Article Text

Abstract
Background Small studies suggest that postconditioning reperfusion interrupted by brief repetitive cycles of reocclusions, may protect the myocardium in the clinical setting.
Objective To test the hypothesis that postconditioning limits infarct size in relation to the area at risk in patients with ST elevation myocardial infarction (STEMI).
Methods 76 patients (aged 37–87 years) eligible for primary percutaneous coronary intervention due to STEMI were randomised to standard percutaneous coronary intervention (n=38) or postconditioning, consisting of four cycles of 60 s reperfusion and 60 s of reocclusion before permanent reperfusion (n=38).
Results The area at risk was determined from angiographic abnormally contracting segments. Infarct size was quantified from delayed enhancement MRI on days 6–9. Infarct size, expressed in relation to the area at risk, did not differ between the control group (44%; 30, 56) (median and quartiles) and the post-conditioned group (47%; 23, 63). The slope of the regression lines relating infarct size to the area at risk differed between the two groups. Infarct size was significantly (p=0.001) reduced by postconditioning in patients with large areas at risk. The area under the curve and peak troponin T release and CKMB during 48 h did not differ between patients in the control and postconditioning groups.
Conclusions This prospective, randomised trial suggests that postconditioning does not reduce infarct size in patients with STEMI in the overall study group. The data indicate that postconditioning may be of value in patients with large areas at risk.
Clinical trial registration information Karolinska Clinical Trial Registration (http://www.kctr.se). Unique identifier: CT20080014.
- Myocardial infarction
- postconditioning
- reperfusion injury
- MRI
- coronary intervention
- coronary artery disease (CAD)
- STEMI
Statistics from Altmetric.com
- Myocardial infarction
- postconditioning
- reperfusion injury
- MRI
- coronary intervention
- coronary artery disease (CAD)
- STEMI
Early reperfusion is a prerequisite for the effective salvage of ischaemic myocardium and reduces morbidity and mortality in patients with ST elevation myocardial infarction (STEMI).1 2 Despite successful primary percutaneous coronary intervention (PCI) many patients develop large myocardial infarcts. Infarct size is an important determinant of short and long term outcome,3 and it is essential to develop therapies that limit the extent of the final myocardial injury. Reperfusion relieves ischaemia but at the same time initiates a series of harmful events, including release of highly reactive free oxygen species which greatly contributes to the final myocardial injury.4 This tissue damage is referred to as reperfusion injury. Ischaemic but still viable myocardium may undergo lethal injury during the very early phase of reperfusion. Importantly, reperfusion also offers a window for intervention with the purpose of limiting the extent of the final myocardial injury. The timing of such an intervention is crucial since the reperfusion injury develops within the first minute after the onset of reperfusion.5
Myocardial tissue can be preconditioned by brief cycles of ischaemia and thereby becomes resistant to the negative effects of a prolonged ischaemic insult.6 Since ischaemic preconditioning must be established before coronary artery occlusion it is of limited use as acute treatment in patients with STEMI. An important experimental observation is therefore that ischaemic myocardium may be protected even by postconditioning—that is, reperfusion followed by repeated cycles of brief reocclusion before permanent reperfusion,7 a procedure that is clinically feasible. Interference with the cascade of harmful events initiated by reperfusion either by pharmacological interventions8 or postconditioning7 significantly reduces final infarct size in experimental studies. Postconditioning in dogs reduced infarct size in relation to area at risk by 44%, an effect that was comparable to that induced by preconditioning. Subsequent studies performed in several different species confirmed these findings.9
Previous studies have shown that the release of creatine kinase was significantly reduced by postconditioning in patients with STEMI.10 11 Furthermore, the absolute infarct size, determined by single-photon CT (SPECT), was smaller in patients subjected to postconditioning.12 13 Although area at risk was determined by Thilbault et al,12 infarct size was not related to the initial risk area, which is of importance when determining the treatment effect. Lønborg et al14 recently reported that postconditioning reduced infarct size in patients with STEMI when evaluated with MRI 3 months after the event. They determined the area at risk from the same images but did not evaluate this area before reperfusion. Thus, it remains to be determined whether postconditioning affects infarct size in relation to the area at risk as depicted before reperfusion. The present study was designed to test the hypothesis that postconditioning, in connection with primary PCI, limits the infarct size in relation to the initial area at risk in patients with STEMI.
Methods
Study group
Patients admitted to the coronary care unit at Karolinska University Hospital planned for a primary PCI due to STEMI were eligible for enrolment if they fulfilled the following inclusion criteria: chest pain >30 min and ≤ 6 h, ST elevation ≥0.1 mV (≥0.2 mV in V1–V3) in two contiguous ECG leads or left bundle branch block, and a thrombolysis in myocardial infarction (TIMI) grade 0 flow in the infarct related artery.15 Exclusion criteria were previous myocardial infarction, previous coronary artery bypass surgery, cardiogenic shock, cardiac arrest, known renal impairment (serum creatinine >150 μmol/l), ongoing treatment with metformin, contraindication for MRI, persistent atrial fibrillation, and any condition that was considered to interfere with the possibility for the patient to complete the study protocol.
The study was performed according to the Declaration of Helsinki16 and good clinical practice. Written informed consent was given by all patients. The study was approved by the local ethics committee at the Karolinska Institutet.
Study design and procedures
This study was conducted as a prospective randomised open study with blinded evaluation (PROBE design). All patients received aspirin 320–500 mg and clopidogrel 300–600 mg orally if not already on such medication, and enoxaparin 40 mg intravenously. A coronary angiography was performed to confirm TIMI 0 flow in the infarct related artery using iodixanol (Visipaque, GE Healthcare, Princeton, New Jersey, USA). Abciximab was given as a bolus (0.25 mg/kg) followed by a 12 h continuous infusion (0.125 μg/kg/min). In order to determine area at risk, biplane left ventriculography was performed before revascularisation. Following these procedures the patients were randomised to primary PCI only or PCI followed by postconditioning (supplementary figure 1). Postconditioning was performed by reinflating the balloon at the same location to a pressure of 2–4 atm for 60 s starting 60 s after the initial reperfusion. This cycle was performed four times according to a protocol used in previous experimental and human studies.10 17 18 Postconditioning was performed with the same balloon catheter as the one used for the initial inflation. The PCI intervention was completed by a coronary angiogram to study the final TIMI flow. Collateral flow to the infarct zone was assessed on the initial angiogram before PCI and graded on a scale of 0 to 3.19
Investigations and measurements
Angiographic determination of area at risk
Myocardial area at risk was estimated by measuring the circumferential extent of abnormally contracting segments.20 Left ventriculography (30° right anterior oblique, 60° left anterior oblique) was performed immediately before coronary angioplasty during infusion of 40 ml of contrast (12 ml/s). An x-ray digital imaging software system (Integris HM 3000, Philips, The Netherlands) was used for global and regional left ventriculogram analysis. Global ejection fraction was calculated by the area–length method. Centreline chord motion analysis was used to quantitatively assess regional left ventricular (LV) function. In this technique, endocardial motion is measured along 100 chords constructed perpendicular to a centreline. The motion of each chord is normalised by the end-diastolic circumference to yield a fractional shortening. This value is then converted into units of SD from the normal mean motion of each chord as derived from a normal reference population. Wall motion was analysed in the distribution territory of the left anterior descending artery (10 to 66 chords) in patients with anterior infarctions, and in the distribution territory of the right or circumflex coronary arteries (51 to 80 chords) in patients with inferior infarctions. Abnormal wall motion extent was defined as the number of chords displaying hypokinetic motion (<1 SD) expressed as a percentage of the LV volume. These measurements were performed by two experienced investigators unaware of the group to which the patient belonged.
Infarct size
A standard MRI was scheduled 1 week after the onset of symptoms. These investigations were performed in the supine position with an eight-channel cardiac coil by means of an 1.5 T system (Signa Excite TwinSpeed, General Electric Healthcare, Waukesha, Wisconsin, USA) during vector-ECG monitoring. Gadolinium contrast (0.2 mmol/kg; Omniscan, GE Healthcare) was administered before positioning the patient in the scanner. The image protocol included scout images, localisation of the short axis and then covering the whole LV with retrospectively gated cine steady-state free precession (SSFP) images. The following parameters were used; SSFP (echo time (TE) 1.58 ms, repetition time (TR) 3.61 ms, flip angle 60°, 25 phases, 8 mm slice, no gap, matrix 226×226). Delayed-enhancement images were acquired 15–20 min after contrast injection using an inversion recovery gradient echo sequence (TE 3.3 ms, TR 7.0 ms, inversion time 180–250 ms to null the myocardium, 8 mm slice, no gap, matrix 256×192) and the same slice orientation as cine SSFP images.21 22 Cardiac triggering was set for diastole to reduce motion artefacts. Each slice was obtained during end-expiratory breath holding. Two-, three- and four-chamber views were also obtained to confirm the findings. MR images were analysed off-line using freely available segmentation software (Segment V.1.8 R0857; http://segment.heiberg.se/). End-diastolic and end-systolic volumes, ejection fraction, stroke volume and left ventricular volume were calculated on cine SSFP sequences. Infarct size was quantified using an automated quantification method that has been validated ex vivo and in vivo in which partial volume effects are accounted for.23 Using this algorithm the intra- and inter-observer variation between two blinded readers was 0.0±3.5% and 0.7±1.1% (bias and SD), respectively.
Blood sampling
Troponin T was analysed with an immunoassay (Modular Analytics E-module, Roche Diagnostics) and CKMB (creatine kinase, myocardial bound) by a chemiluminescence technique (UniCel DxI 800, Beckman Coulter AB). Sampling was performed at admission and every 4 h during the first 24 h after reperfusion and every 6 h until 48 h. Both peak values and the area under the curve (AUC) were determined. An oral glucose tolerance test was performed on day 3–5.
Statistical methods
The primary endpoint of this study was infarct size on day 6–9 expressed as percentage of the area at risk. Secondary endpoints were global left ventricular function, release of cardiac biomarkers during the 48 h following the coronary intervention and TIMI flow after completed angioplasty. Based on an expected reduction in infarct size of 20% and SD of 30%,18 36 patients were needed in each group to achieve p<0.05 with a power of 80% and a two-tailed test. To compensate for patient dropout a total number of 90 patients were planned to be recruited. Computer-generated randomisation in blocks of eight was performed following stratification for left anterior descending coronary artery (LAD) and non-LAD occlusions.
All data are presented as medians and 25th, 75th percentiles. The Mann–Whitney U test was used to test for differences in infarct size and cardiac biomarkers between groups. Fisher's exact test was used to test for differences between dichotomised variables. Linear regression was used for comparing infarct size in relation to the area at risk between groups, and regression analysis was performed with four residuals looking at the best equation. Bland–Altman plots were constructed for comparing intra- and inter-observer variability (n=20) and calculated as the SD of the difference between two calculations divided by the average of the two observers. Statistical analysis was performed using GraphPad Prism V.5.00 (GraphPad Software, San Diego, California, USA).
Results
Study group
During the study period a total of 795 patients were referred to the coronary care unit for a PCI due to STEMI. As figure 1 shows, 89 patients were randomised and 76 completed the study protocol. As can be seen from tables 1 and 2, the two groups were well balanced regarding clinical characteristics and angiographic findings. The postconditioning procedure was well tolerated.
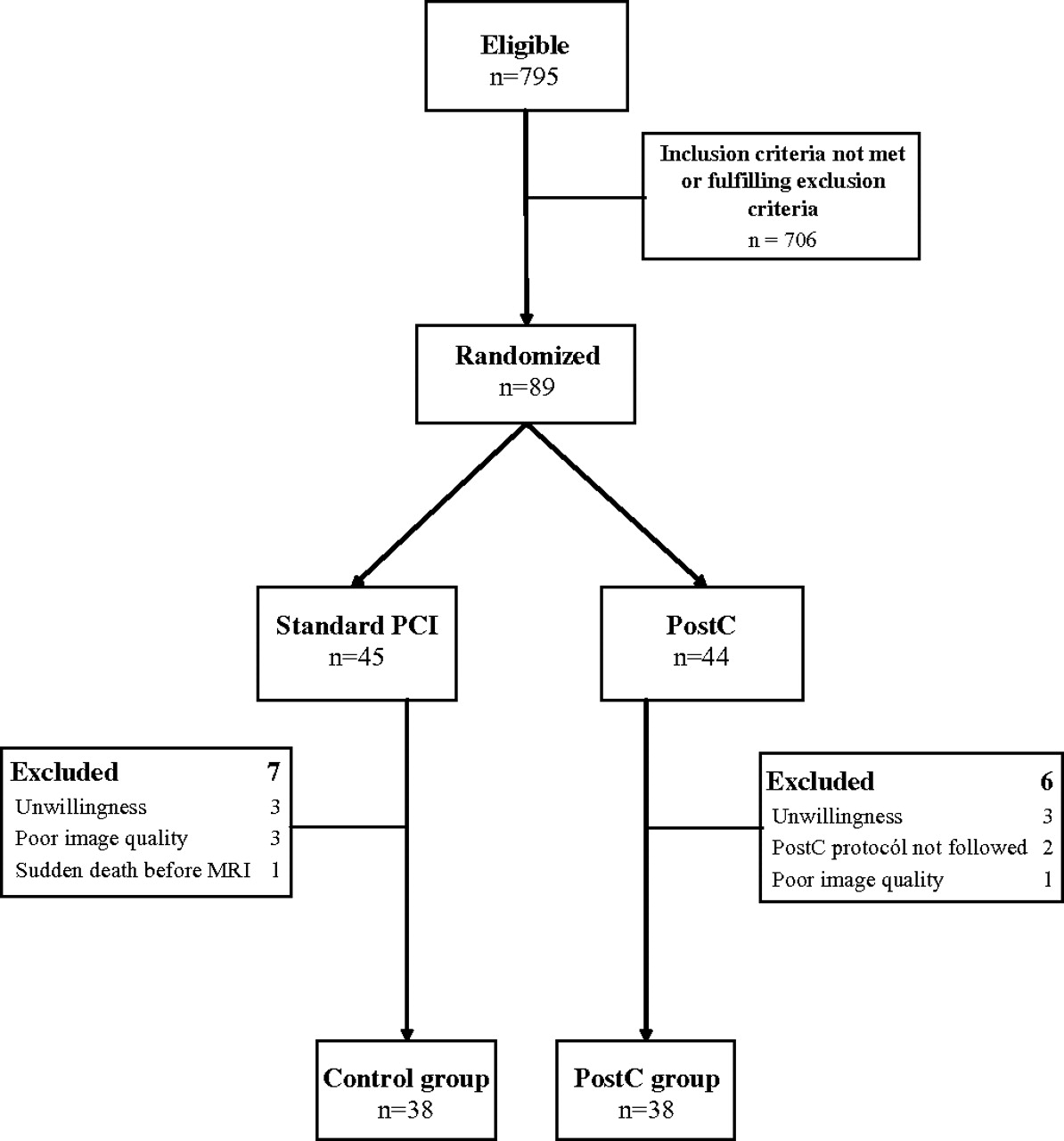
Patient flow chart. PCI, percutaneous coronary intervention; PostC, postconditioning.
Patient characteristics in the control and postconditioning groups
Angiographic data
Infarct size and left ventricular ejection fraction
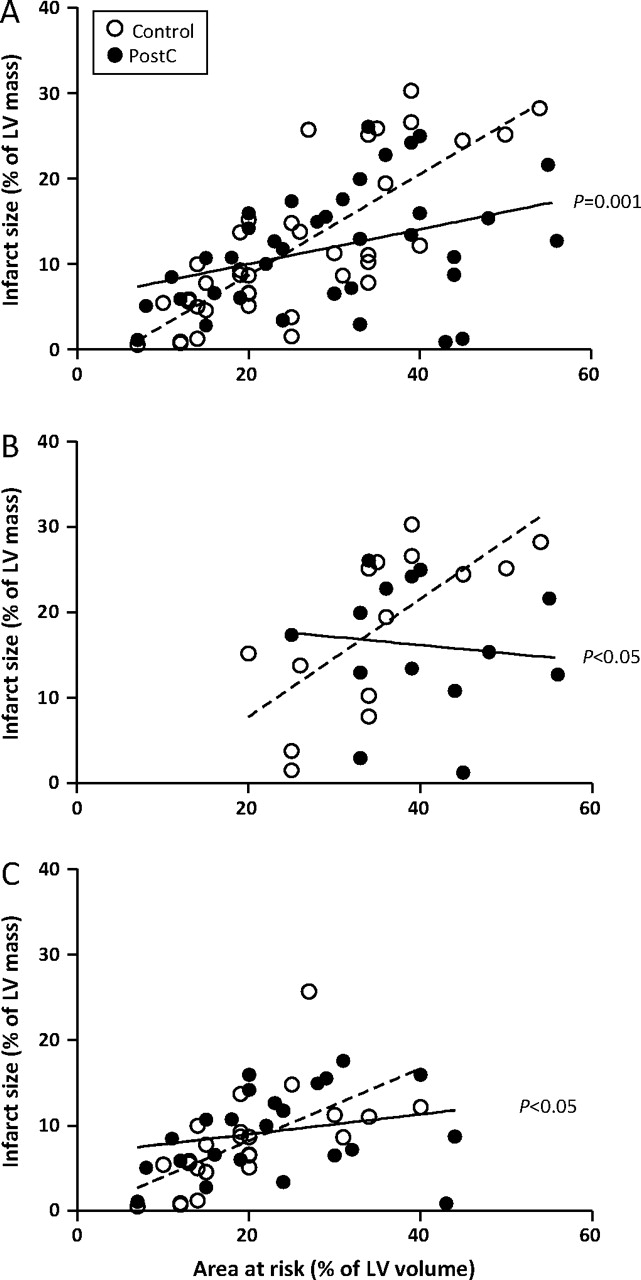
Infarct size, presented as a percentage of the area at risk (figure 2), was not significantly different between the two groups (control: 44% (30, 56); postconditioning: 47% (23, 63)). The regression analysis in which the final infarct size was related to the myocardial area at risk showed a significant difference between the two groups (figure 3A). Patients belonging to the postconditioning group with areas at risk exceeding 30% of the left ventricle had smaller final infarct sizes than the corresponding control patients. Similar results were obtained when analysing LAD and non-LAD related infarctions separately (figure 3B,C). In the multiple regression analysis the infarct size was significantly related to postconditioning and area at risk (p=0.001) but not to age, sex, ischaemic time or smoking habits. Final infarct size in patients with areas at risk in the upper quartile was 54% (50, 68) among those belonging to the control group and 33% (21, 57) among postconditioning patients (p=0.03). In contrast, there were no significant differences in patients within the lower quartiles (data not shown).
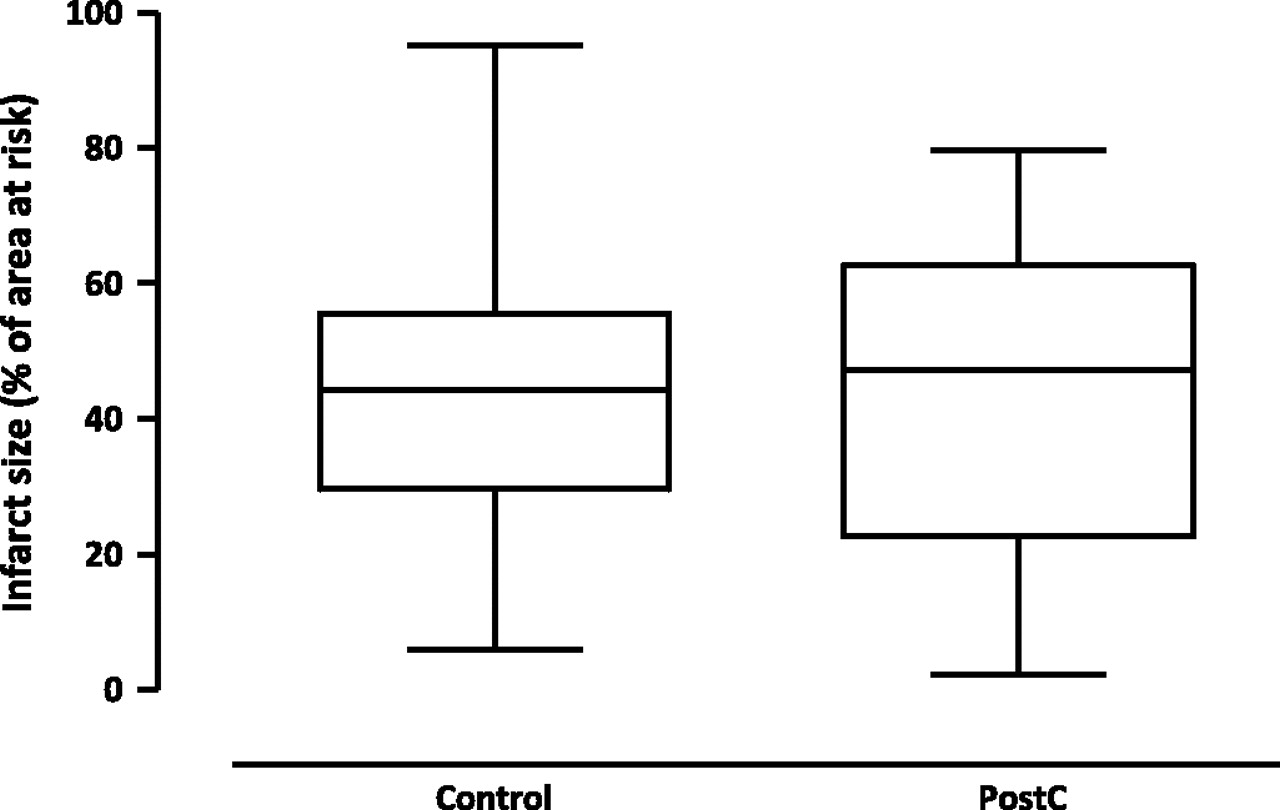
Infarct size in relation to the myocardial area at risk. Infarct size did not differ significantly between patients in the control and postconditioning groups. PostC, postconditioning.
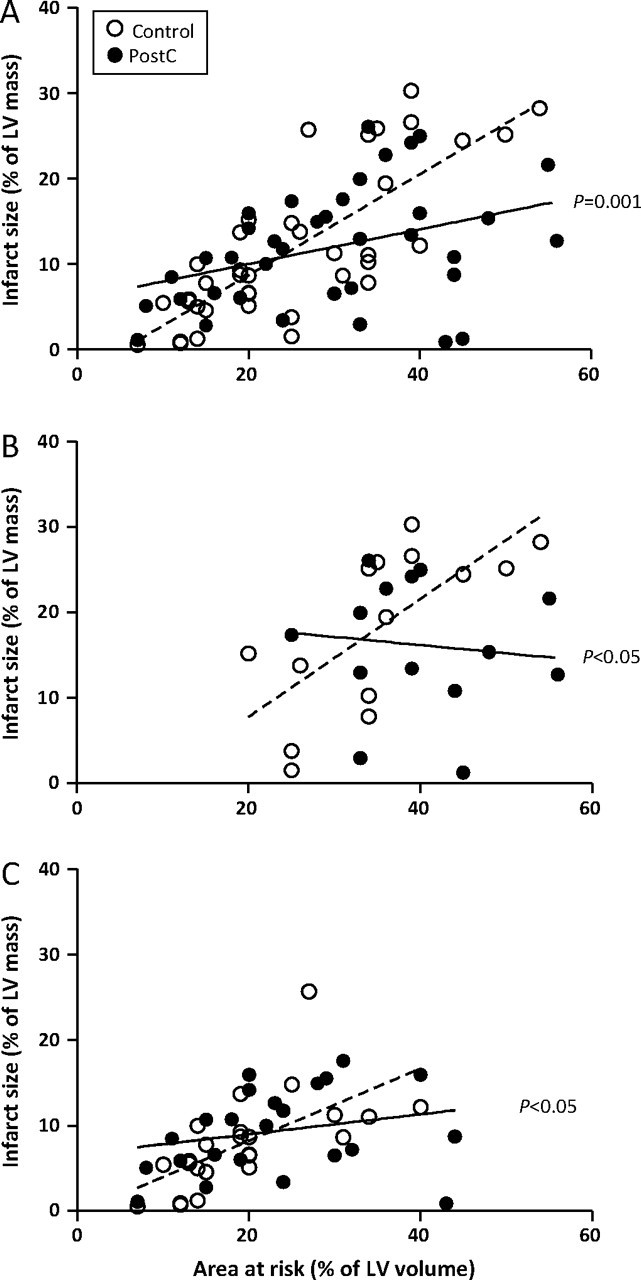
Infarct size plotted against myocardial area at risk: (A) for the overall study population; (B) in patients with LAD infarctions; and (C) in patients with non-LAD infarctions. There are significant differences between the slopes of the regression lines between patients in the control and postconditioning groups. LV, left ventricular.
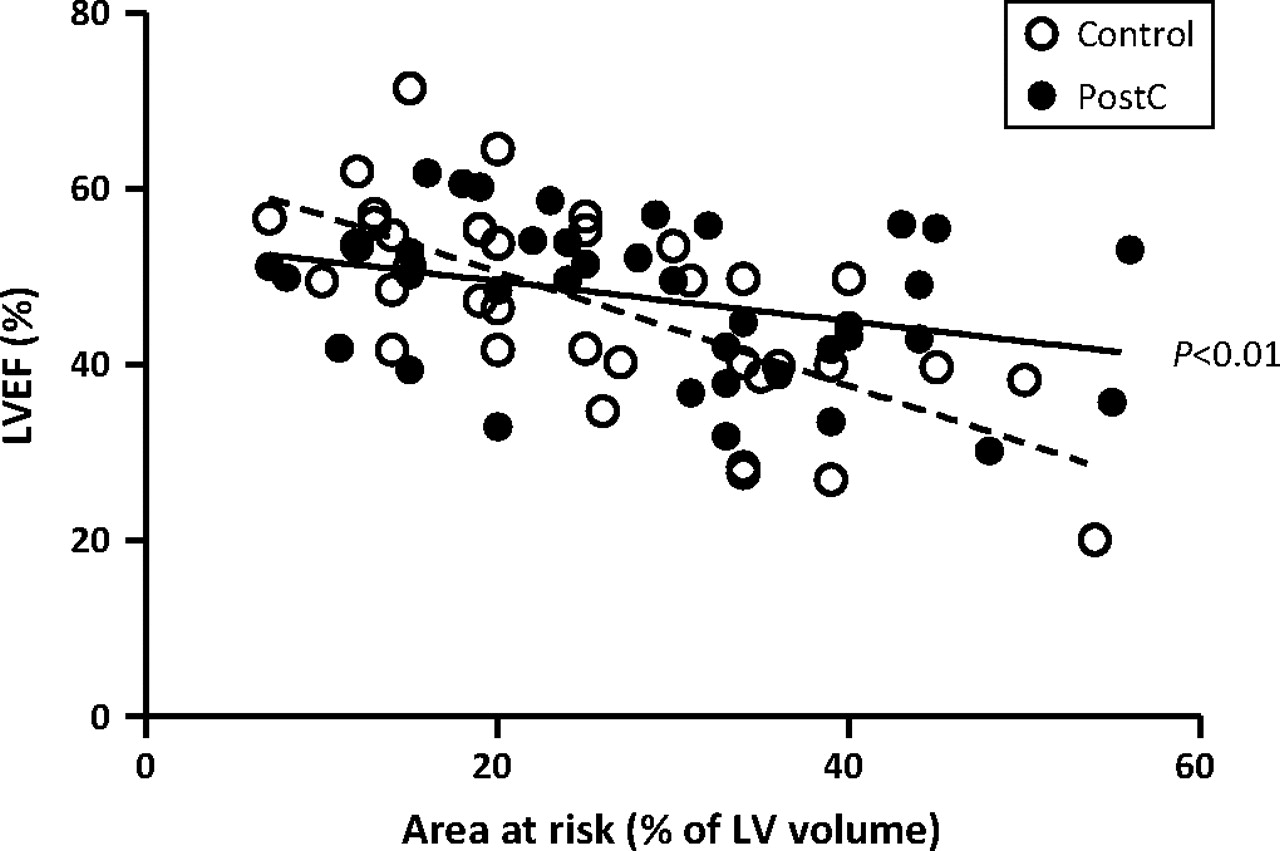
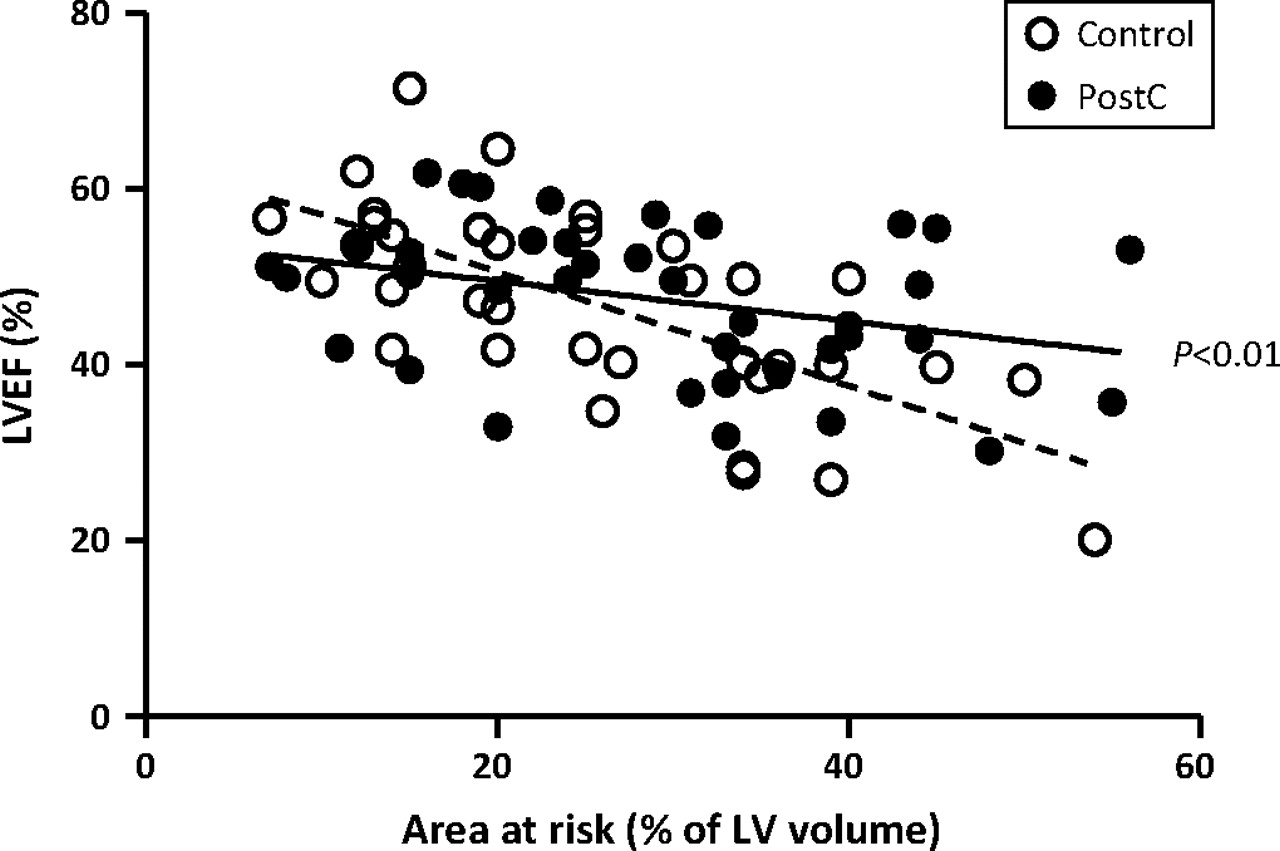
Median left ventricular ejection fraction (LVEF) determined by MRI on day 6–9 did not differ between the control and postconditioning groups: 50% (40, 55) and 50% (41, 54), respectively. Similar to the findings regarding infarct size, there was a significant difference in the slopes of the regression lines. LVEF was higher in the postconditioning group compared with the control group among patients with large areas at risk (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Left ventricular ejection fraction (LVEF) determined with MRI and plotted against myocardial area at risk. There is a significant difference between the slopes of the regression line between patients in the control and postconditioning groups.
Cardiac biomarkers
Troponin T and CKMB (AUC or peak values) did not differ between the control and postconditioning groups. AUC for troponin T was 147 (80, 269) and 165 (95, 279) in the control and postconditioning groups, respectively. AUC for CKMB was 3890 (2388, 6264) and 4175 (2406, 6060) in the two groups.
Discussion
This prospective randomised study evaluating the effect of postconditioning in patients with STEMI did not show any significant difference in infarct size in relation to the myocardial area at risk in the overall study group. However, postconditioning may be of benefit in patients with large myocardial areas at risk.
An obvious advantage with postconditioning is that it can be applied in patients with STEMI undergoing primary PCI. The first groups to report on such protocols were Staat et al11 and Laskey et al10 24 who showed that postconditioning reduced the release of CK, a surrogate marker for infarct size, and improved coronary flow reserve and ST resolution. Thibault et al showed that postconditioning reduced absolute infarct size evaluated with SPECT and improved LVEF in a study of 38 patients with STEMI, but did not relate infarct size to the initial myocardial area at risk.12 This is important in particular when studying small populations.25 In this perspective the recent report by Lønborg et al that postconditioning resulted in a 19% relative reduction of infarct size in relation to the area at risk, is of considerable interest.14
In the present study infarct size, quantified by an automatic MRI algorithm, was related to the myocardial area at risk determined by left ventriculography.10 In contrast to previous reports postconditioning did not influence the infarct size in the overall study group. Interestingly, the slopes of the regression lines differed significantly between the control and the postconditioning groups when infarct size was analysed as a function of the area at risk. Thus, infarct size was smaller in the postconditioning patients within the upper quartile of area at risk in patients with both LAD and non-LAD related infarctions. LVEF also differed, supporting a beneficial effect of postconditioning in patients with large areas at risk. According to the regression analysis a protective effect of postconditioning appeared detectable for areas at risk exceeding 30%. In the light of this observation it is important to note that the left ventricular area at risk, determined from abnormally contracting segments in previous studies,10 12 was 35–40%, which should be compared to 25% in the present study. Collectively these data support the conclusion that postconditioning is protective, especially in patients with large areas at risk.
Additional differences of potential importance between the various studies evaluating the effect of postconditioning deserve to be discussed. In the present study, MRI on day 6–9 was used to determine infarct size, in contrast to 612 and 3 months14 in previous studies. The reason to determine infarct size after 1 week was to limit the influence of LV remodelling which may affect infarct size. Since the reduction of the hyperenhanced area is greatest during the first week,26 determination of infarct size after approximately one week seems optimal, balancing the early disappearance of the increased area of hyperenhancement against LV remodelling. Moreover, infarct size was expressed in relation to the area at risk determined at admission during occlusion of the infarct-related artery. In contrast, Lønborg et al14 estimated the area at risk from an MRI performed 3 months after reperfusion. There is a possibility that LV remodelling during this time period influenced the relation between the area at risk and LV volume. To avoid any influence of spontaneous reperfusion, only patients with TIMI 0 flow were included in the present study, in contrast to previous studies that included patients with TIMI grade 0–1.12 14 Finally, the present postconditioning protocol was four cycles of 60 s reperfusion and 60 s reocclusion. This is similar to the protocol used by Thibault et al12 but different from that applied by Lønborg et al.14 Although original observations suggested that brief cycles are optimal in small animal models (mice and rats), longer periods (30–60 s) may be more effective in larger species (pigs).9 A subsequent analysis could not delineate an optimal postconditioning protocol.27 Still, it seems as if cycles of 60 s were more effective in decreasing the release of apoptotic markers than cycles of 30 s in patients with STEMI.28
Postconditioning may protect the myocardium via multiple mechanisms.29 Experimental data support involvement of the reperfusion injury salvage kinase (RISK) pathway,30 the survivor activating factor enhancement (SAFE) pathway31 and the activation of protein kinase G.32 These pathways may all eventually result in prevention of opening of the mitochondrial permeability transition pore (mPTP).33 The RISK pathway includes activation of the prosurvival kinase Akt, extracellular regulated kinase 1/2 (ERK 1/2), mitochondrial KATP channel activation and finally prevention of mPTP opening. The SAFE pathway also prevents the opening of mPTP via activation of cytokine tumour necrosis factor α and the transcription factor signal transducer and activator transcription-3 (STAT-3). The mechanism of importance in the clinical situation remains to be established.
Study limitations
The size of the study population may have been too small for the detection of minor benefits of postconditioning. The number of patients was based on a power calculation assuming an absolute reduction of infarct size by 20% of the area at risk. This effect was not reached. In this perspective it is reassuring that postconditioning exerted a beneficial effect in patients with large risk areas. Although not directly transferrable to the general group of STEMI patients, this finding is of considerable interest and worthy of future evaluation. Besides postconditioning the extent of the final infarct size may depend on several factors which are difficult to control in a clinical study.4 These include age, comorbidities, medication, pre-infarction angina known to precondition the myocardium as well as presence of collaterals. The groups were well matched regarding these factors, suggesting little impact on the primary endpoint.
Conclusions
This prospective and randomised trial suggests that postconditioning does not reduce infarct size in patients with STEMI in the overall study group. However, the data indicate that postconditioning is protective in patients with large areas at risk. The combined impression of studies performed so far is that postconditioning is a promising technique in need of further exploration. Such studies should probably focus on patients with large risk areas.
Acknowledgments
We are grateful to Kerstin Höglund RNS and Eva Wallgren BMA for their skilled patient management, and to Marie Lundberg and Yords Österman RNS for their excellent technical support during the MRI investigations. We also acknowledge the statistical advice given by associate professor John Öhrvik. This study could not have been conducted without the devoted work of the staff of the catheterisation laboratory.
References
Footnotes
Funding Swedish Heart-Lung Foundation, Swedish Research Council of Medicine (10857, 14231), Stockholm County Council.
Competing interests None.
Ethics approval The study was approved by the local ethics committee at the Karolinska Institutet, Stockholm.
Provenance and peer review Not commissioned; externally peer reviewed.