Article Text

Abstract
Objective: To investigate determinants of, and outcomes from, coronary angiography and intervention in patients with non-ST-segment elevation myocardial infarction (NSTEMI).
Design: Observational study.
Setting: 44 British hospitals with interventional facilities.
Patients: 13 489 admissions with NSTEMI; July 2005 to December 2006.
Main outcome measures: Rate of angiography during index admission; death and readmission to hospital within 180 days.
Results: Significantly lower rates of angiography were seen for women, the elderly, the most deprived and those having cardiac, and most non-cardiac, comorbidities. Performance of angiography, compared with no angiography, was not associated with lower rate of readmission (multiple adjusted hazard ratio (HR) = 0.96, 95% CI 0.74 to 1.24) unless accompanied by coronary intervention (HR = 0.73, 95% CI 0.56 to 0.95). Angiography was associated with reduction in 180-day mortality for survivors of hospitalisation (HR = 0.59, 95% CI 0.49 to 0.72); with greater reduction when followed by an intervention (HR = 0.34, 95% CI 0.28 to 0.42). This mortality benefit after intervention was seen both in women (HR = 0.42, 95% CI 0.29 to 0.60) and men (HR = 0.31, 95% CI 0.24 to 0.41), and across age groups: <65 years (HR = 0.25, 95% CI 0.14 to 0.44), 65–79 years (HR = 0.29, 95% CI 0.22 to 0.39) and ⩾80 years (HR = 0.52, 95% CI 0.37 to 0.74). Mortality benefit was not significantly attenuated by the presence of comorbidities.
Conclusion: Performance of angiography and coronary intervention after NSTEMI was associated with mortality benefit that persisted in the presence of both cardiac and non-cardiac comorbidities. Mortality benefit was seen across age groups and was similar for both sexes.
Statistics from Altmetric.com
Clinical guidelines recommend that patients with non-ST-segment elevation myocardial infarction (NSTEMI) undergo diagnostic coronary angiography soon after admission—USA within 24 h,1 Europe within 72 h.2 Meta-analyses of randomised trials have shown that an early invasive strategy confers mortality benefit compared with conservative or selective invasive approaches, particularly for higher-risk groups.3 4 However, there is debate about the interpretation of randomised trials5 and their validity in shaping care for patients in “the real world”6 7—for example, there is uncertainty as to whether women derive similar mortality benefit as men from an invasive approach.8
Provision of angiography is inconsistent. Patients admitted directly to hospitals with angiography facilities are more likely to receive angiography than those admitted elsewhere.9 10 11 Registry data show that patients with higher-risk profiles are least likely to be selected for angiography and intervention.12 13 While high-risk patients are more likely to undergo angiography in regions with higher “invasive procedure intensity”, this is not owing to a greater selection of patients based upon appropriateness or baseline risk.14
In this paper, we analysed data from the Myocardial Ischaemia National Audit Project (MINAP) to investigate the effect of age, gender and comorbidities on performance of angiography and intervention, and subsequent outcomes for patients with NSTEMI.
Methods
MINAP analyses data on patients admitted with acute coronary syndrome (ACS) from all hospitals in England and Wales. The project uses online data entry and provides hospitals with contemporary analysis of their performance and that of the aggregate for all hospitals.15 16 The dataset of 113 fields allows examination of the management of patients from onset of symptoms until discharge from hospital.17
We analysed records of admissions between July 2005 and December 2006 for patients having a final diagnosis of NSTEMI who were directly admitted to hospitals (n = 44) having interventional facilities. These hospitals were selected to ensure satisfactory completeness of data on provision of angiography, interventions and secondary prevention medication. We excluded patients transferred for investigation and treatment from hospitals without interventional facilities. The diagnosis of NSTEMI was assigned on the evidence of biomarker release and electrocardiographic changes that excluded ST-segment elevation.
Use of angiography and intervention were examined for three clinically relevant groups: the young—that is, <65 years, older patients aged from 65 to 79 years and the elderly, ⩾80 years. Mortality was tracked by the Office of National Statistics using a unique National Health Service number. Analyses of survival were based on patients leaving hospital alive after a first admission. Analyses of death included death of any cause within 180 days. Analyses of readmissions included all patients surviving to discharge, including those who died within 180 days. Asian ethnicity was used as a broad category for patients of Indian, Pakistani, Sri Lankan and Bangladeshi origin.
Statistical analyses
Continuous data were expressed as means, or as medians with interquartile range (IQR) for skewed distributions. Discrete or categorical data were summarised using frequencies and percentages. Continuous data were compared using the Mann–Whitney test and categorical data by χ2 test. A multivariate logistic regression analysis was used to investigate determinants for performance of angiography. Using Cox models that included the hospital to which patients were admitted as a random variable, we examined the effect of angiography on readmission and death with adjustments for other factors. Covariates included age (as a continuous variable), gender, ethnic origin (Caucasian or Asian), current smoking habit, use of coronary angiography, type of doctor providing initial care (cardiologist or generalist), admission area within hospital (cardiac or general medical facility) and a deprivation score obtained from the Index of Multiple Deprivation (IMD)18 (highest quartile (most deprived) against the remainder). The following comorbid conditions were included: previous angina, previous myocardial infarction (MI), treated heart failure, chronic obstructive pulmonary disease, chronic renal failure (creatinine >200 μmol/l), peripheral vascular disease, cerebrovascular disease, hypertension, diabetes and treated hyperlipidaemia. Drugs prescribed at discharge for secondary prevention treatment—angiotensin converting enzyme inhibitors or angiotensin receptor blockers, β blockers, aspirin, clopidogrel and statins—were also included. We adjusted for missing data by creating dummy variables.
To examine the possibility of confounding by indication—those who did not undergo coronary angiography being at too high a risk—we developed a propensity score (the probability of exposure to angiography) in a multivariable logistic regression model which included the following variables: age, sex, smoking status, IMD score, hyperlipidaemia, hypertension, diabetes, previous histories of angina, MI, percutaneous coronary intervention (PCI), heart failure, chronic obstructive pulmonary disease, chronic renal failure, peripheral vascular disease and cerebrovascular disease. The area under a receiver operating characteristic curve was 0.82 (95% confidence interval (CI) 0.81 to 0.83). The median (IQR) propensity score among those who received angiography was 0.74 (0.54 to 0.88), which was higher than 0.34 (0.024 to 0.54) in those who did not. We included the propensity score as a linear term in the adjusted Cox regression models.19 To further control such a confounding effect, we matched the propensity score for patients with and without angiography. The maximum difference in the propensity score allowed for a match was 0.015 for a sensitivity analysis. Gender differences in the effects were examined by interaction test with a two-sided p value.20
All analyses were performed in SPSS (Windows version 14.0; SPSS, Chicago, Illinois, USA) and SAS (Windows, release 8.02; SAS Institute, Cary, North Carolina, USA).
Results
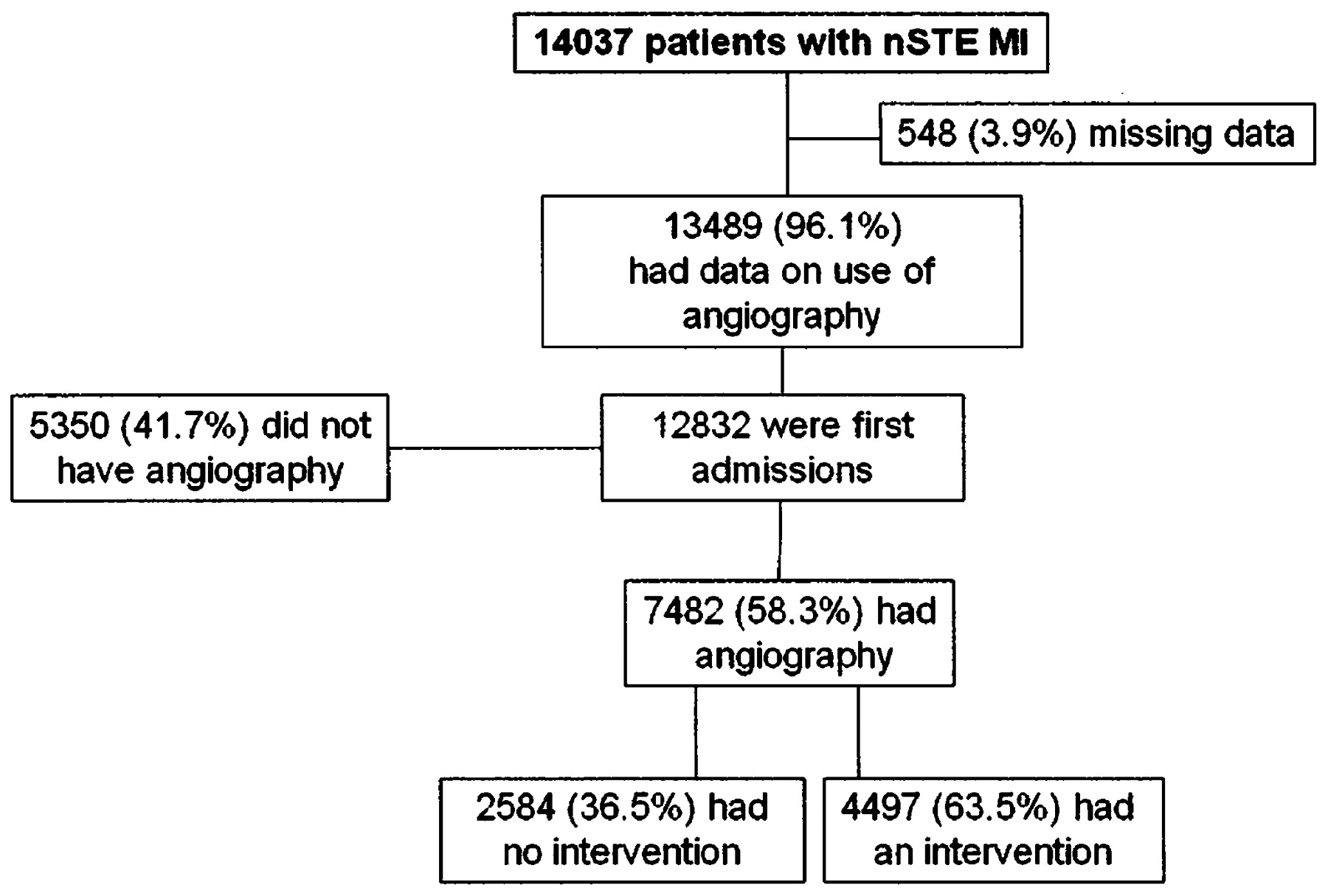
The records of 14 037 patients with a final diagnosis of NSTEMI admitted to 44 interventional hospitals between July 2005 and December 2006 were examined. Information on use of angiography was available for 13 489, of whom 12 832 were first admissions during this period. The median age was 74 years (IQR 63–82) and 62.2% were male. Men were younger than women: 70 years (60–79) against 78 years (69–85). A total of 6.2% patients had Asian ethnicity.
Use of angiography and intervention for first admissions
Of 12 832 first admissions, 7482 (58.3%) had angiography. Data on subsequent interventions were complete for 7081 (94.6%); 4006 (56.6%) had PCI—with 3631 (90.6%) performed during the index admission and 375 (9.4%) after discharge—491 (6.9%) had coronary artery bypass grafting and 2584 (36.5%) had no intervention (fig 1). The “indication” for angiography during admission was available for 7072 (95%). In 3447 (48.7%) angiography was performed for recurrent symptoms and 3625 (51.3%) had angiography as an elective procedure.
{kind=link}
Angiography and interventions for first admissions with non-ST-segment elevation myocardial infarction (nSTEMI). Four hundred and one records where angiography was performed did not have details of any subsequent intervention.
Angiography was performed less frequently with increasing age; 3238/3840 (84.3%) of those <65 years (median age 56.8 years, IQR 50.3–61.2) had angiography, 3380/5189 (65.1%) of those aged 65–79 years (median age 73.5 years, 69.5–76.8) and 864/3803 (22.7%) of those aged ⩾80 years (median age 85 years, 82.6–88.5). Angiography was performed less often for women, 46.7% against 65.2%, multiple adjusted odds ratio (OR) = 0.72, p<0.001. Table 1 shows the rates of comorbidity and other clinical factors, and the frequency with which angiography was performed in relation to these. Lower rates of angiography were associated with care by a generalist (OR = 0.75, p<0.001), admission to a non-cardiac facility (OR = 0.85, p = 0.003) and those in the highest quartile (most deprived) of IMD (OR = 0.76, p<0.001). A higher rate of angiography was associated with Asian ethnicity (OR = 1.61, p<0.001).
Rates of comorbidity and other factors with adjusted odds ratios for the performance of angiography for first admissions
The adjusted odds ratio for the performance of angiography was lower in the presence of most common comorbid conditions; chronic obstructive pulmonary disease (0.71, p<0.001), chronic renal failure (0.62, p<0.001), diabetes (0.76, p<0.001), peripheral vascular disease (0.72, p<0.001) and cerebrovascular disease (0.65, p<0.001), but was higher in the presence of hypertension (1.23, p<0.001) and treated hyperlipidaemia (1.67, p<0.001).
Performance of coronary interventions for those having angiography was lower with increasing age (table 2). Overall 4497 (33.3%) of 13 489 patients with NSTEMI had an intervention (with incomplete data in 401 cases).
Use of interventions for first admissions having angiography
Readmission within 180 days
Of 12 832 first admissions, death or discharge status was available for 12 154 (94.7%), of whom 993 (8.2%) died in hospital. Of the remaining 11 161, 573 (5.1%) were readmitted with possible ACS within 180 days—489 (85.3%) with further infarction (62 with ST-segment elevation), 74 (12.9%) had chest pain without biomarker release, and 10 had missing data. Of 573 readmissions, 484 were single and 89 were multiple (range 2–5).
Rates of readmission were compared between those who did not have angiography, those who had angiography without intervention and those who had a coronary intervention. Readmission rates were 244/4296 (5.7%) for those having no angiography, 101/2372 (4.3%) for those having angiography alone and 126/4128 (3.1%) for those having an intervention. There was no difference in the rate of readmission between those who had angiography alone and those not having angiography (multiple adjusted hazard ratio (HR) = 0.96, 95% CI 0.74 to 1.24). When coronary intervention was performed there was a reduction in the HR of readmission compared with those having no angiogram (HR = 0.73, 95% CI 0.56 to 0.95, p = 0.017). This was statistically significant for men alone (HR = 0.67, 95% CI 0.48 to 0.92, p = 0.014) and not for women (HR = 0.82, 95% CI 0.53 to 1.27, p = 0.382).
Death within 180 days of first admission
There was significant reduction in the adjusted HR of death within 180 days for those having angiography alone compared with those who did not (HR = 0.59, p<0.001), with a greater reduction for those having any intervention (HR = 0.34, p<0.001) (table 3). The reductions in HR of death were similar for men and women, with p>0.5 for gender comparisons for both angiography and intervention. Performance of angiography and intervention reduced the HR of death in the three age bands examined, although benefit was attenuated for patients older than 80 years (table 4).
Numbers, percentages and hazard ratios for 180-day mortality in patients without angiography, with angiography and with intervention
Impact of age on adjusted relative risk of death within 180 days
There was no difference in adjusted HR of death within 180 days between those having angiography for symptoms compared with those having an elective procedure: HR = 1.19, 95% CI 0.95 to 1.49.
A similar analysis was performed for patients matched by propensity score. With a criterion for the maximum difference in the propensity score allowing a match between patients with and without angiograph at 0.015, 5074 closely matched patients were identified for analysis (2537 in each group). Compared with those without angiography, the HR of death within 180 days was 0.55 (95% CI 0.44 to 0.69) for those having angiography alone and 0.36 (0.28 to 0.47) for those having an intervention. For these patients the HR in stratified analysis by gender and comorbidity was similar to that reported in tables 3–6 (data on request).
Impact of the presence of non-cardiac comorbidities on hazard ratio of death within 180 days
Impact of the presence of cardiac comorbidities on hazard ratio of death within 180 days
Impact of comorbidity on outcome after angiography and intervention
The impact of single and multiple comorbidities on outcome after angiography and intervention was examined after aggregating these into two groups—non-cardiac and cardiac. Group one included non-cardiac comorbidities associated with lower angiography rates (chronic obstructive pulmonary disease, chronic renal failure, peripheral vascular disease, diabetes and cerebrovascular disease). The second group comprised those with previous MI, angina, heart failure, PCI, or coronary surgery. The effect of the grouped comorbidities on the HR of death within 180 days was examined for each group. Equal weight was given to each factor. Other previously listed covariates not included within the group under examination were included in the model. Although non-cardiac and cardiac comorbidities were associated with higher unadjusted mortality, neither the presence of non-cardiac nor cardiac comorbidities significantly diminished the impact of the performance of angiography or coronary intervention on the HR of death with 180 days (tables 5 and 6).
Discussion
This study reflects clinical practice in hospitals with interventional facilities in England and Wales. The cohort examined was substantially older (median 74 years) and thus at higher risk, than subjects typically included in randomised trials of interventional treatments for NSTEMI. Angiography was performed for 58.3%, with about one half of this for symptoms of recurrent ischaemia, and 33% also had a coronary intervention. This is similar to a recent international registry study.12 We found that the improved outcome associated with angiography and intervention occurred irrespective of age (albeit attenuated in those older than 80 years), gender, deprivation status or the presence of either cardiac or non-cardiac comorbidity. However, the presence of most comorbidities, admission under the care of non-cardiologists, and (independently) to non-cardiac facilities, was associated with lower angiography rates. In common with others we also found angiography was less likely to be offered to older subjects and women.21 22
Selection for angiography
Risk-averse selection for angiography has been reported from other contemporary registries,12 13 but our study extends this finding to include other commonly encountered comorbidities that carry adverse prognostic implications such as diabetes, and chronic obstructive pulmonary disease. Underuse of angiography in the presence of comorbidities may reflect a concern that angiography and subsequent interventions are of less benefit in the presence of comorbidities. We show that while both non-cardiac and cardiac comorbidities were associated with higher crude mortality, the reduced HR of death associated with angiography and intervention is not significantly attenuated in the presence of either.
Age
Older patients were less likely to be offered angiography. This may reflect an unwillingness to exercise a routine (rather than selective) interventional strategy in the elderly because of increased adverse effects of an interventional approach in, and under-representation of, old people in the trials upon which the recommended strategy is based.23 Additionally, some older patients may be less willing to undergo invasive procedures.24 The reduced HR of death associated with an invasive approach in the elderly reported here supports the wider use of angiography in older patients. We speculate that the attenuated benefit of angiography and intervention in the elderly compared with younger patients may reflect the fact that death rates were based on all-cause mortality.
Gender
After multivariate adjustment, women had a reduced OR of having angiography. This may reflect uncertainty about whether women benefit from a routine invasive approach to the same extent as men25 26 and also knowledge that women presenting with ACS are less likely to have significant coronary disease.27 Although a recent meta-analysis showed that an invasive strategy is associated with improved outcomes for women based on composite end points (death, recurrent MI or further ACS),8 this study demonstrates that angiography and intervention are associated with a reduced HR for the single end point of death within 180 days for women.
Readmission and death
Readmission within 180 days occurred in 5.1%, of whom the majority (85.3%) had further infarction. Angiography followed by intervention (but not angiography alone) was associated with a reduced HR of readmission—implying a reduction in the risk of further infarction. This was only significant for men and was not significant for women.
Performance of angiography reduced the HR of death within 180 days by 41%, and this was reduced further by performance of any intervention (overall reduction 66%). The effects of angiography alone, and the additional effect of intervention were similar in men and women, and were significant in each age group (<65, 65–79 and ⩾80 years). The mortality benefit seen here is larger than that seen in earlier studies comparing conservative with interventional management for NSTEMI.1 2 This may reflect inclusion of younger cohorts, at lower risk, in randomised trials, and the frequent use of (cross-over to) invasive treatments in those allocated to conservative treatments in such trials. Clearly, in our observational study mortality in the group not having angiography was high, reflecting the adverse prognostic characteristics of this group. They frequently had cardiac and non-cardiac comorbidities, were more likely to be in the highest quartile of the index of multiple deprivation, were less likely to be admitted to a cardiac care unit and less likely to be under the care of a cardiologist; all factors associated with adverse outcomes. By contrast, those having angiography had a lower-risk profile. This tends to exaggerate mortality benefit from angiography alone, which as an investigation rather than a treatment is unlikely to have direct prognostic value. However, the possibility that the additional information obtained by performance of angiography, compared with non-invasive testing such as exercise testing, has mortality benefit, cannot be excluded. In other words, recognition that an intervention is not required, and that the patient is lower risk, is more accurate in the presence of a coronary angiogram.
Study limitations
In observational studies, multivariate analysis may not account for all the baseline differences among individual patients with and without angiography. However, adjustments included the IMD score, which is closely related to a health score (correlation coefficient in this database 0.83, p<0.001) that describes health status, including measures of acute morbidity.28 A propensity score was also used to further adjust for biases related to covariates associated with treatment assignments, without substantial changes to the results. Although our primary analyses did not take account of severity of infarction, further adjustment for individual troponin levels, did not alter the results substantially. (Analysis available on request.)
Conclusions
The performance of angiography after NSTEMI was associated with mortality benefit across age groups, without significant gender differences and in the presence of both cardiac and non-cardiac comorbidities. The likelihood of receiving a coronary angiogram after admission with NSTEMI was affected by multiple factors. These include the presence of comorbidities, and patterns of clinical management that prevented full access to cardiac expertise.
REFERENCES
Footnotes
Funding MINAP is funded by the Healthcare Quality Improvement Partnership.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.