Article Text

Abstract
Objective: To investigate the secular trend in survival after a new diagnosis of heart failure in the UK population.
Design and Setting: Comparison of all-cause mortality in the 6 months after diagnosis of heart failure in population-based studies in the south east of England in 2004–5 (Hillingdon–Hastings Study) and 1995–7 (Hillingdon–Bromley Studies).
Participants: 396 patients in the 2004–5 cohort and 552 patients in the 1995–7 cohort with incident (new) heart failure.
Main Outcome Measures: All-cause mortality.
Results: All-cause mortality rates were 6% (95% CI 3% to 8%) at 1 month, 11% (8% to 14%) at 3 months and 14% (11% to 18%) at 6 months in the 2004–5 cohort compared with 16% (13% to 20%), 22% (19% to 25%) and 26% (22% to 29%), respectively, in the 1995–7 cohort (difference between the two cohorts, p<0.001). The difference in survival was not explained by any difference in the demographics or severity of heart failure at presentation. There was a difference at baseline and thereafter in the use of neurohormonal antagonists (β-blockers and angiotensin-converting enzyme inhibitors).
Conclusions: Although early mortality remains high among patients with newly diagnosed heart failure in the UK general population, there is strong evidence of a marked improvement in survival from 1995–7 to 2004–5, perhaps partly explained by an increased usage of neurohormonal antagonists.
Statistics from Altmetric.com
Heart failure is a global healthcare problem. In the UK, approximately 900 000 people live with definite or probable heart failure,1 2 and a further 60 000 people develop incident (new) heart failure annually.3 4 The syndrome affects at least 10 million patients across Europe5 and 5 million patients in the USA.6
The prognosis after a new diagnosis of heart failure in the general population is poor, with a particularly high risk of mortality in the first few months after diagnosis.7 8 9
Over the past 20 years, several large randomised controlled trials of neurohormonal antagonists including angiotensin-converting enzyme (ACE) inhibitors, β-blockers and aldosterone antagonists5 and device therapies10 11 12 have demonstrated improved survival in patients with heart failure. It is hoped that the increasing use of such therapies will improve survival for patients with heart failure in the general population.
Referral series13 14 and hospital registry data15 16 17 18 have reported improved survival. However, these reports may not apply to the general population of heart failure patients due to potential selection bias in such studies and changing thresholds for admission to hospital.
Population-based data on changes in heart failure survival from Europe are lacking. US population-based data on the temporal trend in survival for incident heart failure initially demonstrated no change in survival rates up until the early 1990s,7 19 but more recent reports have suggested improving long-term survival but with a continuing high early mortality rate.20 21 22
We report the secular trend in early survival for incident heart failure in population-based studies based in the south east of England.
Methods
We compared survival data of two combined cohorts of incident heart failure identified in two study periods: 1995–7 and 2004–5. The 1995–7 cohorts (Hillingdon, West London and Bromley, south-east London) have been described previously.8 9 The 2004–5 cohorts (Hillingdon, West London and Hastings and Rother, East Sussex, south-east England) employed similar methodology to the 1995–7 studies.
Study population and identification of cases
The 1995–7 cohorts consisted of 552 incident cases of heart failure identified from a combined population of 443 000.8 9 Study design, case ascertainment and patient characterisation have been described previously.3 4
The 2004–5 study population consisted of two urban populations in the UK. All inpatient care and the majority of outpatient care for the respective study populations are provided by the Hillingdon Hospital and the Conquest Hospital. The populations consisted of 243 006 in Hillingdon and 170 457 in Hastings and Rother, East Sussex, UK. The 2004–5 cohort consisted of 396 incident cases identified from the combined population of 413 463, using similar methodology to the 1995–7 studies.3 4
Potential cases of heart failure arising in the study populations were identified across all studies by daily surveillance of all acute medical hospital admissions, referral by general practitioners of all suspected new cases of heart failure to a general cardiology or heart failure clinic, inpatient referral of suspected new cases of heart failure to the cardiology team and scrutiny of echocardiography lists. Case ascertainment using this methodology was examined in the Hillingdon 1995–6 heart failure study, and was found to be 90%.3
Case definition
A clinical diagnosis of heart failure was defined according to the European Society of Cardiology criteria at the time of the studies.23 To meet the case definition of heart failure (“definite” cases), patients were required to have symptoms of heart failure and the presence of an underlying abnormality of cardiac structure or function. In cases in which the diagnosis was in doubt (“possible” cases), a favourable response to treatment directed towards heart failure was taken as confirmation of diagnosis.
All data regarding “possible” cases and a random sample of “definite” cases were presented to a panel of three cardiologists (MRC, TM and GS) to determine, on the basis of a majority decision, whether the case definition had been met and to classify the aetiology of heart failure. All patients’ medical notes and details from primary care were checked to ensure that only new (incident) cases of heart failure were included in the study.
Follow-up
The date of death was ascertained by “flagging” each patient’s record at the Office of National Statistics using their unique National Health Service number. Follow-up for death was 100% complete for both study periods.
Of the 398 patients recruited in the 2004–5 cohort, two patients (<1%) withdrew from the study due to personal reasons and their data were excluded from the analysis.
Data analysis
Continuous variables with a normal distribution were described using mean and standard deviation (SD). If the distribution was not normal, median and 90% range were used as descriptors. Comparisons of variables with a normal distribution were by Student’s t test, and for non-normal distributed variables that could not be transformed to a normal distribution, by log-rank test. Comparisons of proportions were performed using a χ2 test or Fisher’s exact test. Survival was estimated using the Kaplan–Meier method. The estimated survival probabilities and 95% confidence intervals at 1, 3 and 6 months were calculated. Differences in overall survival were analysed by log-rank test.
The association between clinical and investigative findings and all-cause mortality in the 2004–5 cohort were examined by Cox proportional hazards regression modelling.24 All covariates associated with all-cause mortality in the Cox univariate regression (p<0.15) were then entered into a multivariable Cox regression analysis. Difference in survival between the cohorts was examined by Cox regression, with and without adjustment for variables associated with survival.
Results
Incidence of heart failure
The overall incidence of heart failure, in the 2004–5 study period was approximately 1 per 1000 population per year. The incidence increased with rising age from 0.04 cases per 1000 population per year in those aged 20–34 years to 3.71 in those aged over 85 years. The reported incidence in the 1995–7 studies was similar at 1.3 per 1000 population per year in the Hillingdon Study and 0.9 cases per 1000 population per year in the Bromley Study.3 4
Baseline characteristics
Table 1 gives the baseline demographics and clinical features of the incident heart failure cases identified in the 1995–7 and 2004–5 study cohorts.
Baseline patient characteristics
The 1995–7 and the 2004–5 cohorts were similar by age, body mass index, serum creatinine concentration and ECG QRS duration.
The 2004–5 cohort consisted of significantly more men (p = 0.02), more inpatients at the time of diagnosis (p<0.001) and more cases with a history of myocardial infarction (p<0.001), hypertension (p<0.001) and chronic obstructive pulmonary disease (p<0.001). There were significantly more cases of heart failure due to acute myocardial infarction (p = 0.01). The 2004–5 cohort had significantly lower baseline systolic (p<0.001) and diastolic (p<0.001) blood pressure, lower serum sodium concentration (p = 0.001) and lower haemoglobin (p<0.001). There was a trend to more patients with severe left ventricular dysfunction (p = 0.089) but slightly fewer presenting with symptoms at rest (New York Heart Association (NYHA) class IV) (p = 0.02).
The use of background cardiovascular drug therapy was statistically significantly higher in the 2004–5 cohort; also, 39% were taking an ACE inhibitor or angiotensin receptor blocker (ARB) before the diagnosis of heart failure, compared with 3% in the 1995–7 cohort (p<0.001).
Survival
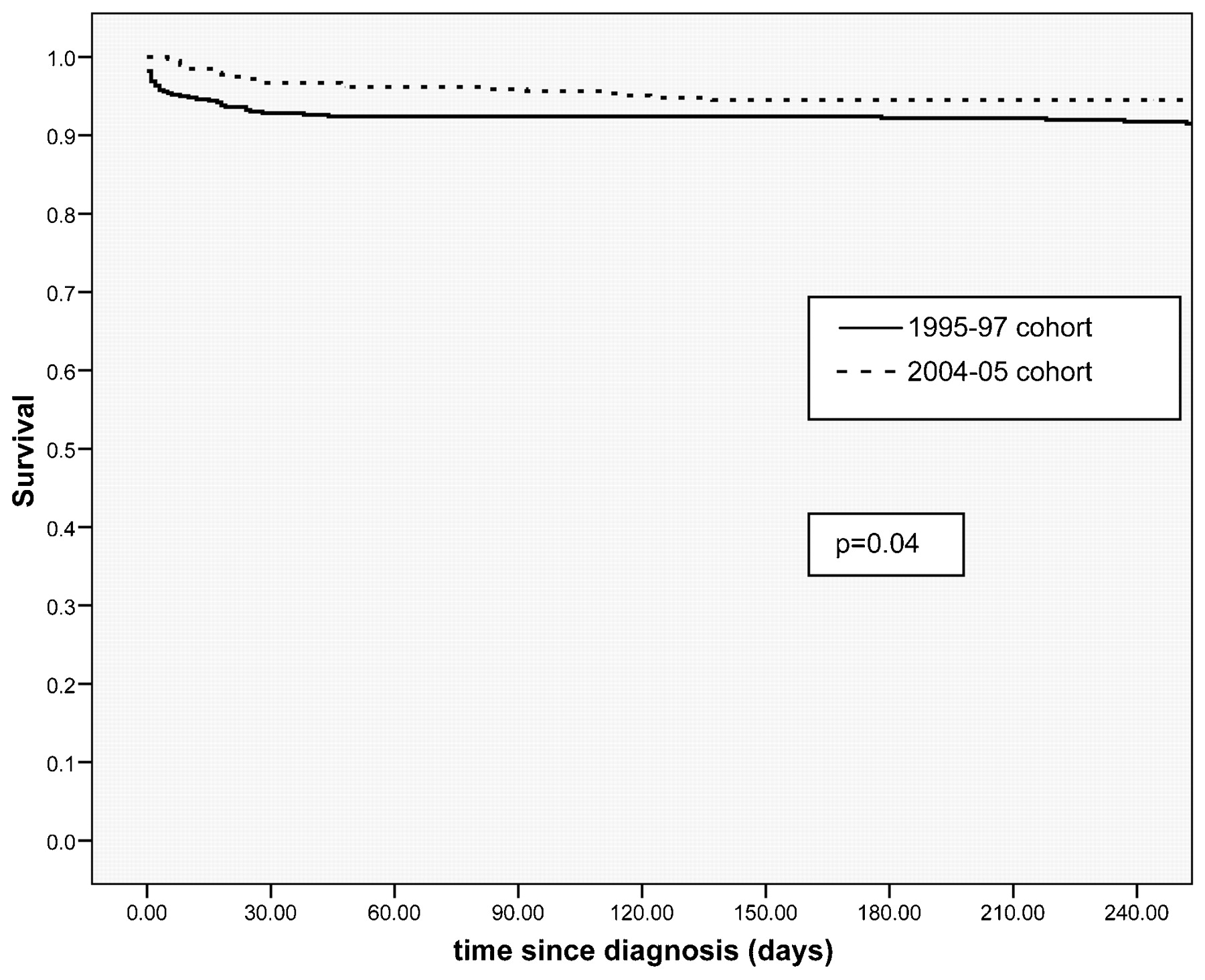
Of the 396 patients with incident heart failure identified in the 2004–5 cohort, 56 patients died during the first 6 months after diagnosis. All-cause mortality rates were 6% (95% CI 3% to 8%] at 1 month, 11% (8% to 14%] at 3 months and 14% (11% to 18%) at 6 months.
Of the 552 patients identified in the 1995–7 cohort, 141 died in the first 6 months after diagnosis. All-cause mortality rates were 16% (13% to 20%) at 1 month, 22% (19% to 25%) at 3 months and 26% (22% to 29%) at 6 months.
Overall survival was statistically significantly better in the 2004–5 cohort compared with the 1995–7 cohort (p<0.001; fig 1), with a hazard ratio (HR) of 0.41 (0.31 to 0.55) for the 2004–5 cohort compared with the 1995–7 cohort. Table 2 gives the age-adjusted standardised mortality ratios. The observed improvement in overall survival remained statistically significant (and numerically little changed) after adjustment for age, gender, racial origin, place of assessment (inpatient or outpatient clinic), serum sodium, serum urea, haemoglobin, systolic blood pressure, NYHA class (IV versus other), left ventricular function (severe dysfunction versus other) at baseline (HR 0.39; 95% CI 0.28 to 0.53; table 3). The improved mortality in the more recent cohort remained after adjustment for the difference in the proportion of patients on background ACE inhibitor treatment in the two cohorts, although the difference in survival was slightly less marked (HR 0.52; 95% CI 0.38 to 0.70).

Improvement in survival of incident cases of heart failure in the two cohorts.
Standardised age-adjusted mortality ratios for the 1995–7 and 2004–5 cohorts
Mortality hazard ratio for 1995–7 and 2004–5 cohorts, with 1995–7 as baseline, and adjusted for age, gender and other factors associated with mortality
Treatment with an ACE inhibitor in the 2004–5 cohort was significantly associated with reduced all-cause mortality on univariable analysis (HR 0.43; 95% CI 0.25 to 0.75; p = 0.003) but not on multivariable analysis. Treatment with a β-blocker in the 2004–5 cohort was associated with a strong trend for reduced all-cause mortality on univariable analysis (HR 0.50; 95% CI 0.25 to 1.0; p = 0.051), but not on multivariable analysis.
Survival after a new diagnosis of heart failure due to acute myocardial infarction was significantly better in the 2004–5 cohort (n = 95) compared with the 1995–7 cohort (n = 96; 6-month mortality: 6% (4 to 6) vs 8% (6 to 10); p = 0.048; fig 2).

{kind=link}
{kind=link}
Improvement in survival of incident cases of heart failure due to acute myocardial infarction in the two cohorts.
Predictors of all-cause mortality
On multivariable Cox regression analysis (table 4), five baseline variables were independently associated with all-cause mortality in the 2004–5 cohort: increasing age of patients; lower serum sodium and higher serum urea (⩾10 mmol/l vs rest); longer QRS duration (⩾100 ms vs rest) and lower systolic blood pressure (<115 mm Hg vs rest).
Cox multivariable regression analysis for all-cause mortality in the 2004–5 cohort
Discussion
This study provides the first European population data on the improved prognosis of heart failure during the early period after a new diagnosis, confirming reports from hospitalised series.15 16 17 18 Although mortality in the early period after diagnosis is high, there has been a significant improvement in the rates of early survival over the past decade. The overall improvement in survival occurs immediately and persists throughout the first 6 months after diagnosis.
The observed improvement in survival between 1995–7 and 2004–5 cannot be explained by differences in research methodologies, as they were similar in both studies. The two cohorts were similar with respect to age, body mass index, serum creatinine and ECG QRS duration but there were certain baseline differences. The 2004–5 cohort consisted of a higher proportion of men, more diagnosed as inpatients rather in the outpatient clinic, a higher proportion with heart failure due to acute myocardial infarction, and a lower serum sodium concentration and blood pressure at the time of presentation compared with 1995–7 (table 1).
Although there is some debate about whether lower socioeconomic status within a population is associated with a poorer prognosis for patients with heart failure,16 25 this cannot explain the difference in survival between the two cohorts, as the second cohort (with a better survival) included a more deprived population (Hastings) than the first cohort (Bromley).26 Hillingdon district was included in both cohorts.
Baseline differences would suggest that the 2004–5 cohort may have been a higher-risk population, with greater expected mortality than the 1995–7 cohort. However, the opposite was found: overall survival was significantly better in the later time period.
The reasons for the observed improvement in survival are likely to be multifactorial. The diagnosis of heart failure may occur earlier, due to increased primary care physician awareness of the diagnosis and better access to diagnostic tests such as echocardiography, so called “lead time bias”. Milder cases of heart failure may be diagnosed, giving rise to “spectrum bias”. Our data show a slightly lower proportion presenting with symptoms at rest (NYHA class IV) (59% in 1995–7 cohort vs 52% in 2004–5 cohort (p = 0.02); table 1). The overall incidence of heart failure is almost identical in the two time periods, similar to data from most but not all population series from the USA.19 20 21 27
The general prescription of ACE inhibitors has increased greatly in the at-risk population of those with hypertension, coronary artery disease and diabetes mellitus.28 We report a substantially increased proportion of patients presenting for the first time with heart failure on such agents (39% in 2004–5 compared with 3% in 1995–7; p<0.001)—this may improve the natural history of heart failure. However, the observed improvement in survival persisted after adjustment for background ACE inhibitor therapy.
In both study periods, patients were not treated according to any specific protocol. Management was at the discretion of the physician caring for the patient during hospital admission or clinic attendance. At the time of leaving hospital (either inpatient discharge/death or outpatient) 79% of patients were taking an ACE inhibitor or ARB in the 2004–5 cohort, compared with only 65% of patients surviving more than 30 days in the 1995–7 cohort.8
The use of early β-blockade is also considerably higher than a decade ago, with almost one-third prescribed a drug in this class before inpatient discharge or outpatient clinic attendance.
The use of ACE inhibitors in the 2004–5 cohort compared favourably with audit data from hospital practice in England and Wales in 2005.29 Although not reported from the original cohort in 1995–7, very few cases would have been on a β-blocker, as this preceded the publication of clinical trials demonstrating survival benefit with the use of β-blockers in heart failure. Although the rates of prescription of drugs known to improve prognosis in heart failure is higher than in 1995–7, it remains suboptimal, as it does across Europe.29 30 31
Clinical trials have shown mortality benefits from the use of cardiac resynchronisation therapy10 32 and implantable defibrillators12 33 in selected patients with chronic heart failure. The use of such devices in the 2004–5 cohort was low (only four patients (<1%) within the first 6 months of diagnosis), reflecting the low UK implant rate at the time of the study. The introduction of device therapy cannot, therefore, account for the overall improvement in survival.
The single most frequent cause of incident heart failure in 2004–5 was acute myocardial infarction. Our data suggest a significantly higher frequency of acute myocardial infarction as a cause of incident heart failure in this cohort by comparison with the earlier cohort. However, this difference is likely to be due to increased sensitivity for the diagnosis of myocardial infarction due to changing definitions of acute myocardial infarction over the study time period and the use of biomarkers of myocardial necrosis such as troponin.34
The diagnosis and management of acute coronary disease, with improved rates of early thrombolysis35 and increasing use of primary angioplasty leading to increased preservation of myocardium, may also be partly responsible for the observed improvement in survival. Although based on small numbers, survival in the first 6 months after a new diagnosis of heart failure due to a myocardial infarction has improved over the past decade in our cohorts.
Other limitations of the study
We cannot comment on the secular trend in mortality in incident heart failure in other areas of the UK, as our studies were confined to the south east of England, albeit from areas with a wide range of socioeconomic and ethnic composition. Improvements reported in hospitalisation series from the UK suggest our findings may apply more broadly.15 16 18 Whether the early improvement in survival is maintained will be reported at a later date, when longer follow-up data become available. The improvement may also be greater in populations with a higher penetration of neurohormonal antagonists and cardiac resynchronisation therapy or implantable defibrillators.
Conclusions
We provide population-based data on well-characterised incident cases of heart failure in the UK, suggesting that although mortality remains high in the early period after diagnosis, there has been a statistically and clinically highly significant improvement in survival over the past decade. This could be related, at least partly, to the increased use of neurohormonal antagonists such as ACE inhibitors and β-blockers, and perhaps a more aggressive approach to the management of acute coronary artery disease.
Despite these findings, the use of β-blockers and aldosterone antagonist therapy remains suboptimal. The focus of heart failure management during this early high-risk period should be the initiation and up-titration of neurohormonal antagonists known to retard the progression of heart failure.
Acknowledgments
The authors are grateful to Tina Chan and Lorraine Dunne for collection of medical data.
REFERENCES
Footnotes
Funding This work was supported by British Heart Foundation Project grant PG/03/097 and by the Royal Brompton and Harefield Trustees.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Ethics approval The Hillingdon Hospital study site was granted ethical approval by the Hillingdon Local Research Ethics Committee on 11 November 2003 (ref no 1268). The Conquest Hospital study site was given ethical approval by the East Sussex Local Research Ethics Committee on 18 November 2003 (ref no ES 03/36).
Patient consent Obtained.
Research was conducted independently from the funders. Professor M R Cowie was the guarantor.