Article Text

Abstract
Objective Primary percutaneous coronary intervention (PPCI) has been acknowledged by the most recent European guidelines to be the preferred treatment for ST elevation myocardial infarction (STEMI). Patients undergoing PPCI are expected to receive a broad spectrum of anticoagulants and antiplatelet agents, which increases the risk of bleedings, in most cases, at the site of vascular access. The burden of bleeding complications after PPCI is as negative as that of ischemic complications not only on in-hospital morbidity, but also on mid- and long–term survival. Owing to the unique features of the radial artery, transradial approach (TRA) seems able to overcome most of the problems related to vascular access particularly in case of STEMI. In this short review we discuss the results of the latest studies and we highlight not only the safety and feasibility of TRA-PPCI, but also the advantages in terms of morbidity and mortality. We finally report on our experience at OLVG Amsterdam, and how TRA can also change the logistics in case of a PPCI programme (short stay).
- Coronary intervention
- acute coronary syndrome
- STEMI
- delivery of care
Statistics from Altmetric.com
In a recent issue of Heart, Hetherington et al1 presented their experience with primary percutaneous coronary intervention (PPCI) performed either via the transradial (TRA) or the transfemoral approach (TFA). Approximately half of the 1051 patients with ST-elevation acute myocardial infarction (STEMI) recruited were treated by TRA. These patients, when compared to TFA patients, showed not only a significant reduction in major vascular complications (0% vs 1.9%) but also in in-hospital major adverse cardiac events (MACE) (2.6% vs 5.2%). Based on these results, the authors pleaded for a change in patterns of vascular access in cases of PPCI. We could not agree more with them.
PPCI has been acknowledged by the most recent European guidelines to be the preferred treatment for STEMI.2 Patients undergoing PPCI are expected to receive a broad spectrum of anticoagulants and antiplatelet agents, such as heparin (unfractionated or low-molecular-weight), direct thrombin inhibitors, thienopyridines, acetylsalycilic acid and GpIIbIIIa inhibitors, in order to reduce the incidence of short-term and long-term ischaemic events. This strategy, although successful, bears the risk of bleedings, which in the most cases, despite the miniaturisation of catheters and the use of haemostatic devices, involve the site of vascular access: haematomas, free bleeding and retroperitoneal bleeding.3 At present, the burden of bleeding complications after PPCI is as negative as that of ischaemic complications not only on in-hospital morbidity, but also on mid-term and long-term survival.4
In the early 1990s, PPCI was far from being an issue but bleeding complications had already emerged as a major concern: at that time interventional cardiologists had just started to implant coronary stents, and the way to avoid stent thrombosis was to load patients with heparin, oral anticoagulants (warfarin) and aspirin. The frequent occurrence of bleeding complications and longer in-hospital stays was the price to be paid. For these reasons, alternatives were sought for the conventional TFA and, eventually, in 1992, the first patient worldwide underwent an elective PCI via TRA at OLVG Amsterdam.5
The radial artery offered the unique feature to be very superficial, thus easy to puncture, but also easy to compress: adequate haemostasis could be achieved without ‘active’ manual compression, but only by a ‘passive’ pressure device or bandage, which would fix the artery against the bone structures behind it. In addition, no major nerves or veins were located near the artery, minimising the risk of injury of these structures. Later on, the validity of this intuition was confirmed by the first randomised study (ACCESS), where TRA showed clear superiority in terms of access-site complications versus TFA and transbrachial access (0% vs 2.0% and 2.3%).6 Oral anticoagulants have been, in the meanwhile, replaced by new antithrombotic and antiplatelet agents, but TRA remains the best solution for preventing bleedings after PCI when aggressive anticoagulation is sought, such as in cases of acute coronary syndrome (ACS) and STEMI. In the EASY study, for instance, Bertrand et al7 have demonstrated a very low incidence of major bleedings (1.4%) in ACS patients undergoing TRA-PCI when taking clopidogrel and GPIIbIIIa inhibitors (Abciximab). In this study, major bleedings emerged as a strong predictor of MACE and mortality at one-year follow-up. On the other hand, Eichhöfer et al8 showed that patients undergoing PCI when taking GpIIbIIIa inhibitors (eptifibatide) had a higher incidence of vascular complications with TFA, but not TRA (1.5% vs 0.6%). Not surprisingly, in their study PPCI presented a higher likelihood of access-site complications than elective PCI.
The first study exploring the safety and feasibility of PPCI via TRA dates back to 1998. In this seminal experience, Ochiai et al9 reported on a series of 33 patients with STEMI who underwent a successful PPCI (with stenting) via TRA. There were no bleeding complications and only one patient died because of the sequelae of a wide antero-septal infarction. A taboo was broken and many other series of PPCI via TRA have been published since then.10–15 Some randomised studies also took place,16–22 but, because of the limited number of patients enrolled and the lack of hard endpoints (mortality, MACE), they did not make a significant breakthrough among the worldwide interventional audience (table 1). As a matter of fact, interventional cardiologists who believe in the advantages of TRA and have chosen to adopt it systematically, are reluctant to expose patients to TFA; the risk is that randomised trials will be conducted by operators who are not as proficient in TRA as in TFA.23 Without robust scientific evidence to support the use of TRA in cases of PPCI, its penetration into clinical practice has been, up to now, shallow. In the USA, TRA still accounts for only 10% of the overall PCI procedures; in Europe and Asia this percentage grows to approximately 30% but still shows a scattered pattern: while some centres perform TRA as the preferred approach (also for PPCI), some others turn to TRA only as a second choice. In the past year, by pooling the results of 12 different studies, Vorobcsuk et al24 gathered a population of 3324 patients who underwent PPCI either via TRA of TFA: they showed an overwhelming 70% reduction in access-site bleeding complications with TRA (0.77% vs 2.61%, OR 0.30). This accomplishment further translated to a lower incidence of MACE (3.65% vs 6.55%, OR 0.56) and mortality (2.0% vs 3.1%, OR 0.54).
A list of randomised studies comparing TRA and TFA for PPCI: procedural times and success, major bleeding rates, in-hospital deaths and MACE at follow-up
A greater awareness that bleeding can be as dangerous as ischaemic complications and the publication of new studies, which for the first time unveiled the link between arterial access, bleeding complications and mortality, have given in the past few years, both in the scientific arena and in clinical practice, an incredible momentum to the issue of TRA-PPCI. The first to be mentioned is probably the MORTAL registry, which retrospectively analysed 38 872 patients who had undergone PCI either via TRA (7972 patients) or via TFA (30 900 patients). Chase et al25 showed in this study that the need for blood transfusion (as an indirect indicator of major bleeding) was halved (1.4% vs 2.8%) by TRA and one-year mortality decreased accordingly from 3.9% to 2.8%. Of note, around two-thirds of the study population were ACS patients who were treated on an urgent basis. Then the PREVAIL study was published, in which Pristipino et al26 prospectively sought for bleeding and vascular complications in 1052 patients who had undergone coronary procedures either via TRA or TFA. In the subgroup of ACS/STEMI patients, both the compositae of bleeding (3.2% vs 6.9%) and ischaemic complications, including death (1.1% vs 4.9%), were in favour of TRA. Last but not least, the study of Rao et al,27 who screened 593 094 (among which 7804 TRA) procedures from the US National Cardiovascular Data Registry, and found that the risk for bleeding and vascular complications was much lower for TRA than for TFA, with a more pronounced spread in STEMI patients (0% vs 3.86%).
In our department at OLVG Amsterdam TRA-PPCI is a credo that renounces any possible abjuration. In 2009 we performed 558 PPCI, among which 95% were TRA (unpublished data). The only reason not to perform TRA was when the radial pulsation was absent or bilaterally too weak to attempt puncture. Cardiogenic shock was not considered an absolute contraindication for TRA, provided that the radial artery was palpable, possibly after insertion of an intra-aortic balloon pump through the groin. Allen's test was never performed, because it is, in our view, inaccurate to detect a patent ulnar supply and not efficacious to predict the development of collateral circulation if radial occlusion occurs. In less than 1% of the cases a crossover to TFA was needed, because of inability either to cannulate the radial artery or to reach the coronary ostia. In most cases, in order to reduce manipulation and thus radial spasm, a catheter was chosen which could fit both the left and the right coronary ostium (Kimny, Boston Scientific, Maastricht, The Netherlands). After the procedure, the sheath was immediately removed and haemostasis was maintained for approximately 4 h.
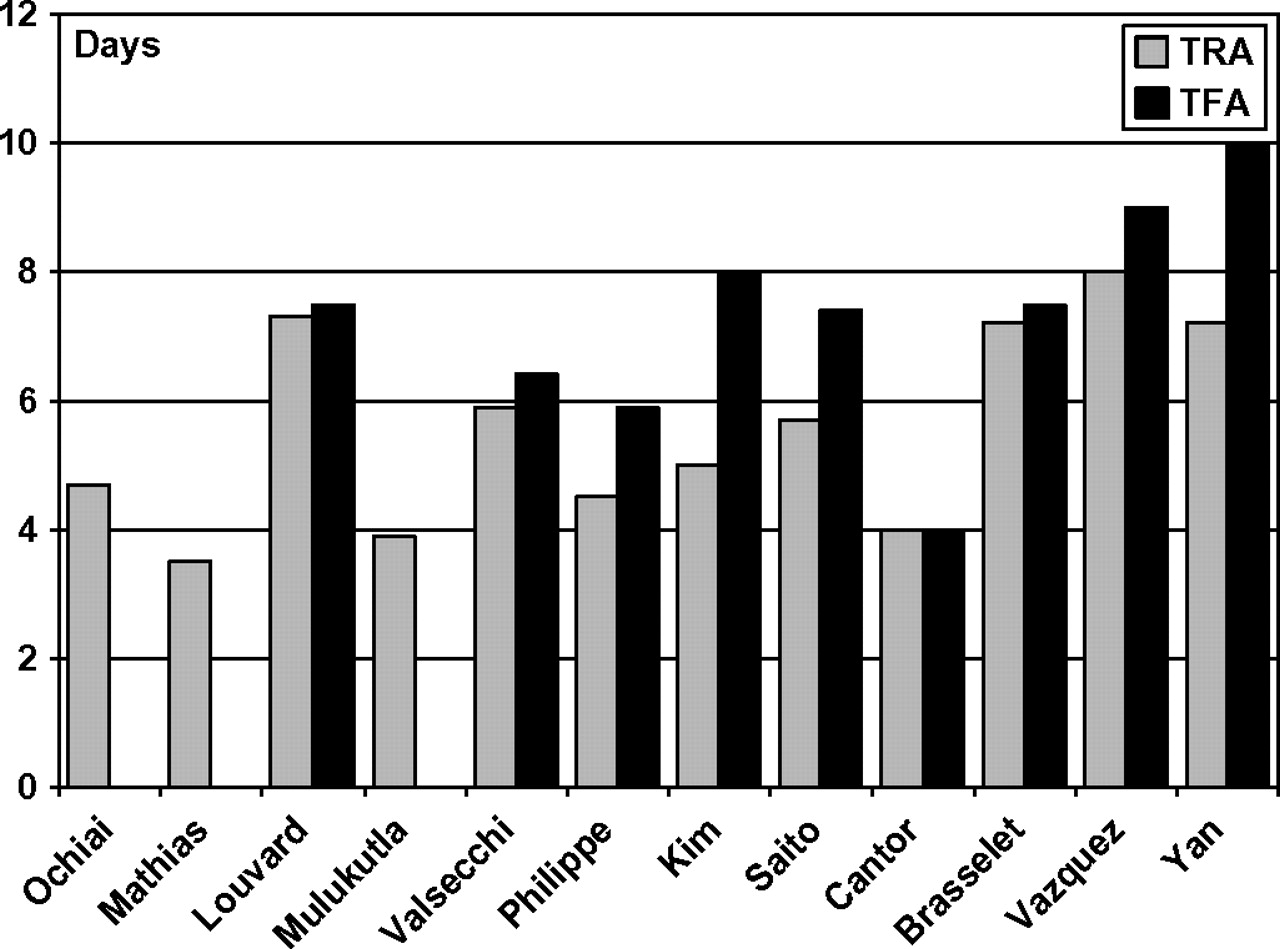
In the early days after a successful PPCI serious adverse events can occur, making these patients not suitable for a day-hospital treatment. However, by reducing bleeding complications at no cost to procedural success and by allowing fast mobilisation of the patient, TRA helps reduce the average in-hospital stay of STEMI patients (figure 1). In our experience, for instance, by careful patient stratification, a subgroup of uneventful STEMI patients who had undergone a successful PPCI, and did not show high-risk features, could see their in-hospital stay minimised to 3–4 days.28 Moreover, given that most of the PPCI programmes are based on a ‘hub-spokes’ network, low to intermediate risk patients can be transferred from the PPCI centre to the referring community hospitals, soon after the PPCI (at our department 2-4 h after completion of the PPCI). By simplifying the logistics around the treatment of STEMI and by shortening in-hospital stays, TRA thus helps not only to cut the hospital costs of a PPCI programme but also to make PPCI available for more patients.

{kind=link}
Length of in-hospital stay (in days) after TRA-PPCI in randomised and non-randomised studies. Grey bars, transradial approach (TRA); black bars, transfemoral approach (TFA). The studies are rank ordered by year of publication.
The fear of inferior procedural results and of a longer delay to reperfusion have been, so far, the two major obstacles to the widespread diffusion of TRA for PPCI. Randomised studies have shown thatthere is neither a significant delay in procedural times nor a reduction in success rates if PPCI is performed via TRA, provided the operator is proficient (table 1). Technology has developed in the last few years in a way that most of the materials necessary for a PPCI, even the more advanced devices, such as bifurcation balloons and stents, distal protection devices, catheters for thrombosuction, intravascular ultrasound or optical coherence tomography probes are 6F compatible. The onset of guiding catheters that can be used without sheath insertion (sheathless) will help upsize the available inner lumen and, thus, the easiness of the procedure at no cost for radial complications.
Interventional cardiologists, like many other highly skilled professionals, are sometimes reluctant to abandon a technique that they fully master and in which they trust, such as, in this case, TFA. This is particularly true in the setting of STEMI, when ‘time is muscle’ and any little technical hindrance could lead to catastrophic consequences for the patient. We acknowledge that, as for many other invasive manoeuvres, a learning curve is necessary,29 and that TRA-PPCI should only be performed by operators who have already developed a solid familiarity with the technique (and its pitfalls) in elective settings (table 2): this probably implies that high-volume operators, rather than ‘weekend’ interventionalists, will be more likely to take up and nurture TRA, enough to perform PPCI at a high rate of success. Far from considering this a limitation, we see here instead probably the most appealing advantage of TRA: the opportunity to set high-quality standards for centres and operators performing PPCIs.
A list of possible problems and solutions with TRA
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.