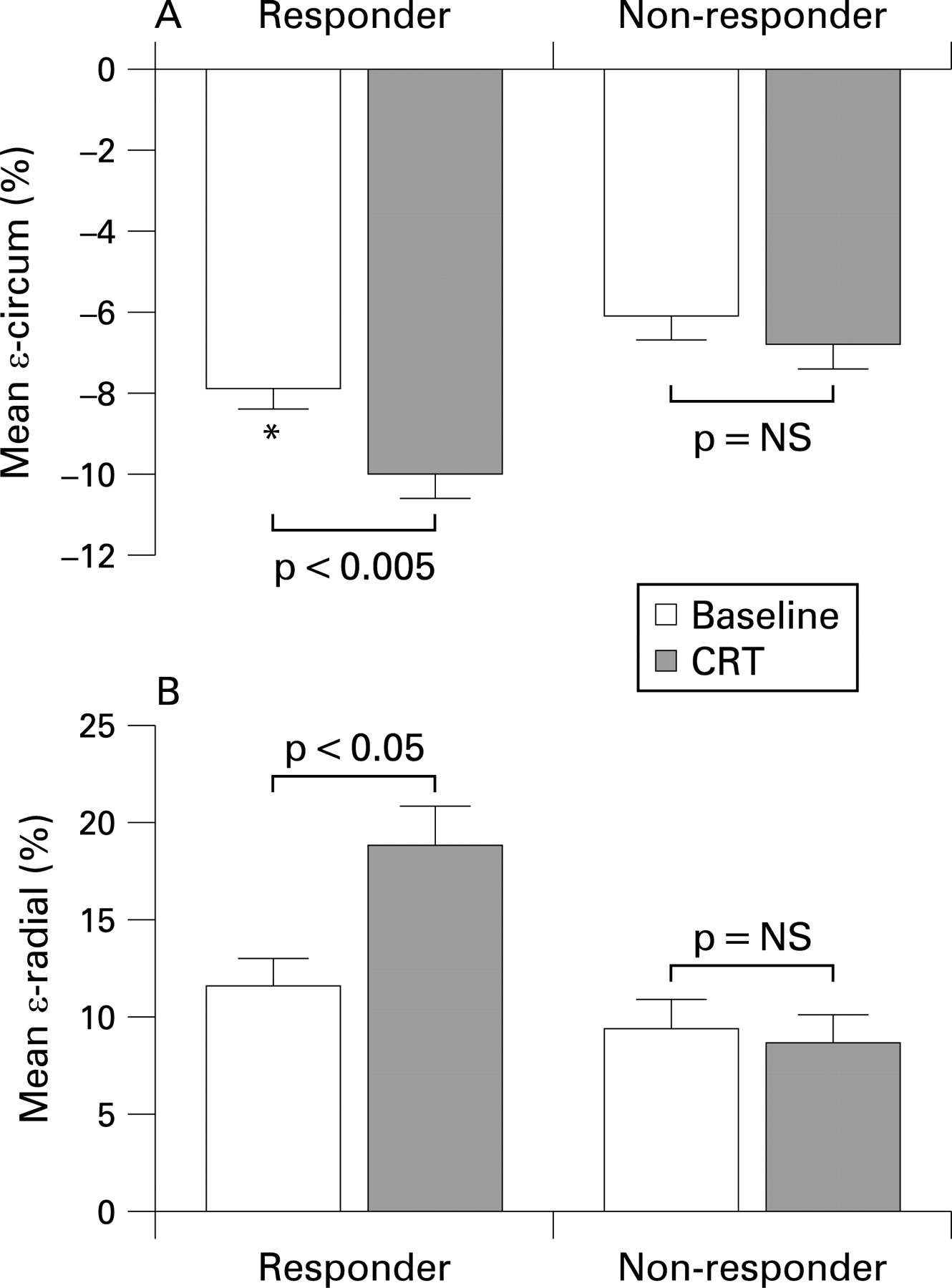
At the end of three months, there were 21 responders of LV reverse remodelling while the other 18 patients were non-responders. The responders showed not only a greater degree of reduction in LVESV (−30.5% (11.4%) vs −4.2% (5.4%), p<0.001) and gain in ejection fraction (10.6% (5.7%) vs 2.6% (2.9%), p<0.001), but also improvement in other echocardiographic parameters—namely, LVEDV, mitral regurgitation, LV length, LV mid-cavity width and sphericity indices (table 2). Since the mid-cavity width was reduced to a greater extent than the length (−8.9% (9.2%) vs −3.4% (6.8%), p = 0.006 for end-diastole; −11.0% (13.1%) vs −5.8% (7.5%), p = NS for end-systole), the LV became less globular in shape. On the contrary, such benefits were not observed in the non-responders (fig 2).
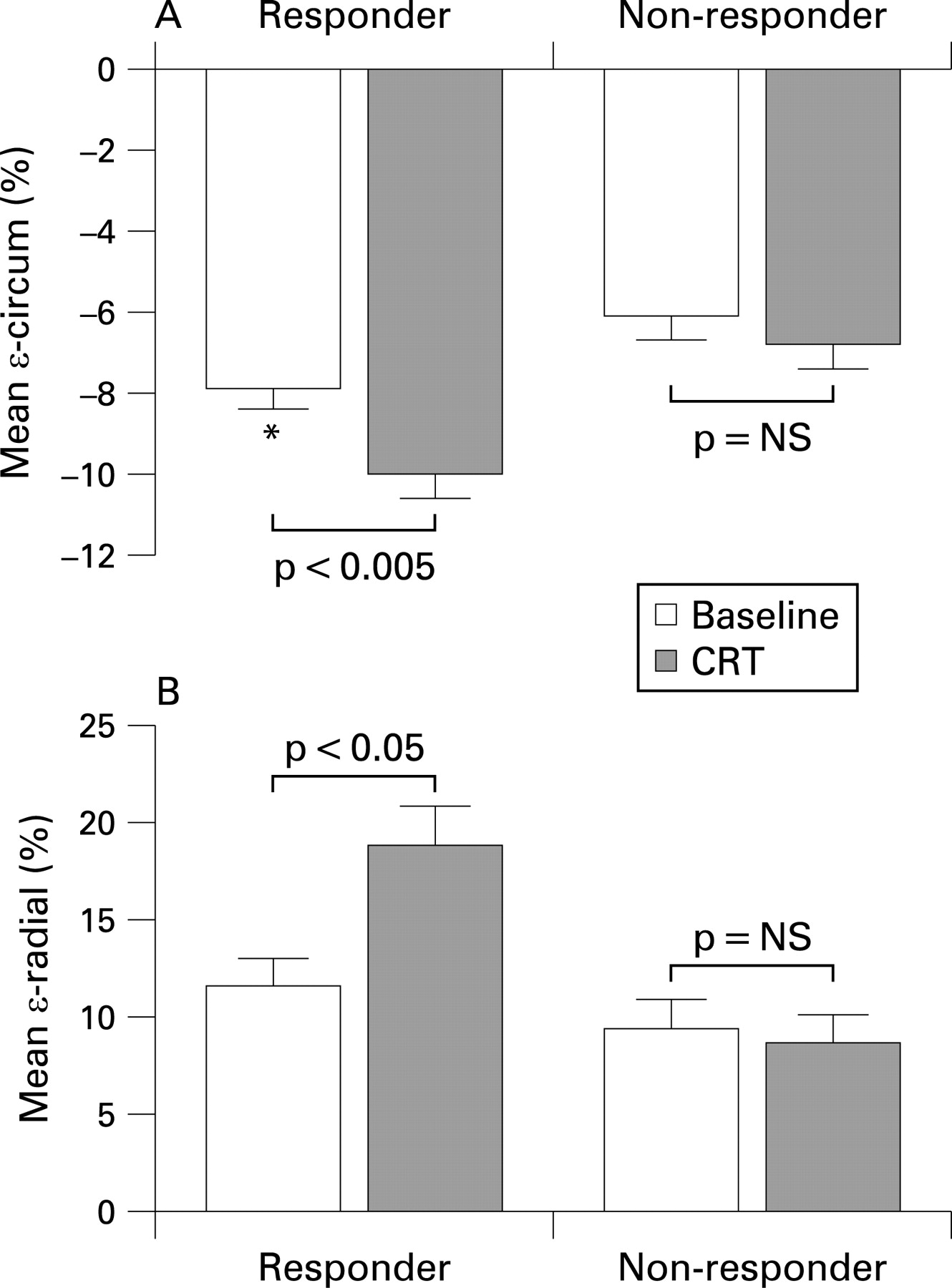
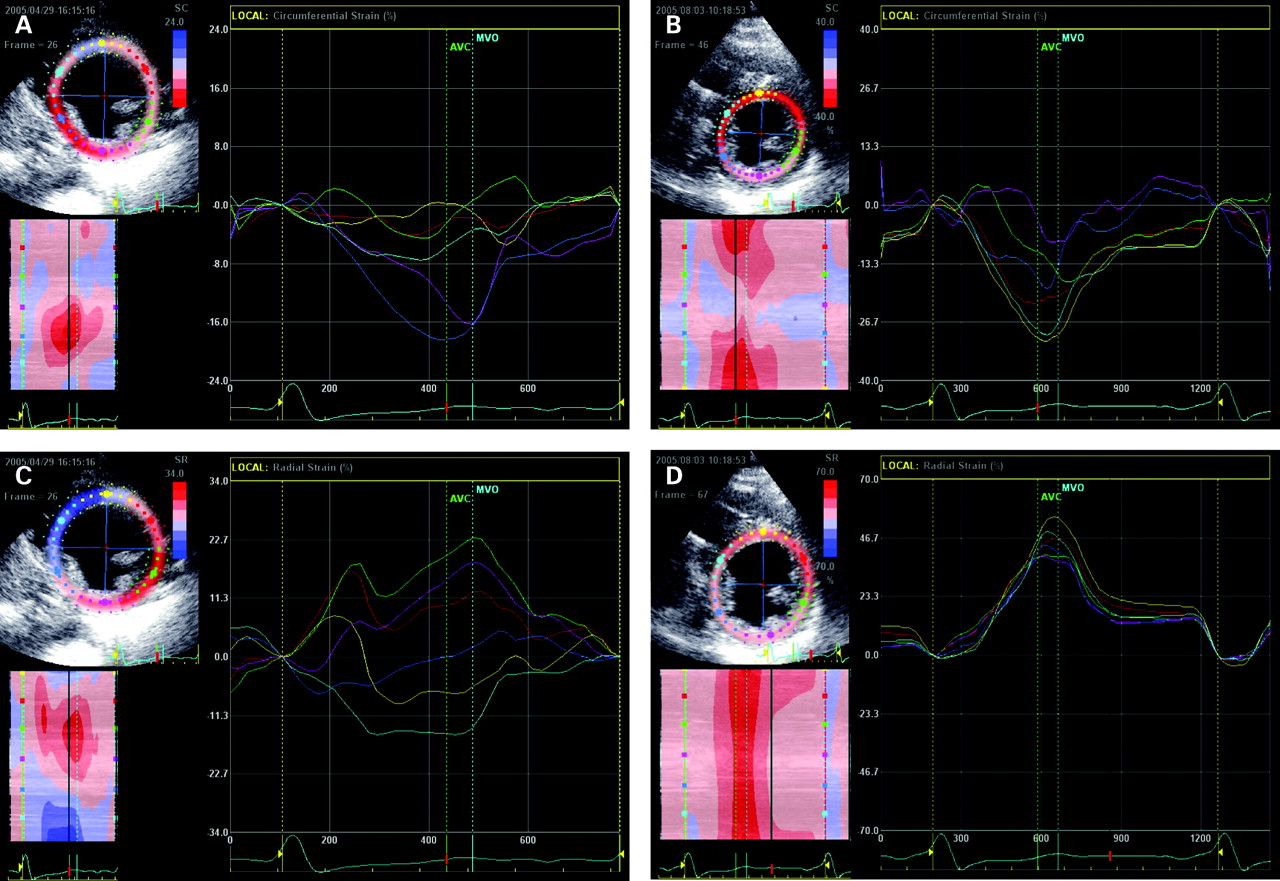
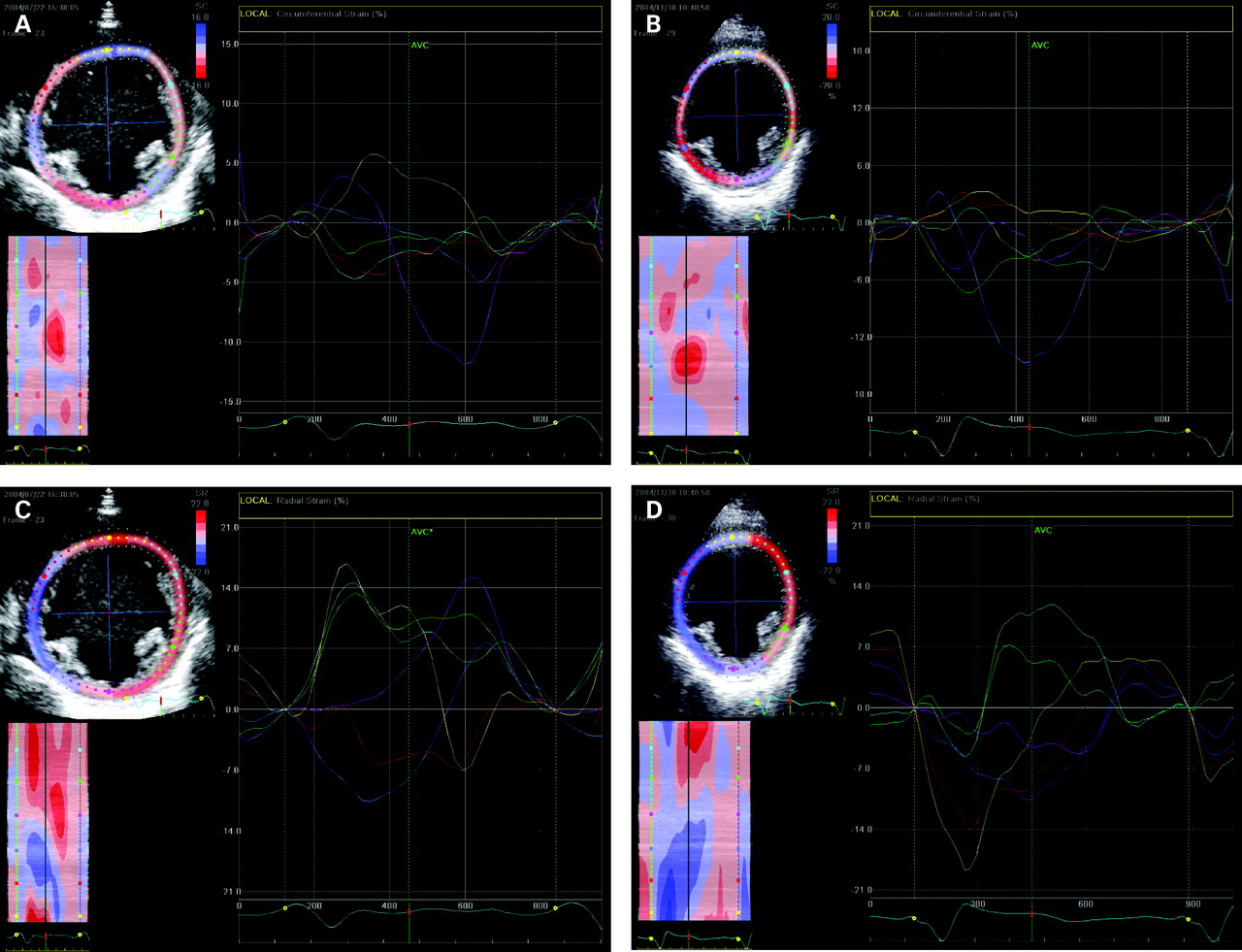
With respect to short-axis myocardial function, the mean ϵ-circum and mean ϵ-radial were significantly increased in the responders after CRT with reduced ϵ-circum-(No) and ϵ-radial-(No) accordingly (table 2) (figs 3 and 4). However, none of the parameters showed any improvement in the non-responders (table 2) (figs 4 and 5). Intriguingly, the torsion had a trend but insignificant decrease in the responders and was significantly worsened in the non-responders. For long-axis function, the mean ϵ-long was not able to show any significant change after CRT in both responders and non-responders (table 2).

Prediction of LV reverse remodelling and improvement of ejection fraction by circumferential strain
There were no differences in the baseline LV volumes and ejection fraction between responders and non-responders; however, the baseline LV end-systolic sphericity index was larger in the responders (p<0.05). With respect to myocardial function, the baseline mean ϵ-circum was greater while the ϵ-circum-(No) was smaller in the responders (both p<0.05) (table 2). From the ROC curve, a cut-off value of mean ϵ-circum ⩾6.5% predicted a gain in LV ejection fraction ⩾5%, with a sensitivity of 73% and a specificity of 71% (area under curve (AUC) = 0.74, CI = 0.58 to 0.90, p<0.05). The same cut-off was also found to predict a reduction of LVESV ⩾15%, with a sensitivity of 67% and a specificity of 67% (AUC = 0.70, CI = 0.54 to 0.87, p<0.05). In contrast, the baseline mean ϵ-radial, ϵ-radial-(No), torsion, torsion-(No), mean ϵ-long and ϵ-long-(No) were not different between the two groups (table 2), neither they were able to predict favourable responses after CRT.
In addition, significant systolic dyssynchrony assessed by Ts-SD was present in 27 patients (69%) at baseline, in which seven patients were found to be non-responders of LV reverse remodelling. However, a lower baseline ϵ-circum <6.5% was observed in four out of the seven non-responders. Intriguingly, when the 39 patients were stratified by the occurrence of dyssynchrony (Ts-SD ⩾33 ms) and/or preservation of short-axis function (ϵ-circum ⩾6.5%), the response rate was much higher (78%) in the patients who fulfilled both criteria. On the contrary, it was the lowest (11%) in the absence of both criteria, and was intermediate (50%) in patients with the presence of either criteria (χ2 = 10.83, p = 0.003) (fig 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
This study comprehensively examined the relation between LV global function, LV geometry and myocardial mechanics in patients with advanced heart failure who received CRT. It was observed that short-term improvement of systolic function and LV reverse remodelling was primarily associated with improvement of short-axis function, but not the long-axis function or LV torsion. This was further supported by the finding that only responders had improvement of the mean ϵ-circum and mean ϵ-radial but not non-responders. Furthermore, a favourable response was at least partially dependent on the relative preservation of short-axis function. In particular, a preserved baseline mean ϵ-circum of ⩾6.5% was able to predict the gain in ejection fraction and LV reverse remodelling.
Short-axis versus long-axis function in heart failure and their changes after CRT
The progression of heart failure is characterised by unrelenting cardiac dilatation and worsening of systolic function—that is, LV remodelling. One of the geometrical changes of LV remodelling is the increase in LV mid-cavity size resulting in a more “globular-shaped” LV. This will further increase the workload of the heart and jeopardise cardiac function. To maintain a normal slender-shaped LV, the short-axis function is crucial. The short-axis function is determined not only by the contraction of LV longitudinal fibres, but also the LV circumferential fibres. In postmortem dissection of the heart, it has been shown that the longitudinal fibres are the major-axis fibres in the LV which aligned at the subepicardial and subendocardial layers and contribute to the majority of systolic function.6 7 The susceptibility of long-axis function to pathological conditions has been observed before clinical symptoms occur or when LV global function is still preserved, such as using tissue Doppler imaging (TDI).16 19 20 Therefore, in a failing heart where the longitudinal muscle fibres are severely dysfunctional, the circumferential muscle fibres may be crucial to compensate and reduce the rate of structural and functional deterioration.
The LV long-axis myocardial function can be easily assessed by TDI in which the lines of Doppler interrogation are almost parallel with the LV long-axis. Despite a dramatic improvement of LV ejection fraction after CRT for three months, the long-axis myocardial systolic velocity was not shown to be improved (or only mildly improved in responders) in previous studies.3 15 In the present study, the ϵ-long using 2D speckle tracking also failed to show any improvement after CRT, which was consistent with previous findings. Furthermore, the angle independency of 2D speckle tracking also enables researchers to investigate other components of myocardial contraction such as ϵ-circum, ϵ-radial and Tor, which has been validated recently by cardiac magnetic resonance imaging (MRI).10–12 Interestingly, there was a significant increase in mean ϵ-circum and mean ϵ-radial in responders of LV reverse remodelling. They also had a favourable change in LV geometry apart from volumetric reduction and gain in ejection fraction. In fact, the shrinkage of LV volume was more easily explained by the reduction of LV mid-cavity width rather than LV cavity length, leading to a favourable increase in sphericity index. Since there was no significant improvement of ϵ-long in the responders, the observed favourable changes in LV systolic function and reverse remodelling after CRT were probably due to the improvement of circumferential fibre function which had been relatively preserved. According to the Laplace’s law, favourable strokework can be achieved by a more slender-shaped heart. In addition, the reduction in the number of segments with paradoxical systolic movement might reflect the improvement of LV short-axis systolic dyssynchrony, which would further facilitate the concerted LV force development during systole.21 It has also been suggested by using cardiac MRI and tagging technologies that circumferential dyssynchrony plays a part in determining cardiac function and response after CRT.22
Preservation of LV short-axis function predicts a favourable response to CRT
LV reverse remodelling response after CRT with reduction in LVESV and gain in ejection fraction has been suggested not only as an objective measure of improvement in cardiac function, but also as a predictor for favourable long-term prognosis.23–25 In addition to the increase in ϵ-circum after CRT, another major finding of this study was that responders had a higher baseline mean ϵ-circum than non-responders, despite similar baseline ejection fraction and mean ϵ-long. Moreover, a baseline mean ϵ-circum of ⩾6.5% predicted improvement in LVESV and ejection fraction. Therefore, it appeared that the relative preservation of LV short-axis function, in particular the circumferential fibre function, would play a pivotal part in mediating the improvement of LV geometry and global function. This might have a “compensatory” role when the long-axis function was severely impaired. For patients with heart failure in whom both long-axis and short-axis fibre functions are severely dysfunctional, they might already be reaching the end-stage or “the point of no return”. Such a contractile reserve deficiency may render the lack of CRT response despite presence of baseline dyssynchrony.
Baseline LV systolic dyssynchrony has been regarded as one of the major factors that predicts favourable CRT response, alongside with other factors such as optimal lead position and proper device programming.26–28 A previous study by cardiac MRI demonstrated that the presence of transmural scar tissue in the posterolateral LV segments provided an incremental value to baseline systolic dyssynchrony for predicting LV reverse remodelling.29 As the presence of significant scar burden may inadvertently reduce the amount of myocardial deformation, the current study also corroborates the previous observation. It appears that the presence or absence of both mean ϵ-circum ⩾6.5% and systolic dyssynchrony will increase the likelihood of occurrence or lack of LV reverse remodelling response.
LV torsion and CRT
LV torsion is another mechanical force that develops during the twisting and shortening of LV fibres, as a result of oblique alignment of longitudinal fibres.8 10 11 LV torsion has been shown to play a part during normal systole and to be reduced in cardiac diseases.9–11 The measured value of torsion in healthy subjects in the present study was similar to that estimated by cardiac MRI as well as by speckle tracking in previous studies.10 11 Although a significant reduction of LV torsion was observed in this study in patients with advanced heart failure, it was not improved after CRT despite significant gains in LV global and short-axis function in responders. In fact, non-responders showed further reduction of LV torsion. Therefore, it appears that LV torsion might not have a role that mediates the favourable changes in cardiac function after CRT. This is also compatible with the other findings as LV torsion is mainly caused by the long-axis fibre contraction, which is situated in an oblique manner and in opposite directions for epicardial and endocardial muscle layers.
Conclusion
The improvement of LV short-axis function rather than long-axis function contributed to the changes in LV global function and geometry after CRT. A relatively preserved mean ϵ-circum of ⩾6.5% might be useful to predict favourable increase in ejection fraction and LV reverse remodelling. In addition, LV torsion and longitudinal strain did not appear to play an important part in mediating CRT benefits.
REFERENCES
Footnotes
Competing interests: None.
Funding: Supported by a research grant from Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong and the SH Ho Cardiovascular and Stroke Centre.