Article Text

Abstract
Background The concept of non-atherosclerotic coronary artery pathology in sudden cardiac death (SCD) has not been given the attention it deserves.
Objective To determine the incidence of non-atherosclerotic coronary artery pathology in SCD and raise awareness among cardiologists and pathologists alike.
Design Retrospective non-case-controlled analysis.
Setting Cardiac pathology centre at the National Heart and Lung Institute and Royal Brompton Hospital.
Subjects Between 1994 and 2008, the hearts of 1647 people undergoing SCD were referred for pathological assessment to ascertain the precise aetiology of SCD.
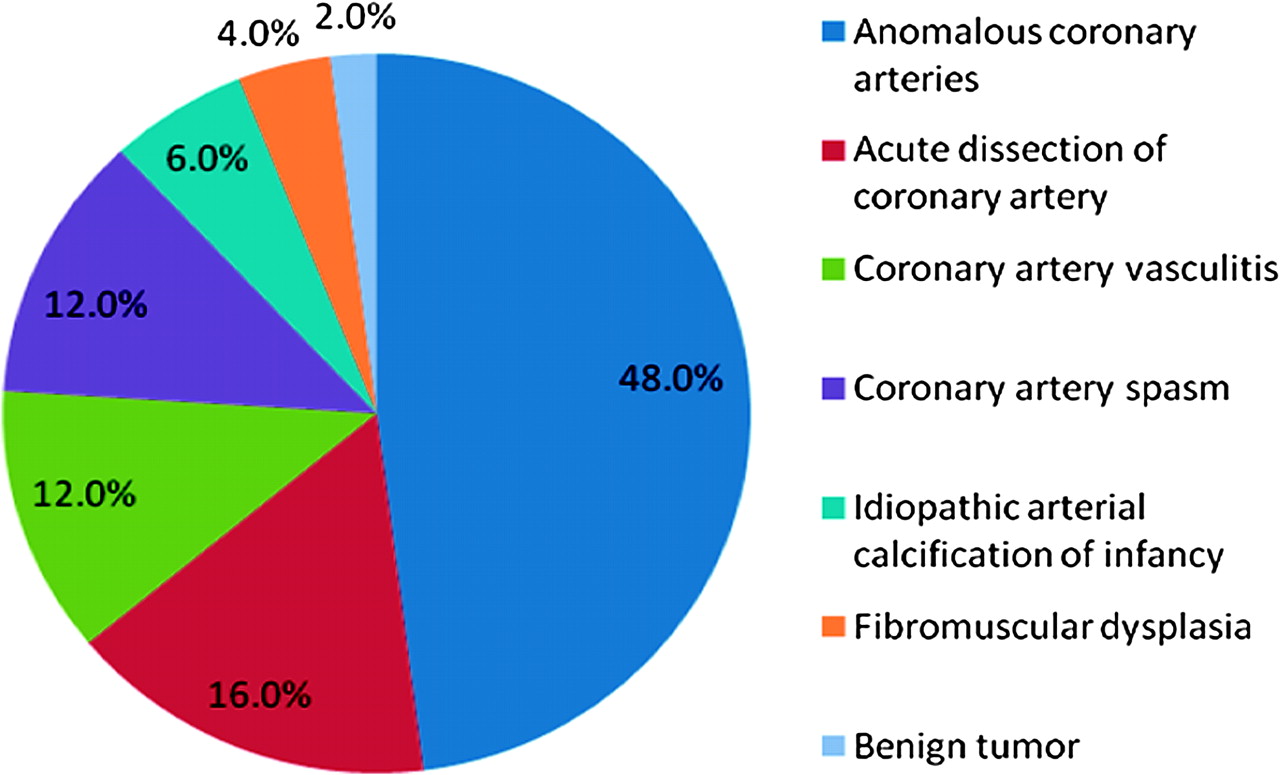
Results Fifty (3.0%) of the 1647 cases of SCD were associated with non-atherosclerotic coronary pathology (31 male subjects (62%) and 19 female subjects (38%, age range (8 weeks–71 years)). Twenty four of the 50 cases had anomalous coronary arteries (48%); eight cases had coronary artery dissection (16%); six cases had coronary artery vasculitis (12%); six cases had coronary artery spasm (12%); three cases had idiopathic arterial calcification of infancy (6%); two cases had fibromuscular dysplasia (4%) and one case had a benign tumour occluding the left coronary ostium (2%). Only 20 of the 50 patients (40%) were documented to have experienced cardiac symptoms such as syncope, chest pain on exertion or breathlessness before their SCD. Twelve of the patients (24%) died during or immediately after physical exertion.
Conclusion Non-atherosclerotic coronary disease is associated with sudden death in all age groups, particularly younger, male patients. Cardiologists need to be aware of these entities and investigate any patient who has cardiac symptoms especially with exertion.
- Anomalous coronary artery
- sudden cardiac death
- coronary artery vasculitis
- fibromuscular dysplasia
- idiopathic calcification of infancy
- syncope
- ventricular fibrillation
Statistics from Altmetric.com
- Anomalous coronary artery
- sudden cardiac death
- coronary artery vasculitis
- fibromuscular dysplasia
- idiopathic calcification of infancy
- syncope
- ventricular fibrillation
Introduction
Sudden cardiac death (SCD) has gained prominence in recent years.1 It is defined as an unexpected death due to known or unknown cardiac causes and generally occurs within 1 h of the onset of symptoms.2 A task force of the European Society of Cardiology has indicated that the incidence of SCD ranges from 36 to 128 deaths/100 000 population/year, the large variation being due to the method of reporting.3 Coronary artery atherosclerosis accounts for most cases, ranging from 59% to 86% of SCD.4 Non-atherosclerotic coronary artery causes of SCD do occur but are considered to be rare with individual cardiologists having little experience of them. This paper is the largest series to date in the UK that reviews a wide range of non-atherosclerotic coronary disease associated with SCD. Our aim is to raise awareness of non-atherosclerotic coronary disease as a possible cause of SCD so that more cases are identified by cardiologists during life.
Materials and methods
The National Heart and Lung Institute and Royal Brompton Hospital acts as a specialist tertiary cardiac pathology centre for SCD in the UK. We have established a database of 1647 hearts between 1994 and 2008 (approximately 50% of the cases aged 35 years and 50% >35 years). Histological sections from the coronary arteries, myocardium, a single myocardial transverse section of the ventricles, or whole hearts are referred by coroners and pathologists throughout the UK with permission obtained from the next of kin. They are often referred to our centre for further evaluation when the findings are ambiguous; when rare entities are suspected; or when no clear cause of death can be established by the local pathologist. The age of the deceased does not bias referral patterns to our centre.
We sought to define retrospectively the premortem clinical and postmortem histopathological findings in each case. The patient's age, sex, circumstances of death, antecedent cardiac symptoms, past medical history and a family history of cardiac disease (when available) were obtained from the referring pathologist or coroner. All patients included in this study underwent a toxicology screen as part of the coroner's mandate since all deaths were sudden and unexpected. For the purpose of the study cases of coronary artery disease (coronary artery stenosis, with or without acute or old myocardial infarction or fibrosis) and congenital cardiac disease were excluded.
Pathological analysis of all hearts using defined protocols was performed by the senior author (MNS) with the consent of the coroner and family of the deceased.5 The heart tissue was analysed both macroscopically and microscopically to identify non-atherosclerotic coronary disease and any resultant acute or chronic ischaemic damage. Histological criteria for ischaemic damage in the heart included acute changes with contraction band necrosis, hypercontracted myocytes and myocyte necrosis with surrounding acute neutrophilic inflammation. Chronic changes included granulation tissue and replacement fibrosis in the myocardium.6–8 Myocardial fibrosis was highlighted after staining with haematoxylin and eosin (H&E) as well as elastic Van Gieson stain. To be considered significant, the fibrosis had to involve at least 20% of the myocardial section supplied by the abnormal coronary artery on naked eye examination. Other causes of fibrosis such as coronary artery disease, coronary thrombosis/emboli, myocarditis, hypertrophic cardiomyopathy and arrhythmogenic right ventricular dysplasia were excluded on both macroscopic and microscopic examination with reference to specific criteria.5 Dilated cardiomyopathy (DCM) was also excluded as a cause of fibrosis. Pathological criteria for dilated cardiomyopathy were defined by the senior author (MNS) and included a heart weighing >500 g with a thin wall measuring <10 mm, a chamber dimension >35 mm and normal coronary arteries. After exclusion of the above cardiac diseases, we presumed that the non-atherosclerotic coronary pathology was responsible for the ventricular fibrosis we identified. Previous studies in which the author (MNS) was involved indicate that this fibrosis would be detected by cardiovascular magnetic resonance and delayed gadolinium enhancement.9 Results were categorised into (a) normal hearts or (b) ischaemic hearts (acute and/or chronic).
This study was approved by the ethics committee of the Royal Brompton Hospital, reference number 01–112, informed consent from relatives was obtained in all cases. This study complies with the requirements of the Human Tissue Act 2004. Incidentally, after the introduction of the act referral volumes to the CRY centre increased.
Results
Non-atherosclerotic coronary artery pathology was associated with SCD in 50 cases giving an incidence of 3.0% of the total database of 1647 cases (table 1). Thirty-one of the affected individuals (62%) were male and 19 were female (38%), age range varied from as young as 8 weeks to 71 years, average age of 32. Twenty-two of the patients (44%) in this study were in the >35 age group.
Relative frequencies of non-atherosclerotic coronary pathology as a cause of sudden cardiac death (SCD) in our series
The circumstances at the time of death were varied. In 12 cases (24%) SCD occurred during or immediately after physical exertion, eight of which were sport related (football/rugby/cross country) and five occurred after a stressful event (post-fight/attack). In 12 patients SCD occurred at rest.
Clinical data were available for 47 of the 50 patients. Cardiac symptoms (chest pain, syncope, breathlessness) were documented to have occurred in 20 patients (40%). The timing of these symptoms in relation to the SCD is recorded in table 2. In the remaining 27 cases it was stated that there was no significant past medical history. Toxicology screens in all patients in this study were negative.
Age and gender distribution and symptom documentation for each cause of sudden cardiac death (SCD)
Anomalous coronary arteries were observed in 24 of the 50 cases (48%) of non-atherosclerotic coronary disease and accounted for 1.5% of the total number of SCDs in our database (table 1, figure 1). The age and gender distribution of this group are documented in table 2. Notably, nine patients were over 35 years and 12 patients (50%) were exercising immediately before their death.

Pie chart to show the non-atherosclerotic coronary causes of sudden cardiac death and their relative frequencies.
The cases of anomalous coronary arteries were classified into three groups:(i) anomalous coronary origin/high take off, (ii) coronary artery ostial stenosis/atresia and (iii) myocardial bridging.
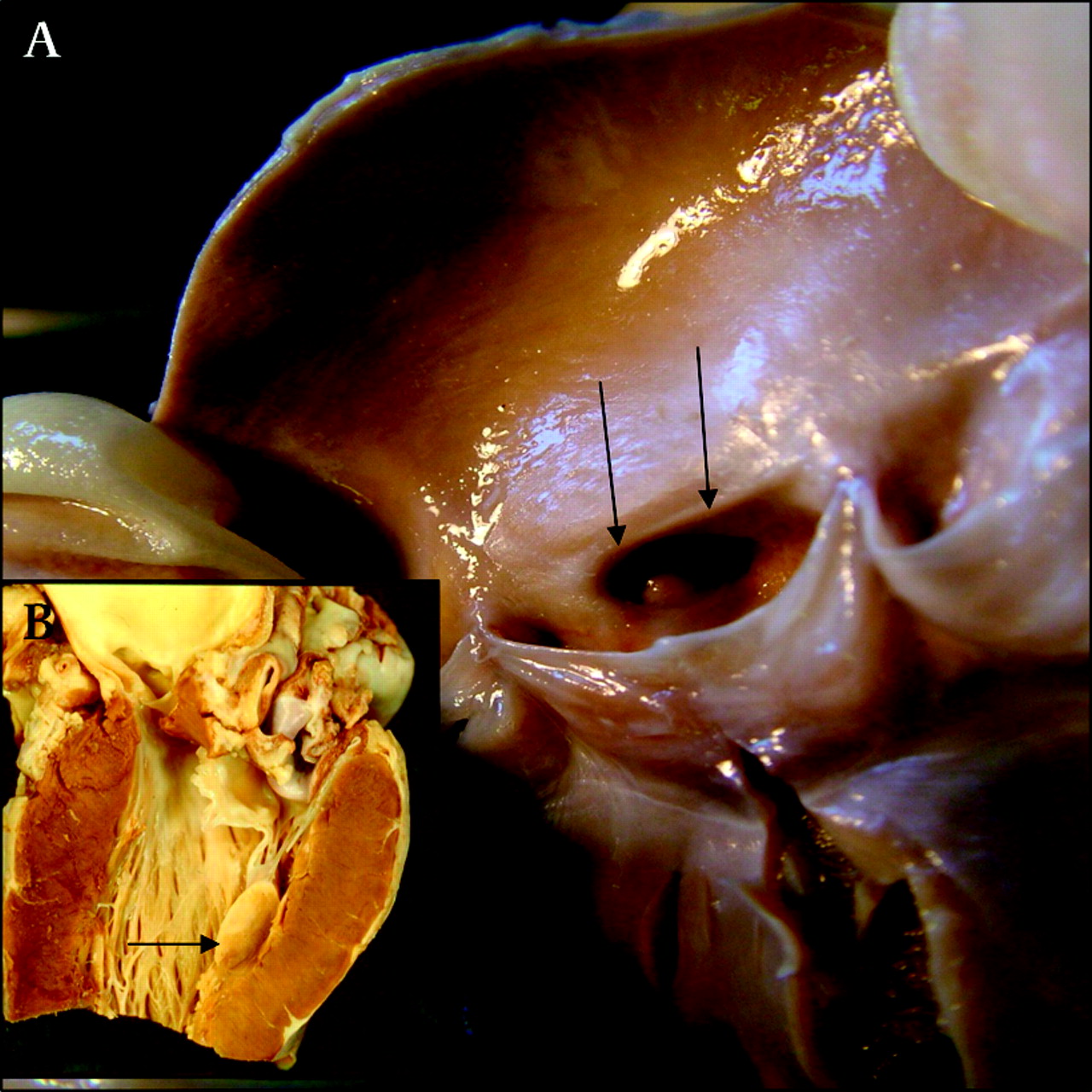
An anomalous coronary artery origin was found in 13 cases, equating to 0.8% of all-cause SCDs. Five cases had an anomalous left coronary artery (LCA) arising from the right coronary sinus (figure 2) and seven cases had an anomalous right coronary artery (RCA) arising from the left coronary sinus. In the remaining case the origin of the RCA was 15 mm above the sinotubular junction (high take off) (figure 3). Eleven of the 13 anomalous arteries had an interarterial course between the pulmonary artery and the aorta. In four of the 13 cases the affected artery was found to have an aortic intramural course (traversing within the aortic wall) with a slit-like lumen.

Cardiac morphology of an 11 year old boy who died suddenly after a cross-country run. (A) Note that both coronary artery ostia arise in the right aortic sinus (arrows). (B) Papillary muscle scarring in the left ventricle resulting from the coronary anomaly (arrow).

Cardiac morphology of a 44 year old man who died suddenly at rest. The aortic root shows high take off of the right coronary artery, 15 mm above the sinotubular junction (arrow).
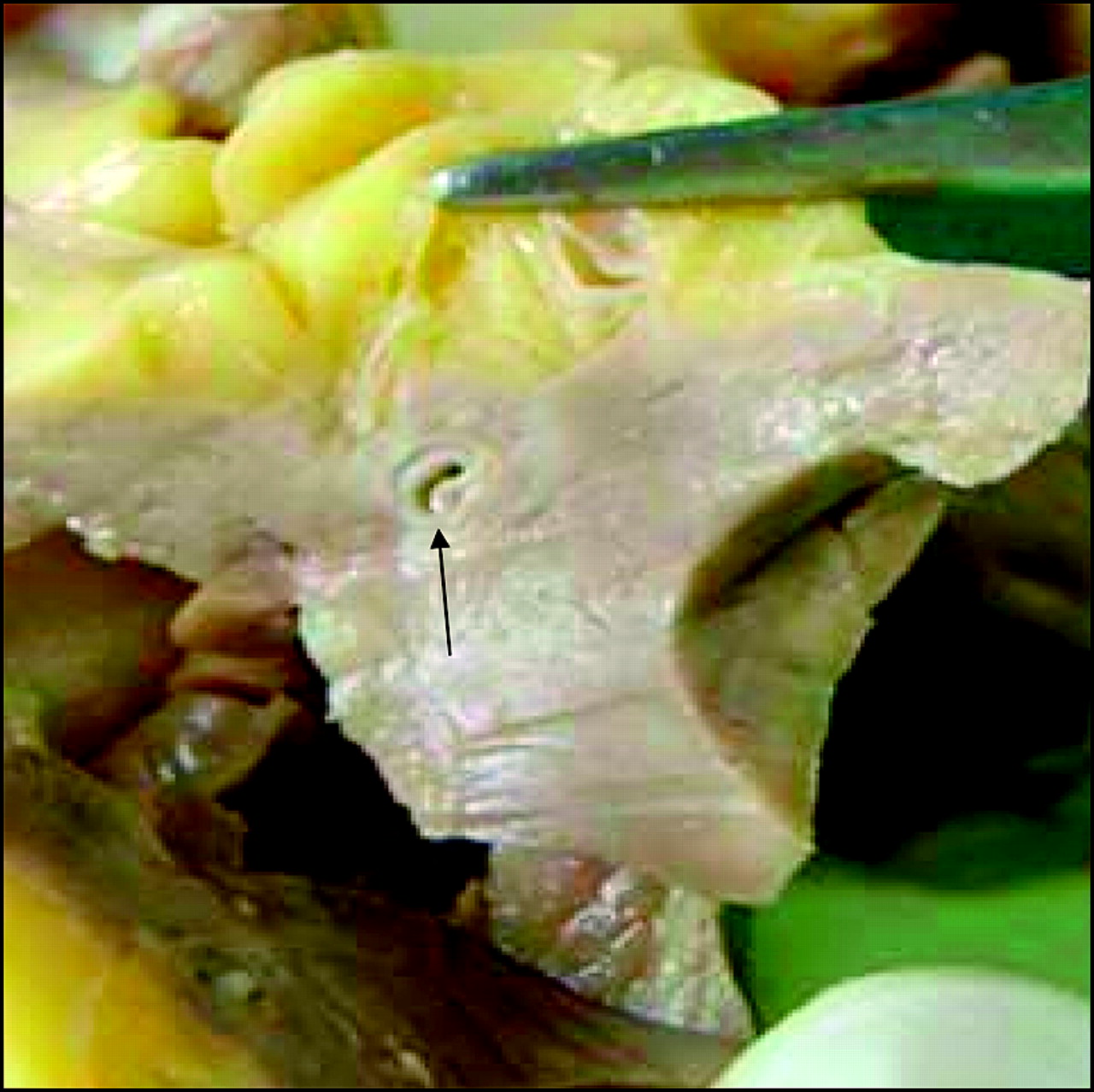
Coronary artery ostial stenosis/atresia was seen in three cases: two children and an adolescent. One patient had RCA ostial stenosis with narrowing of the vessel; in the second patient the LCA ostium was narrowed by a shelf lesion; while the third case had no LCA ostium with a small elliptical indentation (figure 4) with hypoplasia of the left anterior descending and circumflex coronary arteries.
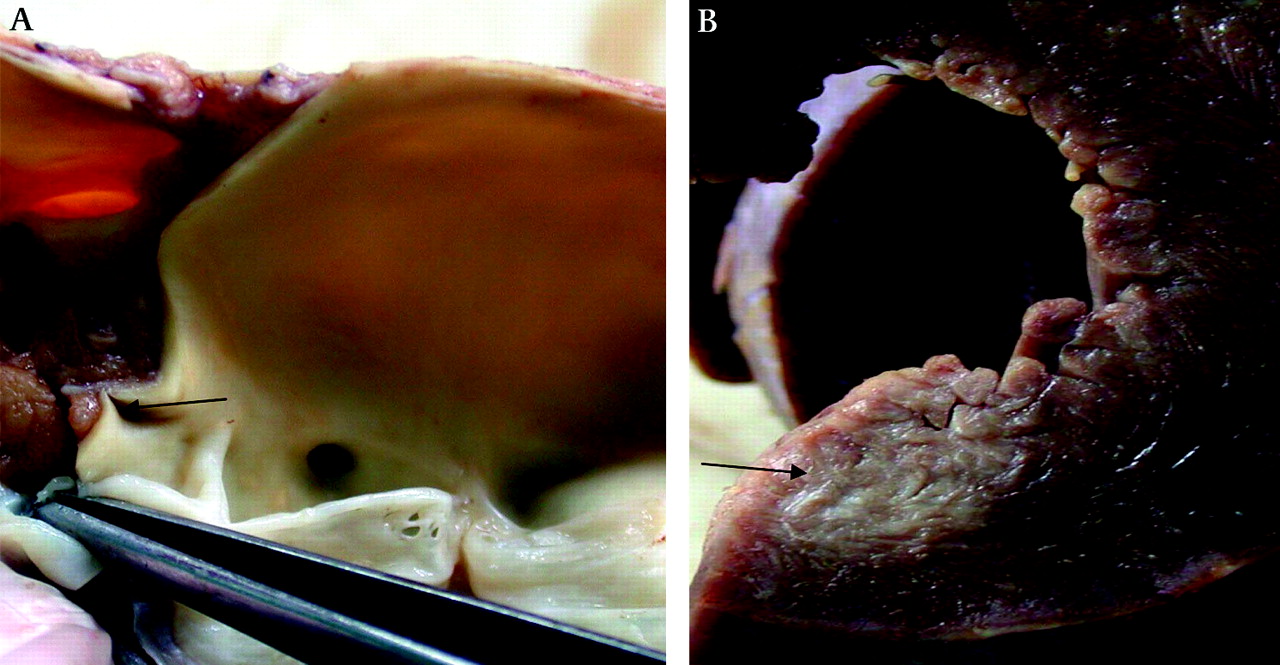
Cardiac morphology of a 17 year old boy who died suddenly while playing football. (A) The aortic root shows that the proximal left coronary artery is atretic with no orifice (arrow). (B) Gross view of the left ventricle showing resultant focal fibrosis of the wall (arrow).
The third group consisted of eight cases of myocardial bridging of the proximal left anterior descending artery (LAD) (figure 5). The myocardial bridge varied from 15 mm to 30 mm in length and from 2 mm to 5 mm in depth. In three cases myocyte disarray was present in the immediate vicinity of the bridged artery. Cardiomyopathy was excluded in these cases because there was no disarray elsewhere in the ventricular myocardium.
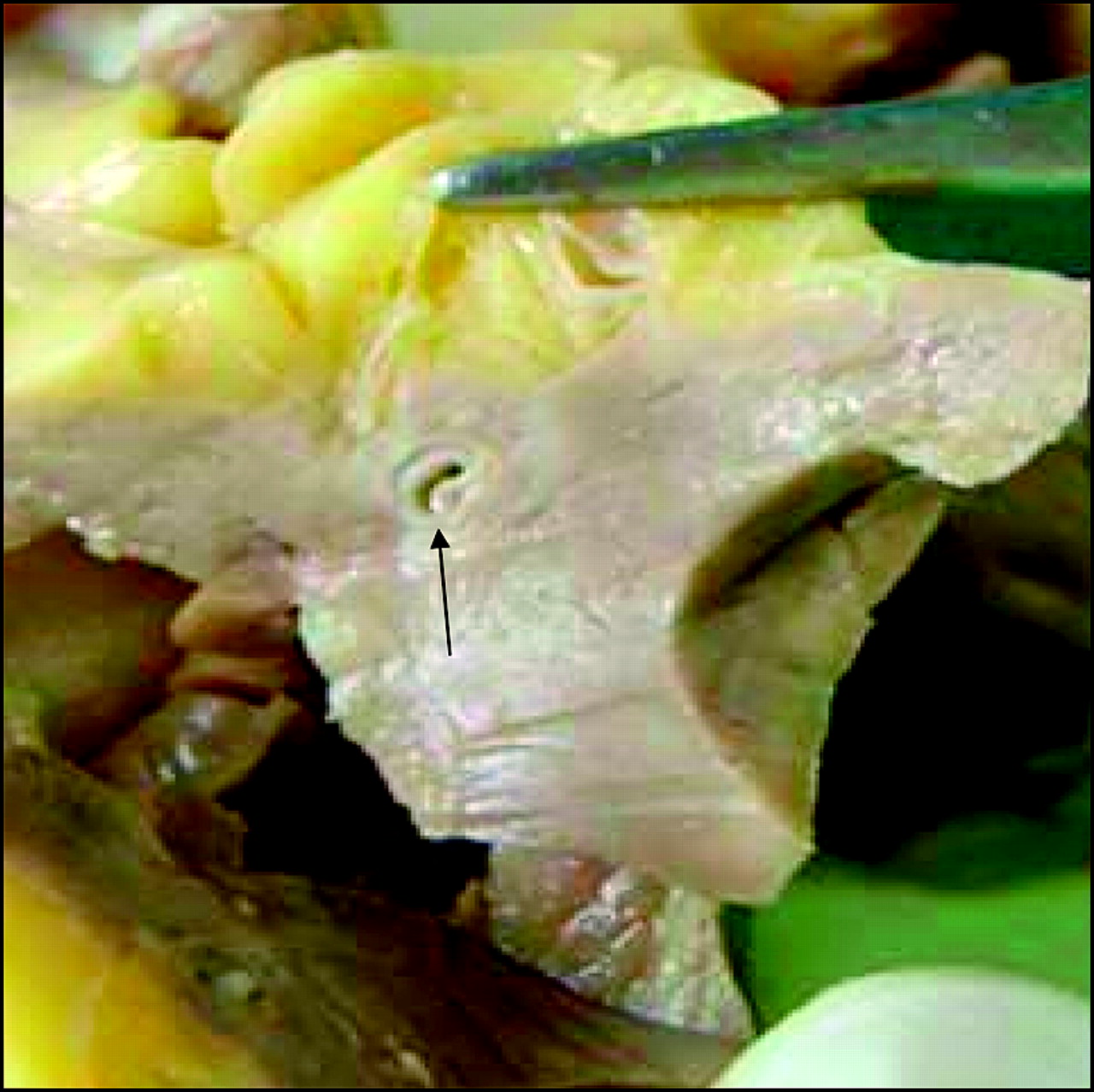
Cardiac morphology of a 50 year old man who died suddenly at rest. Left ventricular myocardium showing the bridged left anterior descending artery tunnelling through muscle at a depth of 4–5 mm (arrow).
Acute dissection of the coronary artery was associated with SCD in eight of the 50 cases and accounted for 0.5% of all-cause SCDs (table 1). This occurred in the LAD in five patients; in the RCA in two cases; and the left main stem, LAD and RCA in one case (figure 6). Notably, five of the eight patients were women, four being between 30 and 40 years of age, including one woman who was 8 weeks post partum. Acute dissection of the LAD was predominantly found in female subjects, whereas acute dissection affecting the RCA was mostly found in male subjects. Marfan syndrome was not detected at autopsy in any case.

Cardiac morphology of a 39 year old woman who died suddenly 8 weeks post partum. High-power view of dissected artery showing an intramural haematoma (black arrow) and a slit-like lumen (red arrow). (Magnification ×100).
Coronary artery vasculitis was attributed to SCD in six patients, 0.4% of all-cause SCDs (table 1). Three of the cases were idiopathic, two cases were associated with Churg–Strauss syndrome, one was associated with an inflammatory pseudotumour of the kidney with IgG paraproteinaemia and one case had concomitant aortitis. Histologically, four of the six cases displayed a prominent eosinophilic component, one case was predominantly lymphocytic and the remaining case showed giant cells. Arterial occlusion was evident on histological analysis in all of the cases, either due to extensive fibrointimal proliferation or intravascular thrombosis.
Coronary artery spasm was associated with death in six patients, accounting for 0.4% of all-cause SCDs (table 1). Signs of acute ischaemic damage with variable evidence of chronic damage were noted in the anteroseptal wall of the ventricular myocardium in the presence of completely normal coronary arteries. Other identifiable causes of SCD were excluded. One of the patients had a history of drug abuse.
Idiopathic arterial calcification of infancy (IACI) was associated with SCD in three cases, which equates to 0.2% of all-cause SCDs (table 1). The patients were all female, two of them were under 6 months old and one was aged 11. In all three cases, histology revealed extensive calcification of the elastic lamina with overlying fibrointimal proliferation, causing occlusion of the affected vessels.
Fibromuscular dysplasia (FMD) affecting the coronary arteries was found in two of the 50 cases, 0.1% of all-cause SCDs (table 1). They were brothers, aged 23 and 18 when they died. They had a family history of young death and experienced cardiac symptoms. Severe arterial occlusion was seen on histology, in the form of extensive fibrous tissue rich in myofibroblasts occluding the lumen with marked intimal hyperplasia.
A benign lipoma occluding the ostium of the left main stem artery of a 52 year old man was the probable cause of SCD in the final case, accounting for 0.06% of the total number of SCDs (table 1). The fatty mass was 10 mm × 10 mm in size and was adherent to the ostium of the left main stem (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cardiac morphology of a 52 year old man who died suddenly at rest. Aortic root showing a benign lipoma occluding the ostium of the left main coronary artery (arrow).
Table 2 reports the age and gender distribution of each anomaly as well as conveying the number of patients who complained of cardiac symptoms.
Table 3 summarises the main ischaemic pathological findings for all of the above cases. While the majority of cases showed signs of ischaemic damage to the ventricular myocardium, no histological evidence of ischaemia was observed in 11 of the hearts (22%) including some patients with anomalous coronary arteries, acute coronary dissection, coronary artery vasculitis and IACI. In all the 39 cases where ischaemic damage was apparent, it was present in the area of distribution of the abnormal coronary artery. When present, the myocardial fibrosis often involved the inner one-third of the wall and trabeculae, indicating an ischaemic origin.
Quantification of the ischaemic pathological findings for each cause of sudden cardiac death (SCD)
Discussion
There are no large studies to date which review a broad range of non-atherosclerotic coronary disease in relation to SCD in all age groups. Our aim was to draw attention to this under-recognised entity, which includes anomalous coronary arteries, coronary artery dissection, coronary artery vasculitis, coronary artery spasm, IACI, FMD and a tumour occluding the left main stem. Forty per cent of the patients experienced cardiac symptoms, including angina, syncope and breathlessness before their death. The remaining patients were asymptomatic and died suddenly. We have drawn on previous knowledge of these conditions and added further information collected from our large cohort of 50 cases.
Non-atherosclerotic coronary pathology was associated with 3.0% of SCDs in this series (50 of 1647 cases). Previous research has used either angiographic or autopsy methods to define the incidence of coronary anomalies. According to the angiographic literature, coronary anomalies affect approximately 1% of the population; this percentage is derived from coronary angiograms performed for suspected coronary obstructive disease.10 Yamanaka and Hobbs reviewed 126 595 angiograms, and coronary artery anomalies were found in 1686 patients (1.3% incidence).11 It is important to note that angiographic studies do not reflect the incidence in the general population as the study samples consist of patients being investigated for coronary artery disease as a result of having symptoms or multiple risk factors.
Necropsy studies yield an even lower incidence: in 18 950 necropsies, Alexander and Griffith observed only 54 coronary anomalies (0.3%).12 In an autopsy series of 270 cases by Chugh et al, non-atherosclerotic coronary pathology had a prevalence of 5.6%.13 The majority of patients (66%) were >35 years of age, with a mean age of 42. Coronary artery disease was the most common finding in their study accounting for 65% of SCDs with no overlap between the two entities. Corrado et al studied 273 autopsies of SCD in the ≤35 age group and found non-atherosclerotic coronary artery pathology accounted for 10.3% of deaths.14 In their series, cardiomyopathy accounted for the largest proportion of SCDs (21%). The difference in prevalence could be explained by the different age distribution and sample sizes of the above studies compared with our series.
Most previous research reviewing non-atherosclerotic coronary artery pathology has focused on the <35 year age group.14 15 However, 22 of the patients in this study (44%) were >35 years of age, highlighting that non-atherosclerotic coronary artery disease is relevant in the older adult population as well as in the younger adults where more attention is focused. Coronary artery stenosis/atresia and IACI affect mainly the paediatric age group and paediatric cardiologists need to be aware of these rare entities. Anomalous coronary arteries and FMD appear to affect mainly the younger adult population (<35 years), whereas coronary artery dissection, spasm and vasculitis are more prevalent in the older adult population.
The frequency of non-atherosclerotic coronary artery pathology compared with other non-ischaemic causes of SCD was highlighted in an earlier autopsy study by Fabre and Sheppard.16 Non-ischaemic cases of SCD referred to our centre between 1994 and 2003 were analysed. Non-atherosclerotic coronary artery pathology accounted for 4.6% of deaths; sudden adult death syndrome with structurally normal hearts 59.3%; cardiomyopathies 23%; inflammatory disorders including myocarditis and cardiac sarcoidosis 8.6%; valvar abnormalities, conduction system defects, congenital heart disease and other rare abnormalities accounted for the remaining 4.5%.
The probable mechanism of SCD in all cases in this series is believed to be ventricular arrhythmia as a result of ischaemia. However, no histological evidence of ischaemic damage was observed in 11 of the hearts (22%) in this study. The mechanism of death in such cases remains controversial. In the classic study from Seattle, only 20% of survivors from out-of-hospital cardiac arrests had a new transmural infarction, with a significant number showing no infarction or necrosis in the post-resuscitation period.17
Anomalous coronary arteries
Anomalous coronary arteries while reported as rare are an acknowledged cause of SCD in adolescents and young adults.18–20 In this series, congenital anomalies of the coronary arteries accounted for the largest percentage of non-atherosclerotic causes of SCD (48%) and 1.5% of all-cause SCD. In a smaller autopsy series, Drory et al reported the incidence of anomalous coronary artery-related SCD as 0.6%; however, all their cases were aged ≤40 years.21 Rodriguez et al reported the prevalence of coronary artery anomalies in an adult population assessed by CT coronary angiography as 21%.22
Patients with an anomalous coronary artery have a high risk for sudden death during or immediately after exertion.23 Our study confirms this, with all of the 12 patients who had a sports-related SCD in our study having an anomalous coronary artery.
Anomalous origin of a coronary artery from the opposite sinus is well established as a cause of sudden death.24–26 Frequently quoted autopsy reports have suggested a 57% mortality for an anomalous LCA originating from the right coronary sinus, and a 25% mortality rate for RCA originating from the left coronary sinus.20 27 On histological analysis, four of the five cases of ectopic LCA showed ischaemic damage, compared with only four of the eight cases of ectopic RCA, reflecting the greater mortality with LCA origin. No association was found between patients who experienced cardiac symptoms and patients in whom ischaemic damage was seen histologically. In the five cases where no evidence of ischaemic damage was seen we cannot be certain that the patient's anomalous origin of a coronary artery definitely caused their death—the possibility of a primary arrhythmic event cannot be excluded.
In recent literature, familial cases of anomalous coronary artery origin with an interarterial course have been reported. Brothers et al identified five families in which a child was diagnosed with anomalous origin of a coronary artery and another family member was subsequently identified through screening with echocardiography.28 Therefore, screening of first-degree relatives for anomalous origin of a coronary artery using transthoracic echocardiography is advised.29
High take-off of the coronary artery has been associated with SCD.25 This study confirms that it is an extremely rare cause of SCD. It is well established that there is normal anatomical variation in the location of coronary ostia at, below and above the sinotubular junction.30 Muriago et al proposed that a relative measurement of 120% or more of the depth of the sinus should be used as the criterion for pathological high take off.30
Coronary artery ostial stenosis/atresia is another rare cause of SCD.25 31 32 Most reported cases have been described in infants and children.33
Myocardial bridging is a congenital coronary anomaly with several possible manifestations, including SCD, but its clinical relevance is debated.26 The prevalence of myocardial bridging varies greatly in reported studies, ranging from 0.5%–2.5% on angiography to 5.4%–85.7% at pathological analysis.34 It is a condition, in which a band of cardiac muscle overlies the coronary artery along its course in the epicardial adipose tissue for a varying length of segment.35 As a consequence, compression of the coronary artery lumen in systole, extending into diastole, is the main functional consequence of this anatomic abnormality.36 It has been reported that this anomaly is of clinical and pathological significance when it has a long (20–30 mm) and deep (2–3 mm) intramyocardial course.35 However, in one of the cases we reviewed, the length of the bridge was shorter, measuring 15 mm with ischaemic damage, highlighting that shorter bridges can be clinically significant. No ischaemic damage was evident in one case, posing controversy over whether the bridged artery was the cause of SCD. However, the patient was under exertion at the time of death, which could potentially cause spasm of the bridged artery. The association between coronary artery spasm and myocardial bridging has been previously reported.37
Myocardial bridging is also considered to be a benign anatomical variant. Julliére et al studied the long-term outcome of 28 patients who had isolated myocardial bridges with systolic compression at baseline. None of the patients had a myocardial infarction during follow-up (11±3 years), indicating that most patients with myocardial bridging have a good prognosis.38
Coronary artery dissection
Spontaneous coronary artery dissection remains a rare but important cause of sudden cardiac death.39 It has been defined as an intramural haematoma of the media of the vessel wall which flattens the true lumen, leading to blood flow obstruction and acute myocardial ischaemia.40 In a review by Basso et al, 80% of the cases of spontaneous coronary artery dissection occurred in female subjects, particularly in post partum period.40 We also found a female predominance; with five of the eight cases being female, but only one of our cases occurred in the postpartum period. The association between the peripartum period and spontaneous coronary dissection has been linked to progestogen-dependent connective tissue changes, which weaken the coronary arterial wall.40 41
Coronary artery vasculitis
Coronary artery vasculitis is a rare cause of SCD and may occur as an isolated form of vasculitis or as a manifestation of systemic diseases such as Kawasaki disease, Churg–Strauss syndrome or systemic lupus erythematosus.42 Our study shows that there is wide variation in the type of vasculitis, with eosinophilic, lymphocytic and giant cell types being identified.
Coronary artery spasm
Coronary artery spasm is a controversial topic for pathologists as it is impossible to detect on histological analysis and it is diagnosed by exclusion of other causes (myocarditis, cardiomyopathy, valvar abnormalities). It was presumed to be the cause of SCD in these cases because of the presence of transmural myocardial ischaemic damage (acute and/or chronic) limited to the anteroseptal wall of the left ventricle (the region of distribution of the LCA) in the absence of any coronary artery pathology. Thrombotic/embolic disease with lysis is a possibility in these cases, but no source for thrombosis or emboli was found at autopsy. Obviously, coronary artery spasm/transient blockage is only an association and a primary arrhythmic event cannot be excluded as the cause of SCD.
Idiopathic arterial calcification of infancy
IACI is a genetically inherited autosomal recessive condition characterised by extensive arterial calcification and stenosis of large and medium-sized arteries.43 It is caused by homozygous or heterozygous mutations in the ectonucleotide pyrophosphatase/phosphodiesterase 1 (ENPP1) gene.44 ENPP1 regulates extracellular inorganic pyrophosphate, a major inhibiter of extracellular matrix calcification. Accurate diagnosis is important since follow-up with genetic counselling is mandatory.
Fibromuscular dysplasia
FMD is currently defined as an idiopathic, segmental, non-inflammatory and non-atherosclerotic disease of the musculature of arterial walls, leading to stenosis of small and medium-sized arteries.45 The aetiology of FMD is unknown. Several hypotheses have been postulated, such as hormonal effects, developmental abnormalities of the vessel wall and genetic factors.46 47 The last of these is significant in this study as both cases were brothers.
Benign tumour
A benign lipoma occluding the ostium of the left main stem was the probable cause of SCD in one of the cases in this study. Rhabdomyomas, atrial myxomas, cardiac fibromas and lipomas located at various other sites in the heart have been associated with sudden death.48
Limitations
A retrospective study of highly selective referrals may not reflect the true prevalence of non-atherosclerotic coronary disease in the UK general population. Second, in cases where no ischaemic damage was evident on histological analysis of the heart it is difficult to associate the coronary abnormality with SCD, and a primary arrhythmic event cannot be excluded.
Conclusions
The data we have collected highlight the association between non-atherosclerotic coronary disease and myocardial ischaemia and SCD in all age groups, particularly younger, male patients. Cardiologists should investigate any patient who presents with cardiac symptoms, especially those occurring with exertion, and be aware of the differential diagnosis of non-atherosclerotic coronary disease. In the era of multidetector CT equipment more cases have the potential to be detected during life allowing action to be taken to reduce the likelihood of a future SCD.49
Acknowledgments
We thank the charity CRY (Cardiac Risk in the Young) for a grant which enabled us to do this work. (http://www.c-r-y.org.uk).