Article Text

Abstract
Aims The aims of the Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART) are to support the improvement of care and evidence-based development of therapy of coronary artery disease (CAD).
Interventions To provide users with online interactive reports monitoring the processes of care and outcomes and allowing direct comparisons over time and with other hospitals. National, regional and county-based reports are publicly presented on a yearly basis.
Setting Every hospital (n=74) in Sweden providing the relevant services participates. Launched in 2009 after merging four national registries on CAD.
Population Consecutive acute coronary syndrome (ACS) patients, and patients undergoing coronary angiography/angioplasty or heart surgery. Includes approximately 80 000 new cases each year.
Startpoints On admission in ACS patients, at coronary angiography in patients with stable CAD.
Baseline data 106 variables for patients with ACS, another 75 variables regarding secondary prevention after 12–14 months, 150 variables for patients undergoing coronary angiography/angioplasty, 100 variables for patients undergoing heart surgery.
Data capture Web-based registry with all data registered online directly by the caregiver.
Data quality A monitor visits approximately 20 hospitals each year. In 2007, there was a 96% agreement.
Endpoints and linkages to other data Merged with the National Cause of Death Register, including information about vital status of all Swedish citizens, the National Patient Registry, containing diagnoses at discharge for all hospital stays in Sweden and the National Registry of Drug prescriptions recording all drug prescriptions in Sweden.
Access to data Available for research by application to the SWEDEHEART steering group.
- Public health
Statistics from Altmetric.com
The Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART) was launched in December 2009 after merging the Register of Information and Knowledge About Swedish Heart Intensive Care Admissions (RIKS–HIA), the Swedish Coronary Angiography and Angioplasty Registry (SCAAR), the Swedish Heart Surgery Registry and the National Registry of Secondary Prevention (SEPHIA). RIKS–HIA was developed as a regional registry in the beginning of the 1990s and was established as a national quality register in 1995. SEPHIA was added to RIKS–HIA in 2005 to register the effects of secondary prevention efforts in patients with acute myocardial infarction (MI). SCAAR was formed in 1998 after a merge of a national angioplasty and a coronary angiography registry, which had been started in the early 1990s by the university hospitals and the smaller hospitals performing coronary angiography. The Swedish Heart Surgery Registry was formed in 1992 for a better review of Swedish heart surgery and a comparison of results between centres.
SWEDEHEART is a national registry of all patients hospitalised for acute coronary syndrome (ACS) or undergoing coronary or valvular intervention for any indication. By merging the four original registries, the whole process of care is kept together and data are entered in one web-based case report form even if the patient is transferred between different units and hospitals. Redundant entering of the same variables is avoided. Every hospital in Sweden providing the relevant services participates except for the secondary prevention part, which so far has been started in 60 out of 74 hospitals. Åland (a region of Finland) joined RIKS–HIA in 2005 and Iceland has been a part of the SCAAR registry since 2008. Both have now also joined the SWEDEHEART registry although their data are kept separate from the Swedish data for the national reviews.
Organisation and funding
SWEDEHEART is led by a steering group, consisting of the chairmen of the working groups of the original four registries and representatives from the Swedish Heart Association and the Swedish Society of Cardiac Nursing. There are four working groups: one for acute cardiac care (RIKS–HIA); one for angiography and angioplasty (SCAAR); one for heart surgery and one for secondary prevention. Uppsala Clinical Research Centre (UCR; http://www.ucr.uu.se), the developer of the web-based version of the registry, takes care of project management, administration, monitoring, quality controls and statistical reports. The registry is financed by the Swedish Association of Local Authorities and Regions (the public healthcare provider). Participating hospitals are not reimbursed by the registry and the costs of local data entry are borne by their internal budget.
The data
Entering data
SWEDEHEART includes patients admitted to hospital because of symptoms suggestive of an ACS and patients undergoing coronary angiography/angioplasty or heart surgery for any indication. The registry enrols approximately 80 000 cases each year; 20 000 with MI, 10 000 with unstable angina, 25 000 with other causes for their symptoms, 40 000 undergoing coronary angiography or angioplasty, of which 55% are due to MI or unstable angina and 7000 undergoing heart surgery. Out of 10 000 patients with MI and younger than 75 years of age, 6000 are followed for 12–14 months regarding secondary prevention (not all hospitals participate in the secondary prevention part). The registry is web based with all data registered online directly by the caregiver and transferred in an encrypted format to a central server. The technical platform, OpenQreg (http://www.sourceforge.net/projects/openqreg/) is published as open source software that can receive data via the internet or from other databases and electronic patient journals. It is also directly connected to the Swedish National Population Registry for immediate access to personal data and deaths. There are approximately 2700 registered users, mainly physicians and nurses.
What is recorded
For patients admitted to hospital because of symptoms suggestive of ACS information is collected prospectively for 106 variables and includes patient demographics, admission logistics, risk factors, past medical history, medical treatment before admission, electrocardiographic changes, biochemical markers, other clinical features and investigations, medical treatment in hospital, interventions, hospital outcome, discharge diagnoses and discharge-medications. For patients younger than 75 years who have been hospitalised for acute MI a follow-up is performed after 6–10 weeks and after 12–14 months, including the addition of approximately 75 variables. For this rehabilitation and secondary prevention part, information about smoking habits, blood pressure, lipd levels, physical activity, cardiac symptoms, quality of life, hospital readmission, medication and participation in secondary preventive programmes is recorded. For assessment of quality of life the standardised quality of life measurement instrument, EQ-5D, is used.1 For patients undergoing coronary angiography/angioplasty for any clinical indication approximately 150 variables are registered. Besides baseline characteristics, the registry includes a detailed description of angiographic findings, procedures, type of stenosis, type of stent, antithrombotic treatment and complications. The system has an interactive method for the registration of restenosis and stent thrombosis. Detailed information about every previously implanted stent anywhere in the country is presented and a mandatory question about the existence of any form of restenosis or stent thrombosis has to be answered. For patients operated for cardiac or thoracic aortic disease more than 100 variables, including demographic data, EuroSCORE (European System for Cardiac Operative Risk Evaluation), detailed information on coronary bypass and valve procedures and postoperative complications, are reported.2
Merging the database with other registries
Every Swedish citizen has a unique personal identification number, which together with name, address and hospital identity, is included in the registry. All patients are informed about their participation in the registry and the follow-up, and have the right to decline participation. The system has an advanced password protection and the user can only see patients from its own hospital. For security purposes, every user activity is logged. The use of a personal identification number enables the continuous identification of the individual patient throughout all care processes and registries in Sweden. After regulatory approval the SWEDEHEART database is, on a yearly basis, merged with the National Cause of Death Register, including information about vital status of all Swedish citizens, and the National Patient Registry, containing diagnoses at discharge for all hospital stays in Sweden, and finally with the National Registry of Drug prescriptions recording all drug prescriptions in Sweden. It is also possible for researchers to apply for access to data from other registries for use in specified research projects. At the merging of the registries, patient identity is removed from the database. Every merge of data from the different registries is performed by the National Board of Health and Welfare after approval of the local ethics committee at Uppsala University. The merged database can only be used in prespecified research projects approved by the SWEDEHEART steering committee and the local ethics committee. It is kept in the custody of the section of statistics and epidemiology at Uppsala Clinical Research Centre.
Data quality
Uppsala Clinical Research Centre provides manuals, education and technical advice, including a telephone help desk for all users of the registry. The system has error checking routines for range and consistency. Definitions are displayed on the screen when data are entered. To ensure the correctness of the data entered a monitor visits approximately 20 randomly selected hospitals each year and compares data entered into SWEDEHEART with the information in the patients' records in 30–40 randomly chosen patients for each hospital. When 637 computer forms from 21 hospitals containing 38 121 variables were reviewed for RIKS–HIA in 2007, there was 96.1% (range 92.6–97.4%) agreement. To reach a high degree of completeness a majority of variables are mandatory and each hospital can monitor data completeness. The registry captures 100% of the patients undergoing angiography, angioplasty or heart surgery. When compared with the National Patient Registry, 60% of patients with acute MI are captured by the SWEDEHEART registry with a large variation between hospitals. The main reason for that is that some ACS patients are admitted to other units than coronary care units. The degree of patient capture is higher in younger patients and in those with ST-elevation MI.
Use of SWEDEHEART data
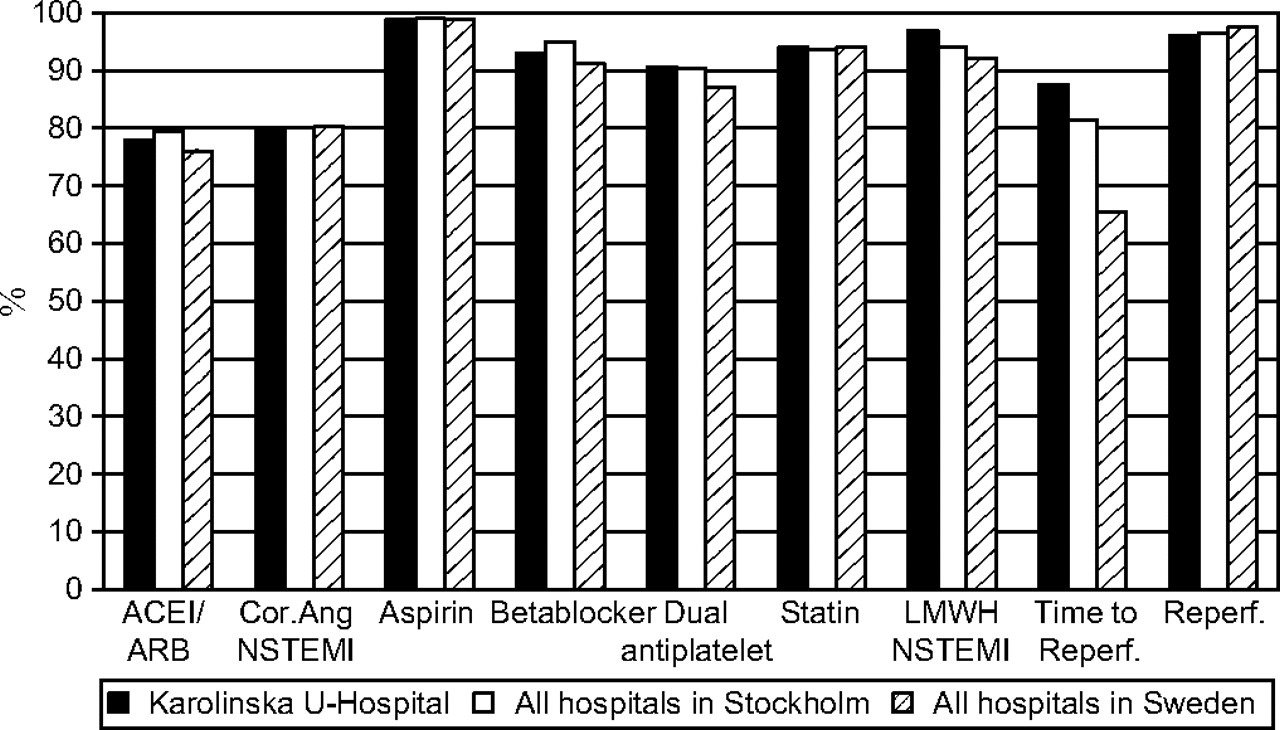
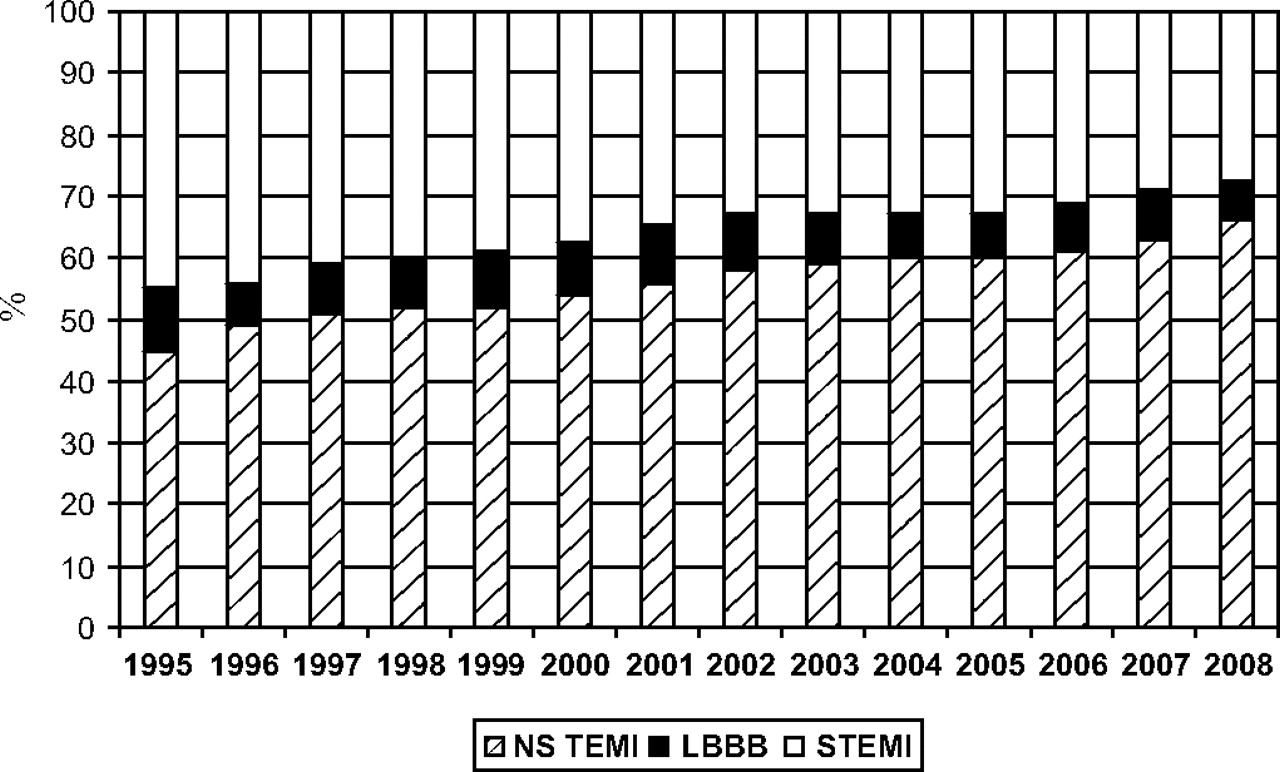
The main purpose is to support the improvement of care by providing information on care needs, given therapies and outcome. The long-term goals are to contribute to decreased mortality and morbidity and to improve cost effectiveness in coronary care. The system provides all users (physicians, nurses and local decision-makers) with an array of online interactive reports continuously monitoring the processes of care and outcomes. It allows direct comparisons over time and with other hospitals (figure 1). For percutaneous coronary intervention patients the system displays detailed information about any previously performed intervention. The system is also capable of producing reports summarising the findings, treatments and interventions that may be printed and included as a part of the patient's clinical files. National, regional and county-based reports are presented on a yearly basis showing all these levels openly concerning a large number of variables. These reports also report about trends over the years with regard to presentation, treatment and outcome (figures 2, 3 and 4). The registry can compare not only the performance of participating hospitals but also different treatment modalities and medical devices. The publicly presented results, especially concerning differences in the standards of care between different hospitals and regions and concerning the adherence to national guidelines, have also been associated with wider professional and public attention. The following discussions in different media and authorities have most likely contributed to the improvements in the standards of care. In addition, many hospitals are engaged in collaborative projects on quality development, which are supported by the online interactive reporting system as a continuous tool for quality development.3 4

Example of bench-marking. Proportion of patients who actually received treatment according to national guidelines. Karolinska University Hospital in comparison with other hospitals in Stockholm and with other hospitals in Sweden. ACEI/ARB, ACE inhibitor/angiotensin receptor blocker; Cor.Ang, coronary angiography; LMWH, low molecular weight heparin; NSTEMI, non-ST-segment elevation myocardial infarction; Reperf., reperfusion therapy; Time to reperf, proportion of ST-segment elevation myocardial infarction patients with time from first ECG to reperfusion therapy according to guidelines.

Type of acute myocardial infarction (with permission from SWEDEHEART Annual Report 2008). LBBB, left bundle–branch block; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.

Reperfusion therapy in ST-elevation myocardial infarction (with permission from SWEDEHEART Annual Report 2008). CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mortality after an acute myocardial infarction in patients 60–69 years of age (with permission from SWEDEHEART Annual Report 2008).
The registry has been an important source of data for research. Hospitals have direct access to their own data, which may be used for further local analyses. Academic researchers who want to pursue questions in the whole national database can apply for specific analyses, which will be performed after acceptance from working groups and the steering committee. Groups that are granted approval must have shown progress within 1 year by presenting an abstract at a meeting, and within 2 years by submitting a manuscript for publication in order to maintain priority for the specific project. SWEDEHEART and its original four registries have, so far, been the source of more than 60 original papers, of which several have been in high-ranking journals.5–29 A policy for the use of data for research sponsored/financed by pharmaceutical or device companies will be established during 2010.
Strengths and weaknesses
The registry has several strengths. Despite the fact that there is no legal requirement for hospitals to participate, it includes consecutive patients at all Swedish hospitals providing acute cardiac care or cardiac interventions. The coverage is 100% for patients undergoing angiography, angioplasty and cardiac surgery, 60% for all ACS cases and almost 100% for ACS patients admitted to coronary care units. It is a web-based registry and data are registered online and the system provides all users with online interactive reports concerning changes of processes of care and outcome in direct comparison with other hospitals. The yearly report is publicly open with regard to hospital identity and is an important tool for decision-makers. The use of personal identification numbers enables long-term follow-up with regard to both mortality and morbidity. The secondary prevention part provides data regarding both symptoms and quality of life.
There are also some weaknesses. Comparisons between hospitals can be difficult to interpret for some inherent reasons. The coverage of MI patients below 80 years of age varies between hospitals from 55% to 95%, mainly because not all ACS patients are admitted to a coronary care unit. Moreover, in comparisons between different hospitals and regions the outcome may differ due to differences in baseline characteristics, age structure or socioeconomic factors in the catchment areas. The steering committee of SWEDEHEART is well aware of these limitations and is trying to ensure the enrolment of all comers with acute coronary syndromes in the RIKS–HIA part. The report of 2010 will include data regarding coverage for each participating hospital. There is also a group working with case-mix analyses in an attempt to adjust for some of the differences between the hospitals. Still, the interpretation of studies comparing differences in outcome between different sites or different treatment alternatives must be done with great caution, which is not always the case in media. The funding of the registry is stable but insufficient. The data collection is financed by the participating hospitals, but most members of the working groups and steering committee do not receive any economic compensation.
Future directions and developing platforms
The registry will be expanded during 2010 to include all cases of percutaneous aortic valve procedures as a separate section. This section will be similar to the SCAAR and surgery sections in order to make it possible to compare resources, patient characteristics and outcomes of open valve surgery compared with percutaneous valve implantations. Currently, pilot centres have started to accumulate plasma and whole blood samples connected to the database. Hopefully these modules can shortly be expanded to accumulate a large-scale national biobank for proteomic and genomic information, which can be related to the clinical information. A randomisation module is under development, which will enable the performance of large-scale randomised registry-based trials of all comer populations. The first randomised study is designed to evaluate mortality after primary percutaneous coronary intervention with or without thrombus aspiration performed before direct stenting in 5000 patients. Further development includes a platform for patient self-reporting regarding quality of life and physical status. This will allow a broad collection of important soft endpoints after all types of ACS care and cardiac interventions.
Another important future development is to integrate the registry with the different electronic patient record systems used in Sweden in order to allow data capture direct from the electronic patient record, and thus minimise the extra work with entering data separately in the register over the web.
Conclusions
SWEDEHEART is the result of two decades of development of registries on coronary artery disease in Sweden. Today, it is an integrated part of the routine care of coronary artery disease patients at all Swedish hospitals. It has proved to be an important tool for the improvement of care and a rich source of data for research.
Acknowledgments
The RIKS–HIA registry was initiated in 1991 by Drs Ulf Stenestrand, Linköping University Hospital and Lars Wallentin, Uppsala University Hospital, Sweden, in collaboration with the user group of participating hospitals. This registry was extended in 2005 by adding the SEPHIA registry under the leadership of Drs Bertil Lindahl, Uppsala University Hospital and Patrik Tydén, Malmö University Hospital. The SCAAR registry was initiated in 1998 by a merge of two separate registries of angiography and angioplasty by Per Albertsson, Sahlgrenska University Hospital, Göteborg and Tage Nilsson, Karolinska University Hospital, Stockholm in collaboration with the user group. The cardiac surgery registry was initiated in 1992 by Dr Kjell Rådegran, Karolinska University Hospital, Stockholm under the auspices of the Swedish Society of Thoracic Surgery. The initiative to merge the four registries came from the chairmen of the registries and was supported by the participating hospitals.
References
Footnotes
Ulf Stenestrand died on 11 February 2010.
Funding The Swedish Association of Local Authorities and Regions.
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.