Article Text

Abstract
Coronary artery stenting is increasingly used as a treatment for coronary artery disease. A period of antiplatelet therapy is mandatory following coronary stenting, in order to minimise the risk of stent thrombosis. About 5% of patients who undergo coronary stenting will require non-cardiac surgery within 12 months, and the management of antiplatelet therapy in this setting is complex, requiring a balance between the risks of both operative haemorrhage and stent thrombosis. The available evidence to guide decision-making in the management of antiplatelet therapy in this setting is reviewed.
Statistics from Altmetric.com
Coronary artery stenting is a well-established treatment for coronary artery disease, significantly reducing the rate of restenosis compared with balloon angioplasty. Stenting temporarily denudes the artery of endothelium, leaving the treated segment prone to thrombosis—a condition usually presenting with myocardial infarction (MI) and carrying a high mortality.1 Stenting therefore mandates a subsequent period of antiplatelet therapy, reducing the risk of thrombosis until the stent has endothelialised.
About 5% of patients who undergo coronary stenting require non-cardiac surgery within 12 months.2 Surgery induces a prothrombotic state owing to increased platelet volume and activation, along with perioperative changes in fibrinogen levels and fibrinolytic activity—factors which may predispose to stent thrombosis. Conversely, antiplatelet agents used to prevent stent thrombosis may increase the risk of intraoperative haemorrhage. We explore the existing evidence to guide decision-making for the timing of non-cardiac surgery following stenting, and the use of antiplatelet drugs in this setting.
GUIDELINES FOR ANTIPLATELET THERAPY FOLLOWING CORONARY ARTERY STENTING
American College of Cardiology and American Heart Association (ACC/AHA) guidelines3 for antiplatelet therapy following coronary stenting published in 2006 recommended 1 month of aspirin and clopidogrel after elective implantation of a bare metal stent (BMS), 3 months for sirolimus-eluting stents and 6 months after paclitaxel-eluting stents. These guidelines have since been superseded by Food and Drug Administration recommendations4 for 12 months of dual therapy in patients at low risk of bleeding, after concerns about late thrombosis in drug-eluting stents (DES)—a view endorsed by the British Cardiovascular Intervention Society. European guidelines5 again propose 1 month of dual therapy after implantation of a BMS and at least 12 months for DES, particularly in small vessels, and long or complex lesions such as bifurcations. After this period, clopidogrel may be stopped, but aspirin is then continued long term. Additionally, in patients who undergo stent implantation in the setting of an acute coronary syndrome, at least 12 months of dual therapy is typically recommended regardless of the type of stent used.
BARE METAL STENTS AND NON-CARDIAC SURGERY
In 2000 Kaluza et al6 reported on 40 patients who underwent preoperative revascularisation, demonstrating a heightened risk of perioperative complications in patients with coronary stents. In the 25 patients who underwent surgery within 14 days of stenting, an alarming mortality rate of 32% was found. Overall mortality was 20%, and no deaths occurred when surgery was performed more than 14 days after stent implantation. Of these eight deaths, two were due to proven stent thrombosis, which was also suspected in a further four cases owing to ECG changes in the territory of the stented artery. Five of the eight patients had received no antiplatelet therapy perioperatively (including both patients with confirmed stent thrombosis), two had received ticlopidine but not aspirin, and only one patient had received both agents.
Subsequent reports confirmed an increased risk of perioperative cardiac complications when surgery was performed within 3–6 weeks of stenting,7–9 with mortality rates of up to 25% (table 1). Wilson et al7 reported a much lower rate of perioperative mortality (4%) in a group of 207 patients, with no deaths occurring when surgery was performed more than 6 weeks after percutaneous coronary intervention (PCI). In this group, only 6.3% of patients received no perioperative antiplatelet therapy.
The highest complication rates seem to occur when all antiplatelet therapy is discontinued early after stent implantation. Sharma et al9 reported that of seven people who discontinued thienopyridine therapy (either ticlopidine or clopidogrel) within 3 weeks of stenting, six died in the perioperative period. Among the 20 patients who continued thienopyridine therapy during surgery, there was only one perioperative death. Although the use of aspirin was not specifically mentioned, the authors stated that the six early fatalities were “not receiving antiplatelet therapy”, suggesting that both agents were discontinued.
These studies imply significant risks of cardiac complications when surgery is undertaken within 4–6 weeks of coronary stenting with BMS, particularly when antiplatelet therapy is discontinued. Although a variety of antiplatelet or anticoagulation regimens were in use early in these reports, most patients studied received contemporary treatment with aspirin and a thienopyridine agent (initially ticlopidine and subsequently, clopidogrel).
DRUG-ELUTING STENTS AND NON-CARDIAC SURGERY
Since their introduction, DES have been implanted in increasing proportions of procedures world wide owing to reduced rates of in-stent restenosis compared with BMS. It is known that endothelialisation of DES takes considerably longer than BMS, leading to a longer period at potential risk of stent thrombosis.10 11
Several small retrospective studies of patients undergoing non-cardiac surgery after DES implantation have been reported. In a study by Schouten et al,12 192 patients (93 patients with BMS, 99 with DES) undergoing surgery within 2 years of PCI were retrospectively stratified into early and late surgery groups. These groups were defined by the ACC/AHA recommendations for antiplatelet therapy following PCI (1 month for BMS, 3 months for sirolimus-eluting stents and 6 months for paclitaxel-eluting stents); 30 patients underwent early surgery, and 162 patients late surgery. The major adverse cardiac event (MACE) rate in the early surgery group was 13.3%, of which all were fatal, with no difference between BMS and DES. In all fatal cases both antiplatelet agents were withheld. However, when surgery was performed early, but antiplatelet therapy was continued, the MACE rate was 0%; whether one or both antiplatelet agents were continued is not specified. The MACE rate in the late surgery group was 0.6%—a single fatal left anterior descending coronary artery stent thrombosis 253 days after paclitaxel stent implantation when aspirin was discontinued for surgery, clopidogrel already having been withdrawn.
Compton et al13 reported a zero event rate in 38 patients undergoing a variety of major and minor procedures after DES implantation. Surgery was relatively late, with a median time to surgery of over 260 days. Aspirin was continued in 30/38 patients, and clopidogrel in 16. Kim and colleagues,14 however, raise further concerns about late thrombosis in DES. Of three perioperative stent occlusions reported (from 138 patients undergoing surgery), two occurred at 264 and 367 days after PCI, and again all antiplatelet therapy was withdrawn before surgery. Godet et al15 prospectively assessed 96 patients with previous coronary stenting undergoing non-cardiac surgery. In their study two cases of stent thrombosis occurred, the first within a BMS in a patient with multiple BMS and DES, and the second within a DES placed 32 months previously. In each case both antiplatelet agents had been discontinued several days preoperatively.
More recently, Vicenzi et al2 prospectively identified 103 patients who were due to undergo non-cardiac surgery within 12 months of coronary stenting. Patients with both BMS and DES were included and the median time from PCI to surgery was 103 days. The study protocol required all patients to continue antiplatelet therapy perioperatively, or interrupt it only briefly (<72 h). All patients also received heparin; either unfractionated heparin to achieve an activated partial thromboplastin time ratio >1.5, or enoxaparin at least 1 mg/kg/day. Troponin T was measured on induction and on the first and second postoperative days. The primary end point of death, excess bleeding, MI and a troponin T rise of >0.035 ng/ml occurred in 46 patients (44.7%). In total, 57 adverse events occurred (table 2), including 12 patients who had acute MI, and 22 patients in whom the primary end point was manifest only as a modest troponin rise, with no other markers of MI (median troponin 0.24 ng/ml). These relatively high complications rates occurred despite the continuation of aspirin in over 80% of patients, clopidogrel in over 40% and the universal use of heparin. Only two complications related to bleeding, and mortality of 4.9% was exclusively due to cardiac causes. Time span from PCI to surgery was the only identifiable factor differentiating those with and without adverse events. Surgery within 35 days compared with surgery after 90 days conferred a 2.1-fold risk of an adverse event.
The most important finding to be taken from these studies is that early surgery carries significantly greater risks than delayed surgery. Although the effect of partial discontinuation of antiplatelet therapy is unclear, within the first few months after PCI, aspirin alone may be insufficient. Data beyond 1 year are limited, but isolated reports of stent thrombosis associated with discontinuation of antiplatelet therapy beyond 12 months are a concern.
ANTIPLATELET THERAPY AND PERIOPERATIVE BLEEDING RISK
Concern about the risk of haemorrhage often leads to discontinuation of antiplatelet therapy perioperatively. A meta-analysis of nearly 50 000 patients by Burger et al16 demonstrated that the perioperative use of aspirin increased the rate of occurrence of minor bleeding complications by 50%. However, the incidence of major bleeding episodes was unchanged except in neurosurgery and prostatic surgery. Other reports have suggested an excess of minor bleeding related to the use of clopidogrel—for example, haematoma following pacemaker implant,17 and bleeding during cataract surgery18 and transbronchial biopsy.19 Data regarding bleeding and clopidogrel use in non-cardiac surgery remains unclear, however, owing to small patient numbers, the variety of procedures undertaken in studies and the absence of clear control groups.
For coronary artery bypass surgery, the CURE trial20 demonstrated excess major bleeding in the 912 patients in whom clopidogrel was not stopped ⩾5 days before surgery (9.6% vs 6.3% in the placebo group). Other data show similar findings to those of the CURE study, demonstrating that rates of intraoperative blood loss, postoperative chest drain blood loss, reoperation for bleeding and requirement for transfusion are consistently found to be higher in patients receiving clopidogrel,21 with occasional exceptions.22
It is likely that the clinical consequences of any increase in operative bleeding are highly dependent on the type of surgery undertaken. Minor bleeding during neurosurgery or ophthalmic procedures might have profoundly different sequelae than those during hip replacement surgery, for example. The type of surgery and the perceived consequence of any increase in bleeding should therefore be carefully considered for each individual patient.
INDICATIONS FOR CORONARY REVASCULARISATION IN PATIENTS UNDERGOING NON-CARDIAC SURGERY
The use of PCI before non-cardiac surgery has previously been widely practised, in an intuitive attempt to reduce the rate of perioperative cardiac complications in patients with known coronary artery disease. This practice has decreased, however, after the accumulation of data suggesting that preoperative coronary revascularisation has little impact on perioperative cardiac event rates when performed solely for this purpose.23
The ACC/AHA guidelines for preoperative cardiac assessment24 state that preoperative coronary revascularisation should be considered in the following circumstances:
acute ST elevation MI;
high-risk unstable angina or non-ST elevation MI;
stable angina with left main stem stenosis;
stable angina with three-vessel coronary artery disease;
stable angina with two-vessel disease involving proximal left anterior descending coronary artery, and either left ventricular ejection fraction <50% or demonstrable ischaemia during non-invasive testing.
Essentially, this comprises a group of patients in whom revascularisation, either by percutaneous or surgical means, is indicated for either symptomatic or prognostic reasons, regardless of the need for non-cardiac surgery. As in any other setting, when planning perioperative revascularisation, the risks and benefits of each strategy should be assessed, and the decision-making process should take into account many aspects, including the patients’ symptoms and comorbidities, coronary anatomy, degree of associated ischaemia and also the urgency and type of surgery to be performed. The guidelines also recommend that in patients who require PCI for any of the above indications, and who will require non-cardiac surgery within 12 months, that a strategy of balloon angioplasty alone, or BMS placement with 4–6 weeks of subsequent antiplatelet therapy is performed.
The chosen method of revascularisation is important. Coronary artery bypass grafting (CABG) surgery may be advantageous in patients with multivessel disease, owing to the reduced requirement for dual antiplatelet therapy. Additionally, angiographic studies have demonstrated that perioperative coronary events do not always originate at the site of severe coronary stenosis, and may be associated with the presence of only mild coronary narrowing.25 CABG surgery may therefore provide greater protection against perioperative events, by shielding against events occurring at any point along the grafted artery, rather than solely within the stented segment. Nevertheless, the risks and benefits in each patient should be carefully considered.
In patients in whom a strategy of coronary stenting is employed preoperatively, particular attention should be paid to the stent implantation technique, as poor stent deployment is known to be associated with an increased risk of stent thrombosis.26 The use of intravascular ultrasound to ensure complete apposition of stent struts should be considered in this setting.
In the future, new techniques of intracoronary imaging, such as optical coherence tomography, may be used in order to ensure complete coverage of stent struts by re-endothelialisation. This may allow identification of patients of higher risk of perioperative thrombotic complications, although at present no such validation of this technique exists.27 28
AHA SCIENCE ADVISORY PANEL
Concern about premature discontinuation of antiplatelet therapy in patients with DES and the subsequent risk of stent thrombosis, has recently led to several recommendations by an AHA science advisory panel29 (box 1).
Box 1 ACC/AHA science advisory panel29 recommendations
Consider the use of bare metal stents or balloon angioplasty rather than drug-eluting stents (DES) in patients due to undergo non-cardiac surgery within 12 months
Healthcare providers to only discontinue antiplatelet therapy after discussion with the patient’s cardiologist
Patient education to ensure that patients understand the need for continuous antiplatelet therapy and the risks of premature discontinuation
Postpone elective procedures with a significant bleeding risk for 12 months after stenting
For patients with DES where clopidogrel must be discontinued, continue aspirin, restarting clopidogrel as soon as possible after the procedure
Similar recommendations have been made by a French task force comprising cardiologists, anaesthetists, haematologists and surgeons.30 The task force emphasises the multidisciplinary decision-making process, and states that all relevant specialties should be involved in the preoperative assessment phase for patients with coronary stents. They propose a compromise in situations where dual antiplatelet therapy cannot be discontinued owing to a high perceived risk of stent thrombosis: to continue aspirin, discontinuing clopidogrel 5 days preoperatively. Based on the platelet half-life of 10 days, this allows the platelet pool to partially replenish before surgery. Administration of a 600 mg loading dose postoperatively would then rapidly re-establish maximal platelet inhibition. In situations where surgical bleeding would carry excessive risk of complications (eg, neurosurgical or ophthalmic procedures), and antiplatelet therapy must be discontinued, the task force recommend that substitution of antiplatelet therapy with either heparin, or a non-steroidal anti-inflammatory drug be considered. The task force concede, however, that this recommendation is purely empirical, with no supporting evidence.
PERIOPERATIVE SUBSTITUTION OF ANTIPLATELET THERAPY
Replacement of standard oral antiplatelet therapy with a short-acting agent to act as a bridge for the period between discontinuation of clopidogrel and/or aspirin and surgery has been suggested. Protocols involving the use of intravenous unfractionated heparin, and short-acting platelet antagonism with infusions of either eptifibatide31 or tirofiban32 have been proposed. These agents may be discontinued several hours before surgery, and restarted shortly afterwards, minimising the time during which platelet aggregation and stent thrombosis may occur. Although these protocols are attractive intuitively, and their successful use has been reported in small case series, there is currently no controlled evidence to support their use.
STENTS WITH PRO-HEALING SURFACES
Continuing development in stent technology may render concerns about the long duration of antiplatelet therapy necessary following DES implantation obsolete. A number of different pro-healing surfaces are becoming available which may allow much more rapid and complete endothelialisation of the stented segment. The Genous-R stent consists of a standard stainless steel stent, which is coated in a matrix containing monoclonal antibodies targeted specifically at the CD34 receptor. This receptor is exclusive to the surface of endothelial progenitor cells, which are preferentially captured onto the stent surface. Once attached to the stent surface, the endothelial progenitor cells mature into endothelial cells, rapidly creating a smooth endothelial surface within the stented segment without the risk of restenosis. These stents are already in limited human use, and low event rates have been demonstrated in small numbers of patients despite dual antiplatelet therapy being administered for only 28 days.33 A recent study reports on a series of 22 patients in whom biological stents were used before life-saving and undeferable major non-cardiac surgery. Despite a mean duration of antiplatelet therapy of only 12.5 days, no perioperative cardiac complications were reported.34 Aspirin was continued postoperatively as the sole antiplatelet agent.
These pro-healing surfaces have yet to be combined with anti-proliferative drug elution, and so at present should be compared with BMS alternatives rather than with DES platforms. Further evaluation of this new technology is continuing, and studies in larger numbers of patients are clearly necessary.
SUMMARY AND CONCLUSIONS
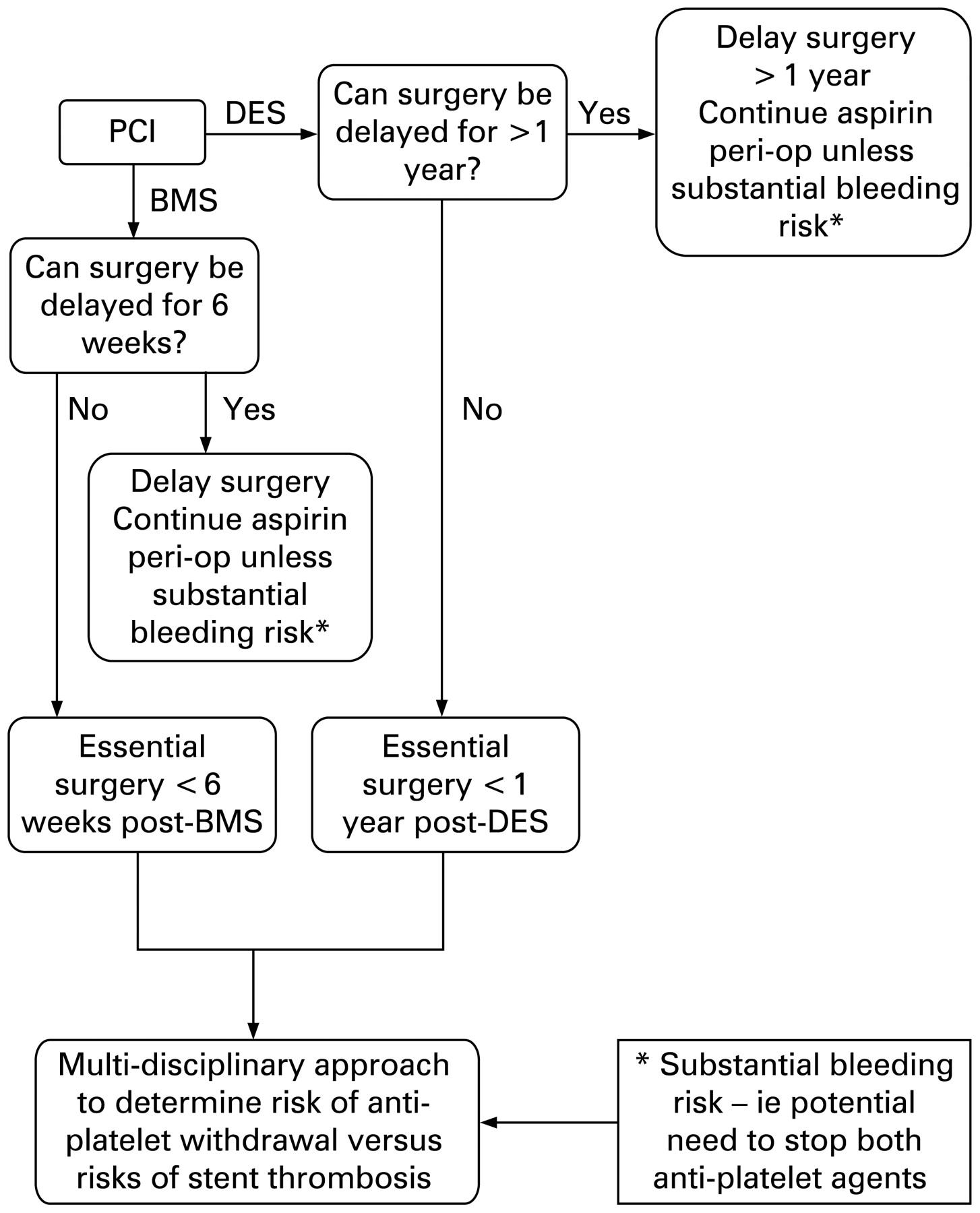
A series of decisions must be made in a patient with coronary artery disease who requires future major non-cardiac surgery. Initially, the cardiologist must decide whether it is necessary that revascularisation takes place before surgery. Multidisciplinary discussion between the cardiologist, cardiac surgeon, surgeon performing the non-cardiac surgery, anaesthetist and other relevant parties should take place at this stage. If revascularisation is warranted, the next step is to determine the form of revascularisation—PCI or CABG? Should PCI be performed preoperatively, then decision about stent type must be based upon several factors, including characteristics of the lesion to be treated, and the type and urgency of the surgery. PCI using DES should ideally not be planned unless non-cardiac surgery can be delayed for >1 year and aspirin continued perioperatively. Similarly, BMS should only be used if surgery can be delayed >6 weeks and aspirin continued perioperatively. Figure 1 expresses these steps as an algorithm. The need for non-cardiac surgery may become apparent only after PCI has been performed. In this setting, non-cardiac surgery should be avoided for 4–6 weeks for BMS unless immediately life-saving. Surgery after this period is associated with a much lower risk of stent thrombosis. Surgery within 3–6 months of DES implantation also substantially increases the risk of cardiac complications, both during and without antiplatelet therapy. Non-urgent surgery should ideally be delayed for at least 12 months. Surgery which cannot be delayed should be performed on dual antiplatelet therapy whenever possible (fig 2). It appears that discontinuation of either agent carries an increased perioperative risk early after stenting. Even beyond 12 months, reports of late stent thrombosis suggest that at least one antiplatelet agent should be continued perioperatively when possible. These risks of late surgery in patients with DES must be assessed individually and a decision reached on a multidisciplinary basis.

Antiplatelet therapy algorithm for percutaneous coronary intervention before elective non-cardiac surgery. BMS, bare metal stents; CABG, coronary artery bypass grafting; DES, drug-eluting stents; PCI, percutaneous coronary intervention.

{kind=link}
{kind=link}
Antiplatelet therapy algorithm in patients undergoing unexpected non-cardiac surgery following recent coronary intervention. BMS, bare metal stents; DES, drug-eluting stents; PCI, percutaneous coronary intervention.
Finally, all healthcare professionals should be aware that stopping aspirin and/or clopidogrel could be a life-threatening decision, only to be taken in discussion with the cardiologist who initiated these treatments. The use of patient “clopidogrel cards” and regular education for both patients and staff might help avoid the occurrence of serious but predictable adverse events.
REFERENCES
Footnotes
Competing interests: None.