Article Text

Abstract
Background Percutaneous coronary intervention (PCI) of small vessels is limited by an increased risk of restenosis and adverse outcome, even when drug-eluting stents (DES) are employed. In recent years, the paclitaxel-coated balloon (PCB) has been shown to reduce neointimal proliferation and the need for target lesion revascularization (TLR) in an in-stent restenosis setting. The impact of a PCB during PCI of small coronary vessels was evaluated and compared to one of the most widely used DES.
Methods In the PICCOLETO randomised clinical trial, patients with stable or unstable angina undergoing PCI of small coronary vessels (≤2.75 mm) were randomised to Dior PCB (28 patients) or Taxus DES (29 patients). The primary study end point was per cent diameter stenosis at 6-month angiographic follow-up (non-inferiority), secondary end points were angiographic binary restenosis and occurrence of major adverse cardiac events (MACE: death, Q-wave myocardial infarction, TLR) at 9 month follow-up.
Results The two groups were not dissimilar regarding clinical and angiographic characteristics. Study was interrupted after enrolment of two-thirds of patients due to a clear superiority of one study group. The primary end point was not met, because the PCB group showed higher per cent diameter stenosis (43.6% vs 24.3%, p=0.029); angiographic restenosis was higher as well (32.1 vs 10.3%, p=0.043), whereas MACE were 35.7% in the PCB group and 13.8% in the DES group (p=0.054).
Conclusions Dior PCB failed to show equivalence to Taxus DES regarding angiographic end points during PCI of small coronary arteries.
Clinical Trial Registration Number (EudraCT code) 2009-012268-15.
- Coronary angioplasty (PCI)
Statistics from Altmetric.com
Percutaneous coronary intervention (PCI) of small calibre coronary vessels is a true challenge for modern interventional cardiology, due to the increased risk of restenosis and adverse outcome.1 However, drug-eluting stent (DES) use, thanks to local delivery of therapeutic agents to reduce neointimal hyperplasia, has changed this scenario.2 Nevertheless, the increased risk of stent thrombosis3 4 or death5 at any time after stent implantation remains a matter of concern in all vessel calibres, even if specific scientific data are lacking.
Compared to a standard, uncoated balloon, a paclitaxel-coated balloon (PCB) has been shown to reduce neointimal proliferation and the need for target lesion revascularisation (TLR) in an in-stent restenosis setting,6 and recently DES.7 Investigators of these two trials concluded that this new method of local drug delivery would not require stent implantation to fight restenosis.
The purpose of this study was to evaluate the impact of a PCB during PCI of small native coronary vessels compared to standard treatment with DES.
Methods
The PICCOLETO study was a prospective, single centre, randomised trial comparing the efficacy of the Dior PCB (Eurocor, Bonn, Germany) with Taxus Libertè DES (Boston Scientific Corporation, Natick, MA, USA) in small coronary arteries (diameter ≤2.75 mm). The study was entirely conducted at the interventional cardiology unit of Ospedale della Misericordia in Grosseto, Italy.
Between August 2007 and August 2008, after obtaining informed written consent, all consecutive patients of at least 18 years of age with stable or unstable angina and a clinical indication for PCI of at least one small coronary artery were randomised to treatment with PCB or Taxus stent.
Patients were excluded from the study if they met at least one of the following criteria: acute myocardial infarction within the previous 48 h, unstable haemodynamics, chronic renal insufficiency with a serum creatinine level of more than 2.0 mg/dl, known hypersensitivity or contraindication to aspirin, heparin, clopidogrel or paclitaxel, sensitivity to contrast media that could not be controlled with premedication and life expectancy of less than 2 years.
Randomisation was performed in a 1:1 ratio by computerised, open-label assignment in consecutive blinded envelopes. A randomly permuted blocks method was used to generate the randomisation plan. Although operators were not blinded to the device used, the clinical end points were adjudicated by two investigators blinded with regard to patients' treatment allocation. A local ethics committee approved the study. This clinical trial obtained an EudraCT code (2009-012268-15).
The Dior PCB is a coronary dilatation catheter with a nanoporous balloon surface coated with paclitaxel microcrystals. Paclitaxel coating concentration is 3 μg/mm2 of balloon surface area, homogeneously distributed. During inflation, the drug is released onto the vessel wall.
Patients randomised to the control group were treated with the Taxus Libertè DES described elsewhere.8 PCB were available in diameters of 2.25, 2.5 and 2.75 mm, and in lengths of 15–25 mm. Taxus stents were available in diameters of 2.5 and 2.75 mm, and in lengths of 8–32 mm.
Percutaneous coronary intervention was performed according to current international guidelines. Prior to guidewire insertion all patients were administered unfractionated heparin (single bolus of 100 IU/kg, then adjunctive boluses following activated clotting time) or bivalirudin (bolus of 0.75 mg/kg followed by an infusion of 1.75 mg/kg/h for the duration of procedure). A bailout glycoprotein IIb/IIIa receptor inhibitor strategy was recommended in the two groups only in case of procedural thrombotic complications, big coronary clots and complex or prolonged intervention.
All patients undergoing PCI received aspirin (either 100 mg/day for at least 3 days prior to PCI or a pre-PCI 300 mg intravenous bolus), and clopidogrel (300 or 600 mg as a loading dose, followed by 75 mg daily). Patients were considered to be adequately loaded with clopidogrel if they were on chronic therapy or had been treated with a loading dose of 600 mg >2 h or 300 mg >6 h before PCI.9 10
Predilatation was recommended in patients undergoing Taxus implantation. In the PCB group, a gentle balloon deployment was attempted, otherwise in case of resistance a predilatation with uncoated balloon was also recommended. In all cases of difficult PCB positioning, investigators were asked to change the device in order to maintain an adequate paclitaxel coating.
Paclitaxel-eluting stent (ES) inflation time was 20–30 s, afterward all stents were postdilated with a non-compliant, standard balloon; PCB inflation time was 45 s repeated twice, and recommended dilatation pressures were between 8 and 16 atmospheres.
In case of unsatisfactory angiographic result after PCB inflation (persistent dissection other than A type following National Heart, Lung and Blood Institute (NHLBI) classification11 and/or final thrombolysis in myocardial infarction (TIMI) flow <3), patients underwent per protocol bare metal stent (BMS) (ML Vision; Abbott Vascular, Abbott Park, Illinois, USA).
Angiographic success was defined, based on a visual estimation, as a final angiographic residual stenosis of <30% with TIMI 3 flow and the absence of evident coronary dissection. Procedural success was determined based on a satisfactory angiographic outcome and absence of any major in-hospital complication (acute myocardial infarction, need for target vessel revascularisation or death).
All patients continued aspirin indefinitely and clopidogrel 75 mg daily for 1 month in cases of stable angina and lone PCB use, 3 months in cases of PCB and provisional stent implantation and 12 months in cases of unstable angina or Taxus implantation.
Clinical follow-up visits were scheduled 30 days, 6 months and 9 months after index procedure in all study patients. All patients were also scheduled to undergo angiographic follow-up between 6 and 8 months after index procedure. An interim analysis was planned after enrolment of 65% of patients. In the case of lack of equivalence between the two study groups regarding primary end point, it was planned to stop enrolment.
Angiography was performed before and after all interventions and at 6 months follow-up. All measurements were performed on cineangiograms recorded after 200 μg of intracoronary nitroglycerin administration. Identical projections were used for each comparison. Quantitative analysis of the coronary angiographic images was performed by one of the study investigators. The CAAS II research system (Pie Medical Imaging) was used for automated contour detection and quantification. The parameters that were measured included: lesion length, reference vessel diameter, minimal lumen diameter and per cent diameter stenosis (difference between reference diameter and minimal lumen diameter divided by reference diameter and multiplied by 100).
Measurements included the inner stenotic area, the stented area with measurement shoulder to shoulder (in-stent) and the total stented area plus 5 mm of the proximal and distal area (in-segment); in the case of PCB use without stenting, the area corresponding to the balloon length plus 5 mm proximally and distally was measured. Angiographic restenosis was defined as stenosis of at least 50% of the luminal diameter.
Study end points were analysed by intention-to-treat. The prespecified primary end point of the study was the per cent diameter stenosis of the culprit lesion at 6 months angiographic follow-up obtained with QCA, where non-inferiority between the two study groups was hypothesised.
Secondary end points of the study were:
–angiographic binary restenosis at QCA (non-inferiority);
–occurrence of major adverse cardiac events (MACE: death, new ST elevation myocardial infarction12 and TLR) at 9 months clinical follow-up (non-inferiority).
It was decided not to use late lumen loss analysis, a common end point in clinical studies with stents and angiographic follow-up,13 because in the authors' opinion the possible acute recoil in the PCB group would have underestimated the results in this group.
The sample size of the trial was calculated on the basis of the findings of a previous randomised trial14: a 30±18% diameter stenosis with the PES was expected at 6 months angiographic follow-up. A similar result for the PCB group, with a +12% threshold, was hypothesised. To achieve this objective, with a power of 80% and a two-sided α-level of 0.05, the target population for each study group was 40 patients with follow-up angiography.
The main analysis was performed on an intention-to-treat basis. Data are presented as mean±SD or as proportions (%). The differences between groups were assessed by χ2 test or Fisher exact test for categorical data and t test for continuous data. The RR and its 95% CI were calculated for each study end point. A two-sided p value <0.05 was considered statistically significant.
Results
Sixty patients were randomised in the PICCOLETO Study, 29 in the PCB group and 31 in the DES group (figure 1). The planned overall 80-patient population was not reached because investigators decided to stop the enrolment after scheduled interim analysis due to an evident supeority of one study group. One patient in the PCB group, and two in the DES group were lost at follow-up (p=0.63).
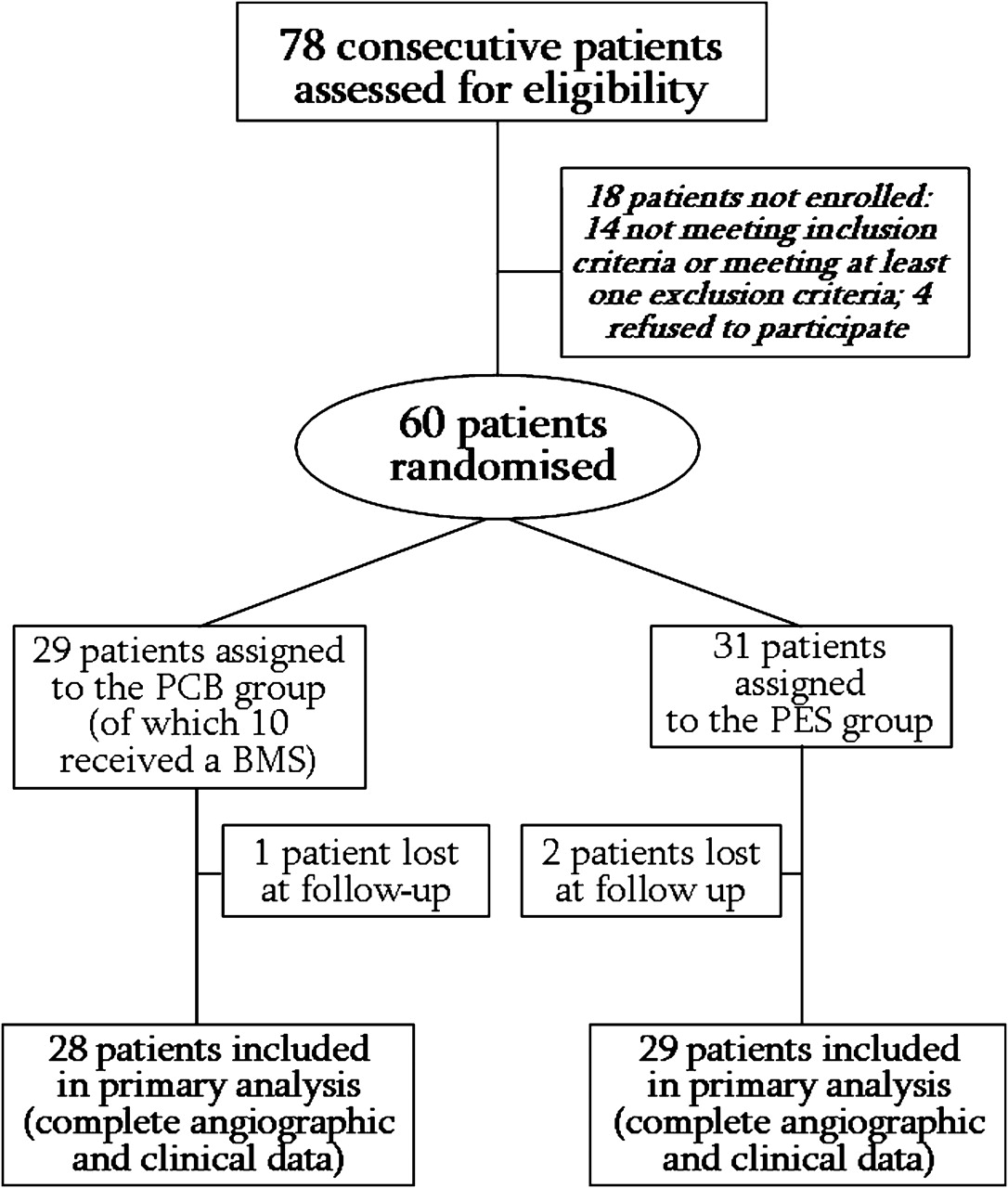
Flow chart of study population of the PICCOLETO trial. PCB, paclitaxel-coated balloon; PES, paclitaxel-eluting stent.
Baseline clinical and angiographic characteristics are shown in table 1. There were no significant differences between the two groups regarding main clinical and angiographic data.
Baseline clinical and angiographic characteristics
Procedural characteristics are shown in table 2. There were no significant differences between study groups regarding multivessel PCI, target vessel and procedural success. On the other hand, as expected, in the DES group there were more stents implanted (p=0.024), lesion predilatation was more common (p=0.001) and a bigger final lumen diameter was achieved (p=0.009).
Procedural characteristics
Complete follow-up angiography at a median of 189 days (IQR: 172 to 201 days) was carried out in 57 patients (95% of enrolled patients). Angiographic outcome is presented in table 3.
Six months angiographic outcome
The prespecified primary end point of the study, per cent diameter stenosis at 6 months follow-up (non-inferiority hypothesised), was not met due to an evident superiority of the Taxus group (24.3±25.1% vs 43.6±27.4%, p=0.029).
The PCB group also showed a higher rate of angiographic binary restenosis, an unmet secondary end point of the study (10.3% vs 32.1%, p=0.043).
Figure 2 shows the cumulative frequency distribution of minimal lumen diameter (MLD) (pre-PCI, post-PCI and at control angiography).

Cumulative frequency distribution of minimal lumen diameter (MLD): pre-percutaneous coronary intervention (PCI), post-PCI and follow-up, in the two study groups. DES, drug-eluting stent; MLD, minimal lumen diameter; PCB, paclitaxel-coated balloon; PES, paclitaxel-eluting stent.
All 57 patients of the study underwent 9 months clinical follow-up (table 4). The number of patients who suffered a MACE was not statistically different across study groups, but a strong trend towards better clinical outcome was discovered in the Taxus group (13.8% vs 35.7%, p=0.054). This result was mainly driven by the increased rate of TLR in the PCB group (32.1% vs 10.3%, p=0.15).
Nine months clinical outcome
Two deaths were registered in the study population (p=0.98): one patient in the PCB group died from intracranial haemorrhage and one in the PES group due to liver malignancy. No cardiac death was observed across study groups, nor any stent thrombosis/abrupt vessel closure. Only one patient in the PCB group suffered an acute Q-wave myocardial infarction in a vessel not treated during index procedure (p=0.30).
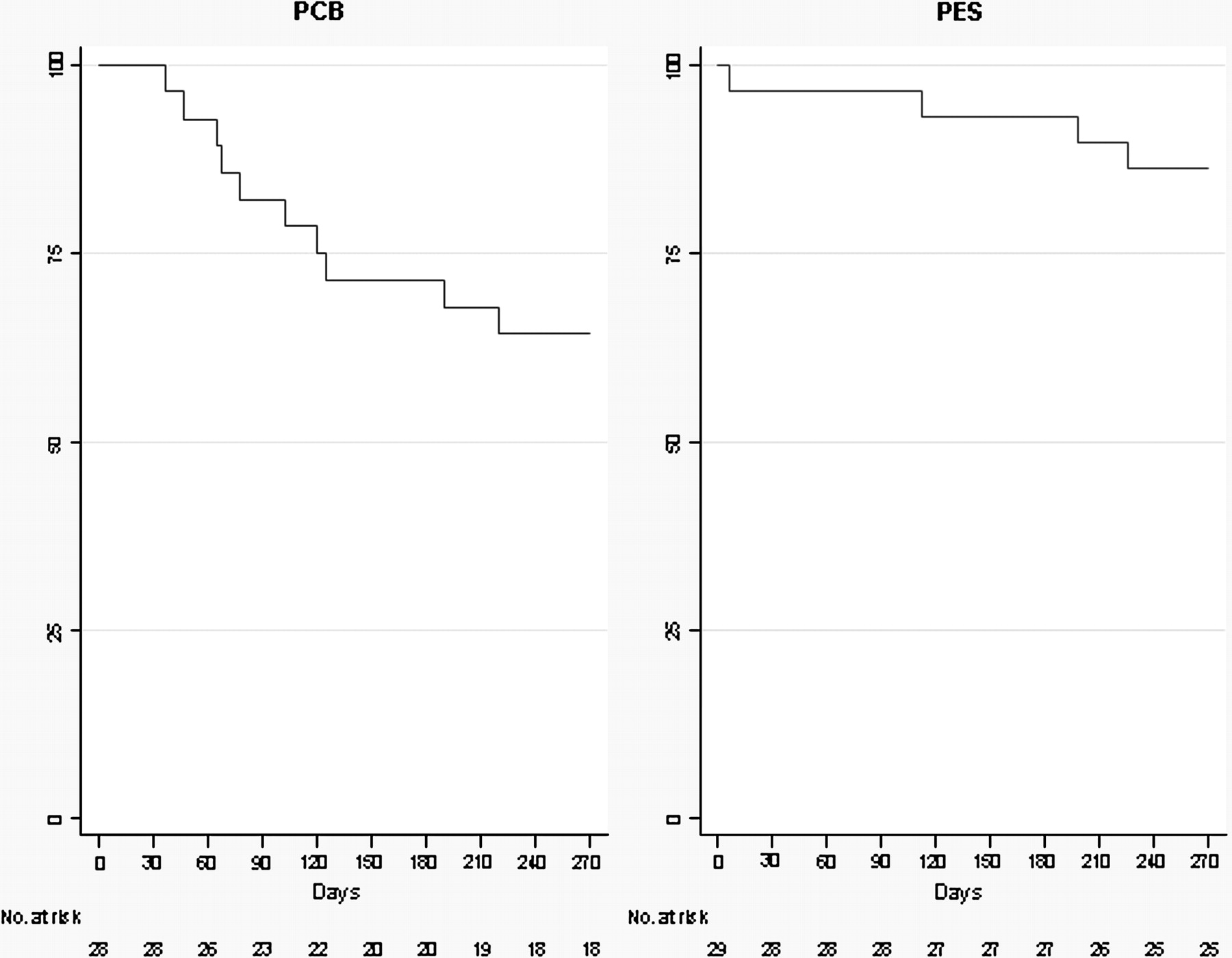
Figure 3 shows Kaplan–Meier curves for MACE, showing early failure of the PCB, mainly driven by increased TLR.
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier curves for MACEs, showing early failure of PCB, due to increased rates of TLR. MACE, major adverse coronary event; PCB, paclitaxel-coated balloon; PES, paclitaxel-eluting stent; TLR, target lesion revascularisation.
Discussion
The PICCOLETO study failed to demonstrate any equivalence between Dior PCB and Taxus stent for the treatment of small coronary artery disease in terms of angiographic restenosis; if patients in the PCB group showed a higher per cent diameter stenosis, patients treated with the Taxus stent experienced an incidence of per cent diameter stenosis lower than expected. Moreover, a strong trend towards better clinical outcome with the Taxus stent has been observed, mainly driven by a higher revascularisation rate in the population treated with PCB. The present findings do not support the original hypothesis of using a PCB for PCI of small coronary artery disease. A simplistic explanation would resolve with the axiom that a stent is always better than a balloon. However, it is believed that before drawing such conclusions, some considerations should be made.
First of all, PCI of small coronary arteries has always brought little satisfaction to interventional cardiologists. If there is a clear superiority of stenting over balloon angioplasty for coronary vessels with diameter ≥3.0 mm,15 this argumentation is controversial for smaller calibre arteries.16 Drug-eluting stent use has changed this scenario, dramatically reducing in-stent restenosis rate and TLR in this setting.17 18 However, the increased risk of stent thrombosis at any time after DES implantation has cooled down the initial enthusiasm. Stent thrombosis risk seems independent from vessel calibre, but is increased in longer lesions and in patients with diabetes mellitus, typical features associated with small vessel disease (in the present population, more than 40% were diabetic) 19 20 The risk of stent thrombosis continues for 5 years after DES implantation,21 whereas the possibility of undergoing major surgery increases with ageing in Western populations.
Moreover, sustained drug release after DES implantation and an imputable inflammatory effect of the polymer have been advocated as possible causes of delayed re-endothelialisation over stent struts, that has been found to be a common feature of this complication.22 On the contrary, the drug-coated balloon, in addition to the absence of a permanent metal prosthesis, allows a rapid dilution of the drug after inflation, that is increased by paclitaxel high tissue penetration and persistence, due to its lipophilic properties.23 Drug distribution is also higher, because in the case of DES implantation only about 15% of the stented vessel wall is covered by struts, whereas a drug-coated balloon allows drug distribution hypothetically all around the vessel wall.
Second, the Dior balloon is the only device of this kind to be marketed in Europe. In the recently published Pepcad II study, the SeQuent Please PCB (B Braun, Melsungen, DE, Germany) achieved better in-segment late lumen loss when compared to the Taxus stent in an in-stent restenosis population.7 Moreover, the not yet published Pepcad I SVD (small vessel disease) study24 was a multicentre, prospective, one-arm registry that showed a very intriguing 0.32 mm late lumen loss and an 11.7% target lesion revascularisation rate at 6 month follow-up.
The Dior PCB utilises a peculiar coating technology, where adherence of paclitaxel is mediated by a roughened surface of the balloon, whereas in the SeQuent Please PCB paclitaxel is stuck to a water-soluble matrix, that warrants complete release of paclitaxel after first balloon expansion, with high bioavailability of the drug on the target site; the two technologies have already been compared in a porcine model, where the latter warranted significantly better inhibition of neointimal proliferation.25 A recent study in which the Dior PCB was tested in a porcine model, showed a 48 h tissue paclitaxel concentration of 0.3 μg/g,26 a quantity of drug that has already been shown to be enough to achieve a complete inhibition of smooth muscle cell proliferation.27
If it is true that different technologies used for DES have already been shown to translate into different clinical outcomes, the same could be argued for PCB.
Another point that deserves mention is the choice of the Taxus stent for the control group. Direct comparisons between Taxus and Cipher (Cordis Corporation, Johnson & Johnson, New Brunswick, New Jersey, USA) stents has shown the superiority of the latter in terms of late lumen loss, TLR and MACEs in patients treated for small vessel disease and in patients with diabetes.14 18 28 Therefore, it is argued that the difference observed in the present study between PCB and Taxus stent could be even higher if a different DES was used.
Finally, an interesting issue to address in future studies is routine implantation of a BMS after PCB use. In the present study only 36% of patients in the PCB group received a stent. The analysis of this small subgroup showed a binary restenosis rate of 28.9% of patients, a finding similar to that of patients treated with the lone PCB. On the contrary, in the above-mentioned Pepcad I SVD registry,24 patients not undergoing stent implantation after PCB achieved an extraordinary low late lumen loss and TLR rate (0.16 mm and 4.9% respectively). However, due to the small population of the present study subgroup, and the non-randomised nature of the Pepcad I SVD study, no conclusion can be drawn about this specific issue, and further specific studies are needed.
A number of limitations about this pilot study should be pointed out. First of all, the nature of the study itself is questionable: comparing a stent to a balloon in small vessels subordinates the second group to acute vessel recoil, an important component of restenosis, independent from the effect of paclitaxel. The population enrolled was small and not sufficient to allow for drawing any clinical conclusions.
Due to the different treatment allocations (randomisation to lone balloon or stent), the study could not be blinded to operators; investigators that analysed the study endpoints were blinded, but about two-thirds of patients in the PCB group did not receive a stent, a difference easily observed by investigators. The particular clinical setting of the study population (small vessel disease, high percentage of patients with diabetes, the exclusion of patients with recent myocardial infarction) renders this study unique, and its results should not be extrapolated to different clinical characteristics.
In conclusion, the technology tested in this study during PCI of small vessel disease was inferior to the gold standard treatment with DES. However, the opportunity for treating coronary lesions without placing a (drug-eluting) stent is too attractive to be left out of further experiments.
References
Footnotes
Linked articles 201376.
Competing interests None.
Ethics approval This study was conducted with the approval of the Ethics Committee, Ospedale della Misericordia, Groseto, Italy, 5 July 2007.
Provenance and peer review Not commissioned; externally peer reviewed.