Article Text

Abstract
Objective: The evaluation of novel biomarkers for the diagnosis of acute destabilised heart failure (HF).
Design: Prospectively conducted study on diagnostic accuracy.
Setting: Emergency department of a tertiary care hospital.
Patients: 251 consecutive patients presenting to the emergency department with dyspnoea as the chief complaint.
Main outcome measures: Index tests were plasma concentrations of 10 biomarkers (BNP, MR-proANP, MR-proADM, copeptin, CT-proET-1, ST2, adiponectin, chromogranin A, proguanylin and prouroguanylin). The reference standard was the diagnosis of acute destabilised HF, which was based on the Framingham score for HF plus echocardiographic evidence of systolic or diastolic dysfunction.
Results: Median plasma concentrations of all 10 biomarkers were higher in patients with dyspnoea attributable to acute destabilised HF (n = 137) than in patients with dyspnoea attributable to other reasons (n = 114). Applying receiver operating characteristic curve (ROC) analyses, areas under the curve (AUCs) for BNP (0.92) and MR-proANP (0.88) were significantly higher than the AUCs of the other eight biomarkers (MR-proADM, 0.75; adiponectin, 0.73; CT-proET-1, 0.72; proguanylin, 0.68; ST2, 0.67; prouroguanylin, 0.62; copeptin, 0.62; and chromogranin A, 0.56). In multivariate logistic regression analysis only increased BNP and MR-proANP concentrations remained independent markers for the diagnosis of HF. Both markers alone or in combination added similar diagnostic information besides all clinical information available in the emergency department.
Conclusions: The data showed that BNP and MR-proANP were the only independent diagnostic markers of HF. Both markers provided similar diagnostic information and were clinically useful as an aid in the diagnosis of acute destabilised HF in an emergency setting.
Statistics from Altmetric.com
B-type natriuretic peptide (BNP) and amino-terminal proBNP (NT-proBNP) are well established biomarkers for the emergency diagnosis of acute destabilised heart failure (HF) in patients with dyspnoea.1 2 3 4 In addition, both peptides have been implemented in the routine algorithms for the diagnosis of HF.5 6 However, HF results not only from cardiac overload or injury, but also from a complex interplay among neurohormonal, inflammatory and other biochemical mechanisms.7 To optimise the diagnosis of acute destabilised HF in an emergency setting, these complex mechanisms could be addressed by diagnostic strategies. A single biomarker alone is considered not sufficient for a correct diagnosis in this setting, and a multi-marker approach might be more efficacious for an improved diagnostic accuracy.7 8
We have previously compared head to head the diagnostic accuracies of BNP and NT-proBNP for the diagnosis of acute destabilised HF in an emergency setting.4 Furthermore, we have demonstrated in the same study cohort that increased plasma concentrations of BNP, midregional pro-A-type natriuretic peptide (MR-proANP), midregional proadrenomedullin (MR-proADM), the C-terminal part of the arginine vasopressin prohormone (Copeptin), the soluble isoform of a interleukin-1 receptor family member ST2 (sST2), chromogranin A and the C-terminal endothelin-1 precursor fragment (CT-proET-1) are predictive for one-year mortality in the patients diagnosed with acute destabilised HF.9 10 11 In addition, we have similarly evaluated the prognostic value of adiponectin, a novel adipocytokine, in those same patients.12 There are two other interesting candidate peptides—guanylin and uroguanylin. Both peptides are synthesised as prohormones (proguanylin and prouroguanylin), require proteolytic processing, elicit natriuresis by activating specific guanylate cyclase receptors in the kidney, and increased concentrations been reported in patients with HF.13 14 15
The aim of the present study was to evaluate the utility of established and novel biomarkers (BNP, MR-proANP, MR-proADM, copeptin, CT-proET-1, sST2, adiponectin, chromogranin A, proguanylin and prouroguanylin) for the diagnosis of acute destabilised HF in patients with shortness of breath presenting to an emergency department.
Methods
Study sample
The present evaluation is a post hoc analysis of a previously described study cohort.4 16 In brief, 251 consecutive patients consulting the emergency department of the St John of God Hospital (Linz, Austria) with dyspnoea as a chief complaint were prospectively studied to compare head to head the diagnostic accuracies of BNP and NT-proBNP for acute destabilised HF in an emergency setting.4 The diagnosis of acute destabilised HF was based on the Framingham score for HF plus echocardiographic evidence of systolic or diastolic dysfunction.4 Patients were defined as having systolic dysfunction if their left ventricular ejection fraction (LVEF) was ⩽50%. Patients with a LVEF >50% were further examined for diastolic dysfunction. Each of these patients underwent pulsed wave Doppler examination of mitral inflow before and during the Valsalva manoeuvre. Diastolic dysfunction was defined as impaired relaxation or restrictive or pseudonormal pattern. Systolic HF was defined according to the Framingham score for HF plus echocardiographic evidence of systolic dysfunction (that is, LVEF ⩽50%). Diastolic HF (heart failure with preserved ejection fraction) was defined according the Framingham score for HF plus LVEF >50% and echocardiographic evidence of diastolic dysfunction. The present evaluation was performed and described according to the criteria recommended by the standards for reporting of diagnostic accuracy (STARD) initiative.4 17 The study protocol was approved by the local ethics committee in accordance with the Declaration of Helsinki. All study participants gave informed consent.
Biochemical analysis
During the initial patient examination in our emergency department blood samples were collected for the measurement of BNP concentrations and were analysed within the next 4 hours by a commercially available assay, an AxSYM analyser (Abbott Diagnostics). Aliquots of these EDTA-plasma samples were stored at −80°C for further analyses. MR-proANP, MR-proADM, copeptin and CT-proET-1 were measured by sandwich immunoluminometric assays (BRAHMS AG); sST2 was measured with a sandwich double monoclonal antibody ELISA method (Medical & Biological Laboratories); adiponectin was measured with a commercially available sandwich ELISA (BioVendor Laboratory Medicine Inc); and CgA was determined by a radioimmunoassay (EuroDiagnostica), as previously described.9 10 11 12 Another aliquot from each study participant was used for the determination of plasma proguanylin and prouroguanylin concentrations. In the present work we measured proguanylin and prouroguanylin fully automated on a BEP 2000 instrument (Dade Behring) with a commercially available sandwich ELISA (BioVendor Laboratory Medicine Inc). All 251 plasma samples were measured in one batch approximately three years after blood collection in a blinded fashion to the clinical features and the biochemical data.
Statistical methods
Statistical analysis was performed using the SPSS version 13.0 software (SPSS Inc) and the MedCalc 10.0.0.0 package (MedCalc Software). All probabilities were two tailed and p values <0.05 were regarded as significant. Univariate comparisons were performed with the Fisher’s exact test for the categorical variables and with the non-parametric Mann–Whitney U test for the continuous variables (respective p values were not adjusted for multiple comparisons, and are therefore only descriptive). Receiver operating characteristic (ROC) plots were constructed and areas under the curve (AUCs) for the diagnosis of HF were calculated for all 10 analytes. The respective AUCs were compared according to the method of Hanley and McNeil.18 Cut-off concentrations for all biomarkers were determined according to the 90% sensitivity criterion derived directly from the ROC curves. These cut-off concentrations render the emergency diagnosis of HF unlikely as described in a consensus statement.6 Positive and negative predictive values at these cut-off concentrations were calculated by use of the ratio of cases in the positive and negative groups (reflecting the prevalence of the disease in our study population). In a secondary analysis separate ROC plots were also constructed for the diagnosis of systolic and diastolic HF. Logistic regression analyses were performed to determine whether the biomarker plasma concentrations above the respective cut-off concentrations were independent diagnostic markers for acute destabilised HF.
Results
Biomarker concentrations in patients with shortness of breath
Of the 251 patients with dyspnoea as a chief complaint, 137 were classified as having dyspnoea attributable to acute destabilised HF, and 114 patients were classified as having dyspnoea attributable to other reasons. Demographic and clinical characteristics of the study participants according to HF classification are given in table 1. Median BNP, MR-proANP, MR-proADM, copeptin, CT-proET-1, sST2, adiponectin, chromogranin A, proguanylin and prouroguanylin concentrations were higher in the patients with dyspnoea attributable to acute destabilised HF than in the patients with dyspnoea attributable to other reasons.
Patient characteristics according to HF classification (n = 251)
Biochemical diagnosis of acute destabilised HF
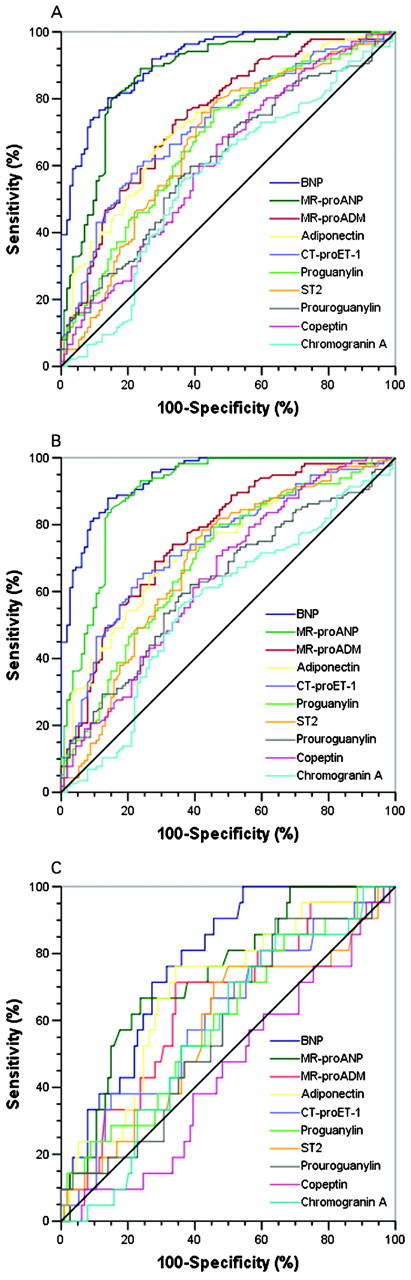
In distinguishing between patients with dyspnoea caused by acute destabilised HF (n = 137) and patients with dyspnoea attributable to other causes (n = 114), the AUCs were 0.92 (95% CI 0.87 to 0.95) for BNP; 0.88 (0.83 to 0.91) for MR-proANP; 0.75 (0.69 to 0.81) for MR-proADM; 0.73 (0.67 to 0.79) for adiponectin; 0.72 (0.66 to 0.79) for CT-proET-1; 0.68 (0.61 to 0.75) for proguanylin; 0.67 (0.60 to 0.74) for sST2; 0.62 (0.55 to 0.69) for prouroguanylin; 0.62 (0.55 to 0.69) for copeptin; and 0.56 (0.49 to 0.64) for chromogranin A. Corresponding ROC plots are displayed in figure 1A. The AUCs for BNP and MR-proANP were significantly higher compared with AUCs of the other eight biomarkers (p<0.001). The complete information, including the appropriate decision statistics, for the biochemical diagnosis of acute destabilised HF at the 90% sensitivity criterion in patients with shortness of breath are listed in table 2.

{kind=link}
Receiver operating characteristic (ROC) curves for the biochemical diagnosis of acute destabilised heart failure (HF) by established and novel biomarkers in patients with shortness of breath presenting to the emergency department. (A) Entire cohort (137 patients with dyspnoea attributable to systolic HF or diastolic HF vs 114 patients with dyspnoea from other causes). (B) Diagnosis of systolic HF (116 patients with dyspnoea attributable to systolic HF vs 114 patients with dyspnoea from other causes). (C) Diagnosis of diastolic HF (21 patients with dyspnoea attributable to diastolic HF vs 114 patients with dyspnoea from other causes). BNP, B-type natriuretic peptide; Copeptin, C-terminal part of the arginine vasopressin prohormone; CT-proET-1, C-terminal endothelin-1 precursor fragment; MR-proADM, midregional proadrenomedullin; MR-proANP, midregional pro-A-type natriuretic peptide; NT-proBNP, amino-terminal proBNP; sST2, soluble isoform of a interleukin-1 receptor family member ST2.
Diagnostic information for the biochemical diagnosis of acute destabilised HF by established and novel biomarkers at the 90% sensitivity criterion in patients with shortness of breath presenting to the emergency department
In a secondary analysis we constructed separate ROC plots for the diagnosis of systolic HF (that is, 116 patients with dyspnoea attributable to systolic HF vs 114 patients with dyspnoea caused by other reasons) and diastolic HF (that is, 21 patients with dyspnoea attributable to diastolic HF vs. 114 patients with dyspnoea caused by other reasons). The respective results were similar to those detailed in the previous paragraph in that the AUCs of BNP and MR-proANP were higher than those of the other eight biomarkers as demonstrated by figures 1B and 1C. For the diagnosis of systolic HF the AUC was 0.94 (95% CI 0.90 to 0.97) for BNP and 0.90 (0.86 to 0.94) for MR-proANP. For the diagnosis of diastolic HF the AUC was 0.78 (0.70 to 0.84) for BNP and 0.74 (0.65 to 0.81) for MR-proANP, respectively.
Independent diagnostic value of each biomarker
To test for an independent diagnostic value of each biomarker we performed a logistic regression analysis including all 10 markers in one model (table 3). Detailed data are given in table 3 and in this analysis only BNP and MR-proANP remained independent markers for the diagnosis of acute destabilised HF. Therefore, for all further analyses we only considered these two markers but not the other eight which were not independently associated with the correct diagnosis (MR-proADM, copeptin, CT-proET-1, sST2, adiponectin, chromogranin A, proguanylin and prouroguanylin).
Independent diagnostic value of each biomarker for acute destabilised HF
In the next step of our evaluation we aimed at comparing the diagnostic accuracies of BNP and MR-proANP alone or combining both markers in one model (table 4, models 1–3). With respect to the overall diagnostic accuracy of the three statistical models, there was a negligible difference between the different approaches (diagnostic accuracy 83% for BNP alone, diagnostic accuracy 80% for MR-proANP alone and diagnostic accuracy 84% for the combined model).
Diagnostic value of increased BNP and MR-proANP plasma concentrations for acute destabilised HF with and without consideration of clinical variables available at the emergency department
Next we were interested in whether the inclusion of the clinical information available in the emergency department (age, sex, estimated glomerular filtration rate, history of acute destabilised HF, and the presence of orthopnoea, paroxysmal nocturnal dyspnoea, nocturnal cough, jugular venous distension, pulmonary rales, third heart sound and peripheral oedema) changed the overall diagnostic accuracy of the statistical approach. Combining the clinical information with BNP or MR-proANP or both markers resulted in a slightly increased overall diagnostic accuracy. The diagnostic accuracy for the whole statistical model was 84% for BNP and clinical information, 85% for MR-proANP and clinical information and 87% for the combination of BNP, MR-proANP and clinical information (table 4, models 4–6). When we performed a logistic regression analysis with all clinical information available in the emergency department but excluding BNP and MR-proANP, we obtained a diagnostic accuracy of 79%.
Discussion
Results from this comparative evaluation of established and novel biomarkers for the diagnosis of acute destabilised HF in an emergency setting showed that BNP and MR-proANP were the only independent diagnostic biomarkers for ruling out acute destabilised HF in patients with shortness of breath. Both markers added similar diagnostic information to clinical variables available in the emergency department. There was no clinically relevant increase in diagnostic accuracy when both markers were combined in one statistical approach.
As stated previously, natriuretic peptide testing is now widely used in clinical practice and is incorporated into cardiovascular guidelines for the diagnosis of HF.5 6 However, the diagnosis of acute destabilised HF remains a challenge and several novel biomarkers are currently under investigation for improving diagnosis, for risk stratification and for monitoring of the treatment of these patients. Of these candidate biomarkers, adrenomedullin, endothelin-1, and the more stable fragments of their precursor peptides (MR-proADM and CT-proET-1) have been shown to be strong prognostic markers in patients with HF and acute myocardial infarction.9 19 20 Furthermore, reports on neurohormones like copetin and chromogranin A have demonstrated that increased concentrations are present in patients with HF and both markers are associated with poor clinical outcome.9 11 21 22 In addition, it has recently been demonstrated that circulating sST2 seems to be an excellent marker for risk stratification in patients with acute destabilised HF.10 23 Even adiponectin is a predictor of mortality in patients with acute destabilised HF independent of clinical confounders and BNP.12 Finally, we included two other interesting natriuretic peptides—namely, proguanylin and prouroguanylin, into our comparative evaluation for the diagnosis of HF. There exists so far only scarce but promising data on these peptides in patients with HF.13 15
In our study, however, only the established biomarkers BNP and MR-proANP remained strong and independent markers for the diagnosis of acute destabilised HF, whereas all other biomarkers evaluated in this study failed to add independent diagnostic information. Consequently, these biomarkers are probably not useful for diagnostic purposes in an emergency setting. Nevertheless, the use of these biomarkers might be of further interest for risk stratification in patients with HF.
The fact that BNP and MR-proANP proved to be applicable for diagnostic purposes in our study is conceivable because both reflect the pathophysiological conditions in HF. Patients with acute destabilised HF have cardiac overload and increased cardiac wall stretch is the trigger for the release of cardiac natriuretic peptides (that is, ANP and BNP). Both peptides cause diuresis and natriuresis, inhibit the renin-angiotensin-aldosterone system and act as vasodilators.24 Thus, the actions of ANP and BNP may oppose the pathophysiological abnormalities in acute destabilised HF. However, as we observed no relevant increase in the diagnostic accuracy in combining BNP and MR-proANP in comparison with the measurement of either BNP or MR-proANP alone, the statement is justified that a dual-marker approach does not provide improved diagnostic information in clinical practice. In contrast, the other biomarkers (MR-proADM, copeptin, CT-proET-1, sST2, adiponectin, chromogranin A, proguanylin and prouroguanylin) do not reflect the pathophysiological conditions of cardiac stretch specifically but are involved in other non-cardiac diseases.25 26 27 28 29 30 Thus, these markers cannot be considered cardiac specific. This might be the reason why they apply for risk stratification in acute destabilised HF (often being associated with several comorbidities such as pneumonia, COPD, etc) but are not useful for diagnostic purposes in an emergency setting.
Compared with other studies in this field the strengths of our trial are the stringent study design reported according to the STARD initiative,17 the performance of echocardiography in each patient within three days after their enrolment (assessing both systolic and diastolic dysfunction) and the large number of novel biomarkers for comparative evaluation. The major limitation of the present study is that this was a post hoc evaluation of the diagnostic capability of several novel biomarkers in an emergency setting. We also have to acknowledge that our study is a single-centre study performed in a relatively small sample of predominantly male patients and may not accurately represent the general demographics of patients presenting with acute destabilised HF to other emergency departments.
In conclusion, the present comparative evaluation of established and novel biomarkers for the diagnosis of HF demonstrated that BNP and MR-proANP are the only independent diagnostic markers of HF. Both markers provided similar diagnostic information and were clinically useful as an aid in the diagnosis of acute destabilised HF in an emergency setting.
REFERENCES
Footnotes
Funding We thank Abbott Diagnostics, BRAHMS AG, Critical Diagnostics and BioVendor Laboratory Medicine Inc for providing reagents free of charge.
Competing interests TM has received speaking fees from Abbott Diagnostics, and BRAHMS AG.
Provenance and peer review Not commissioned; externally peer reviewed.