Article Text

Abstract
Objective To assess whether prehospital initiation of high-dose tirofiban in addition to high-dose clopidogrel results in more adequate inhibition of platelet aggregation (IPA) and better clinical outcome after primary percutaneous coronary intervention (PCI).
Methods Prespecified two-centre substudy of the prospective, international, multicentre, placebo controlled Ongoing Tirofiban in Myocardial Infarction Evaluation trial 2 (On-TIME-2 trial). 648 of 964 (67%) patients in the On-TIME-2 trial with ST elevation myocardial infarction undergoing primary PCI were studied. Pre-PCI IPA after early prehospital initiation of high-bolus dose (25 μg/kg) tirofiban was compared to placebo in addition to acetylsalicylic acid, unfractionated heparin and 600 mg clopidogrel.
Results IPA was measured at a median of 60 min after study medication administration. In all four tests: Fe induced platelet aggregation, ADP induced platelet aggregation, platelet function analyser (PFA)-100 (collagen–epinephrine and collagen–ADP cartridge) IPA was higher in patients pretreated with high-dose tirofiban (p<0.001 for all tests), even after >74 min of pretreatment. Patients in the highest quartile of IPA had less residual ST segment deviation 1 h post-PCI (p value for trend: p=0.001, 0.004, 0.001, 0.002 respectively). There was a significant relationship between PFA-100 (both cartridges) and major adverse cardiovascular events (MACE, p=0.028, p=0.035) and early thrombosis (p=0.009, p=0.007).
Conclusions 60 min of prehospital initiated antiplatelet treatment including high-dose tirofiban resulted in higher levels of IPA compared to pretreatment with acetylsalicylic acid and high-dose clopidogrel alone, even after longer pretreatment times. Levels of IPA were significantly related to ST resolution and MACE, including stent thrombosis. This substudy confirms the main findings of the On-TIME2 trial that clopidogrel alone is suboptimal, even at high dose and administered well in advance of primary PCI.
- Platelet aggregation inhibition
- platelet function
- STEMI
- clinical outcome
- tirofiban
- platelets
Statistics from Altmetric.com
Introduction
Platelets play an important role in the development of acute coronary syndromes.1 Platelet inhibiting drugs, such as glycoprotein IIb/IIIa blockers, inhibit the final common pathway of platelet aggregation and improve results when administered during primary percutaneous coronary intervention (PCI) for an acute myocardial infarction.2–4 Recently, we reported that routine prehospital initiation of high-bolus dose tirofiban in addition to acetylsalicylic acid and high-dose clopidogrel improved ST segment resolution and clinical outcome after primary PCI without increasing major bleeding risk, which emphasises that further platelet aggregation inhibition in addition to high-dose clopidogrel is mandated in patients with ST elevation myocardial infarction (STEMI) undergoing PCI.4 Although reduced levels of platelet aggregation inhibition by antiplatelet therapy are correlated with increased likelihood of major adverse cardiovascular events (MACE) after primary PCI, platelet function measurement is not embedded into daily clinical practice of myocardial infarction management.5–9 Studies investigating the ex vivo platelet variability and clinical outcome after myocardial infarction are of limited patient size.10 We hypothesise that the beneficial effect of triple in comparison with dual antiplatelet therapy is reflected by increased platelet inhibition and that platelet inhibition is related to clinical outcome. Therefore, we assessed platelet function in the On-TIME-2 study patients from two selected participating centres.
Methods
Patients
The study was a prespecified and registered (number ISRCTN06195297) substudy of consecutive patients of the Ongoing Tirofiban in Myocardial Infarction Evaluation 2 trial (On-TIME-2) trial and was performed in two centres in The Netherlands (Zwolle and Nieuwegein). The On-TIME-2 study is a prospective, international multicentre, double-blind, placebo-controlled, randomised clinical trial to evaluate the value of prehospital initiation of high-bolus dose of tirofiban on background therapy of acetylsalicylic acid, unfractionated heparin and 600 mg clopidogrel (600 mg loading dose followed by 75 mg daily for 1 year) in STEMI patients on improving the extent of myocardial reperfusion (primary endpoint).4 11 Eligible patients were randomised to pretreatment with a 25 μg/kg bolus, followed by a maintenance infusion of 0.15 μg/kg/min of tirofiban or placebo. The protocol was approved by our institution's review board and ethical committee and written informed consent was obtained from all patients. PCI was performed immediately after coronary angiography in all patients. All patients were additionally treated with β blockade, statin therapy and ACE inhibition. In our substudy, blood samples were collected before PCI, but after having received study medication (tirofiban or placebo) in addition to 600 mg oral clopidogrel, 5000 IU heparin intravenously and 500 mg acetylsalicylic acid intravenously. The samples were drawn from the femoral sheath in plastic tubes at the start of catheterisation, before additional heparin infusion, using the Vacutainer (Becton Dickinson, Franklin Lakes, New Jersey, USA) system.
Fe induced platelet aggregation
Fe induced platelet aggregation (FIPA) was measured using AISI 434 low carbon stainless steel as a stimulus. Citrate anticoagulated (0.109 M) whole blood was used, collected within 1 h before platelet function testing. Duplicate samples of 2 ml citrated blood were added to tubes containing 100 mg steel wool (Haemoscan, Groningen, Netherlands) and after 5 s mixture on a vortex (type MIX TM01, Retsch, Haan, Germany), incubated for 15 min at room temperature. Subsequently, platelet count was performed on each sample using a routine blood cell counter (Sysmex K4500, Sysmex, Kobe, Japan) and on a reference tube. In the presence of the agonist steel, platelets aggregate and adhere to the steel surface. As the aggregated platelets exceed the threshold limitations for platelet size, they are no longer counted as individual platelets. The ratio between the non-aggregated platelets in the agonist sample and the platelet count in the reference tube without steel multiplied by 100% was used as the platelet aggregation inhibition. The FIPA test was recently validated in a pilot study and was compared with other platelet function tests.12 FIPA measurement was highly reproducible (correlation coefficient r=0.942, p<0.001 between duplicate samples). FIPA correlated well with ADP induced platelet aggregation (r=0.83, p<0.001) but weakly with platelet function analyser (PFA)-100 bleeding time (r=0.56, p<0.001). FIPA could be measured in patients in which platelet aggregation could not be measured by PFA-100 or after ADP because of extensive platelet inhibition by multiple antiplatelet regimes.
ADP induced platelet aggregation
For measurement of the ADP platelet aggregation inhibition, we used the Sysmex K4500 method.13 Blood samples were collected in plastic tubes containing EDTA and tubes containing PPACK with 20 μM/l ADP (Plateletworks, Helena Laboratories, Beaumont, Texas, USA). A routine platelet count was performed on each sample. The platelet count in an EDTA tube was used as a reference. In the presence of the agonist ADP, platelets aggregate and associate. As the aggregated platelets exceed the threshold limitations for platelet size, they are no longer counted as individual platelets. The ratio between the non-aggregated platelets in the agonist sample and the platelet count in the reference tube × 100% was calculated as the platelet aggregation inhibition. In our laboratory, we reported a correlation coefficient of 0.90 between the Sysmex K4500 and the ICHOR point-of-care platelet analyser (Helena Laboratories) to validate the Sysmex K4500 platelet aggregation measurement.14 15
Platelet function analyser
Platelet function was measured using a platelet function analyser (PFA-100, Dade Behring, Marburg, Germany), an instrument that provides a quantitative measurement of platelet adhesion and aggregation in whole blood flowing through a small aperture under high shear conditions.16–19 The aperture (147 μm) is coated with 2 μg type I collagen and 50 μg epinephrine bitartrate (col-EPI) or 50 μg ADP (col-ADP). The closure time of the aperture, referred to as bleeding constant, is an indicator of platelet function.
Clinical outcome
All platelet function tests were compared with the primary outcome of the On-TIME-2 trial: residual ST segment deviation 1 h post-PCI and with MACE (mortality, urgent target vessel revascularisation or recurrent myocardial infarction at 30 days) and early stent thrombosis.
Statistical analysis
Statistical analysis was performed with SPSS V.12.0. Continuous data were expressed as mean±SD, and categorical data as percentage, unless otherwise denoted. The analysis of variance and the χ2 test were appropriately used for continuous and categorical variables, respectively. For comparison of the relationship of four quartiles of platelet aggregation inhibition using FIPA, Plateletworks and PFA-100 with the ST segment deviation at 1 h, ANOVA tests were used. For comparison of the platelet function test and MACE, bleeding and early stent thrombosis was investigated using Pearson's χ2 test. For comparison of the effect of incubation time of study drug and platelet function, a Kruskal–Wallis test was used. A p-value of <0.05 was considered statistically significant.
Results
From June 2004 until November 2007, 1398 patients were randomised. Platelet aggregation inhibition data were available in 648 of the 964 (67%) patients recruited in Zwolle (n=578) and Nieuwegein (n=70) due to late initiation of the platelet function substudy. Platelet aggregation inhibition was measured at a median of 60 min after the administration of study medication in the ambulance. Table 1 presents baseline characteristics of these patients.
Baseline characteristics of patients according to randomisation (n=648)
Platelet aggregation inhibition levels were significantly higher after pretreatment with tirofiban as compared to placebo (figure 1). There was no relationship with longer pretreatment time and platelet aggregation inhibition for either dual or triple antiplatelet pretreatment (table 2).
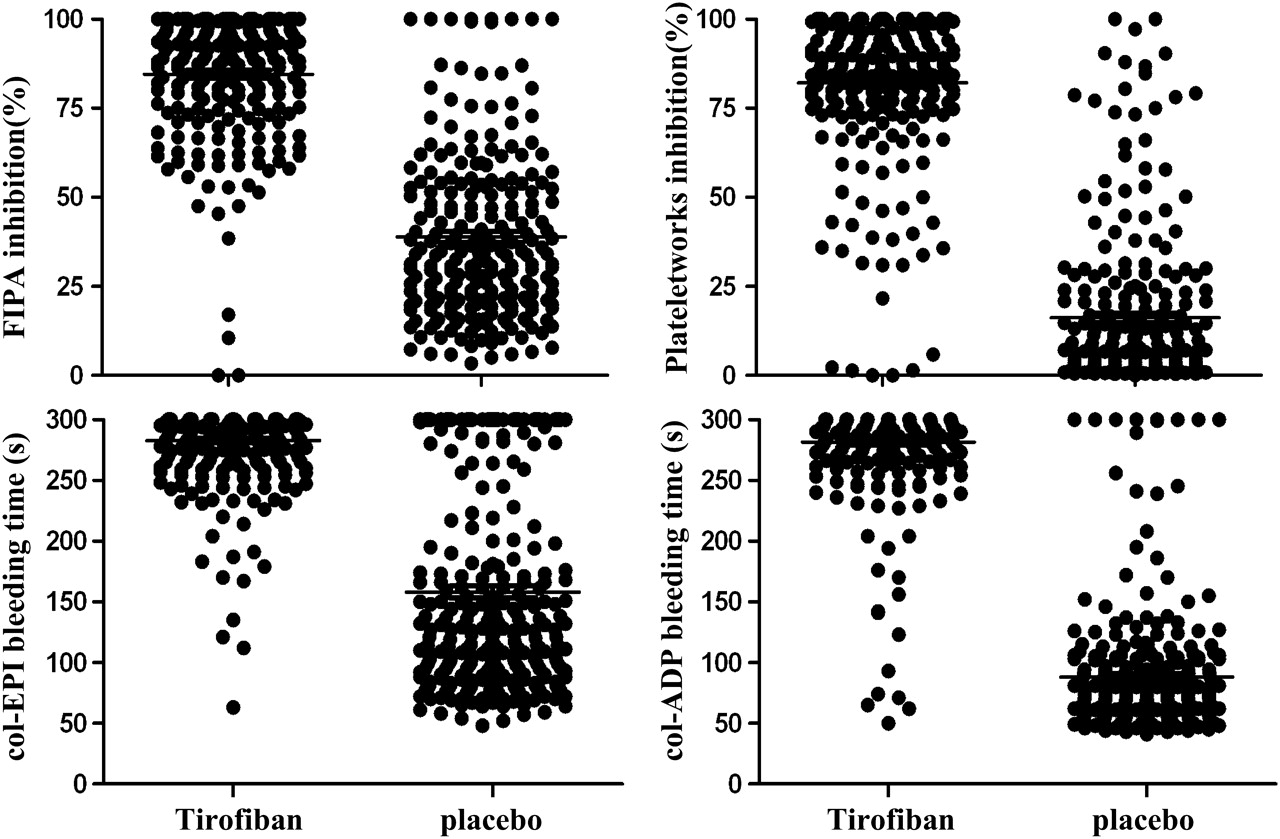
Platelet aggregation inhibition levels in patients receiving high-dose tirofiban were significantly higher as compared with placebo using Fe induced platelet aggregation (FIPA), Plateletworks and platelet function analyser (PFA)-100 (col-EPI and col-ADP); p<0.001 for all four tests. col-EPI, collagen–epinephrine cartridge; col-ADP, collagen–epinephrine cartridge.
Levels of platelet aggregation inhibition according duration of infusion with dual or triple antiplatelet therapy in quartiles of infusion duration
After more than 74 min of pretreatment with high-dose clopidogrel and acetylsalicylic acid, the mean level of platelet inhibition was still below half of the platelet inhibition levels after maximal 45 min of pretreatment with additional tirofiban.
Platelet function and clinical outcome
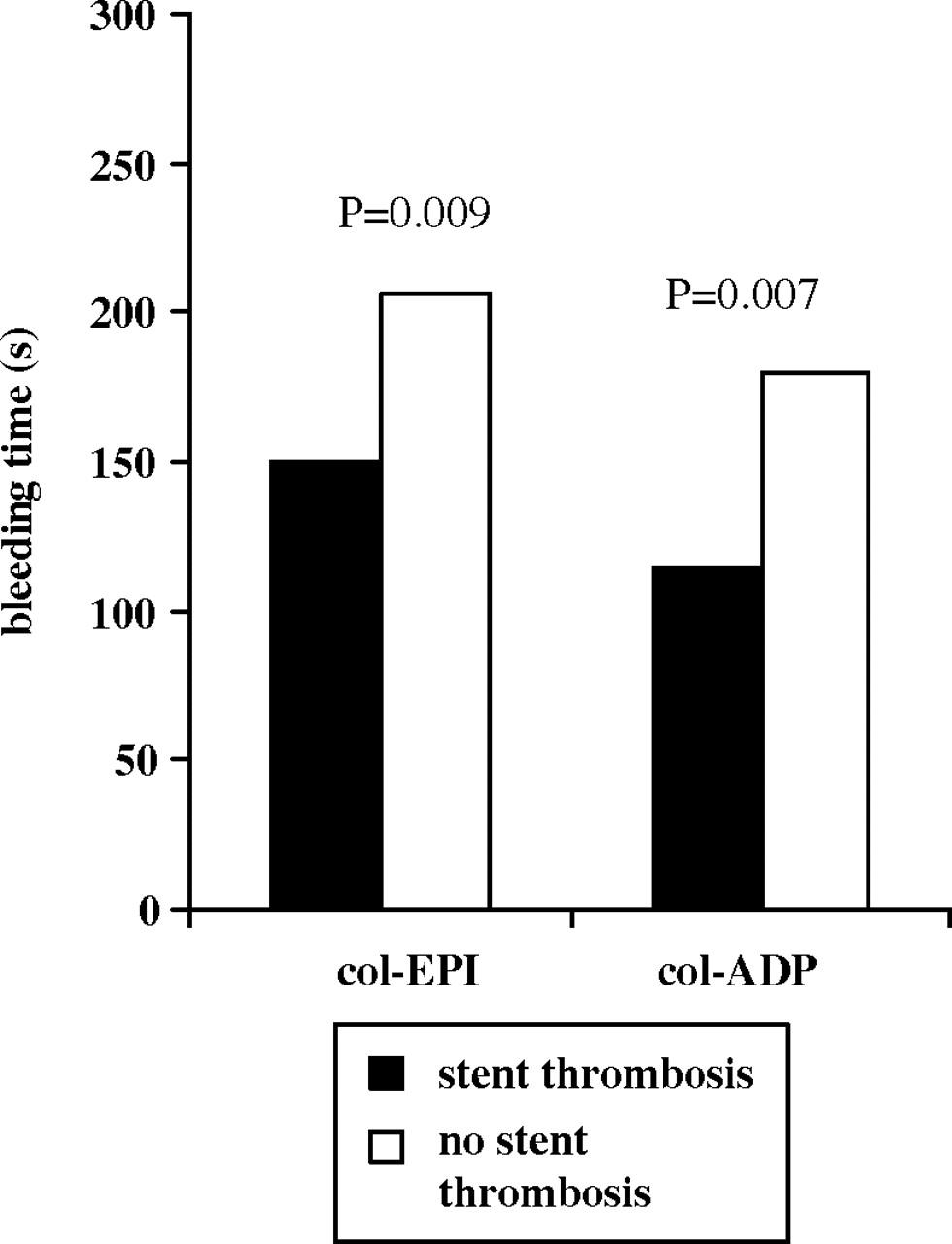
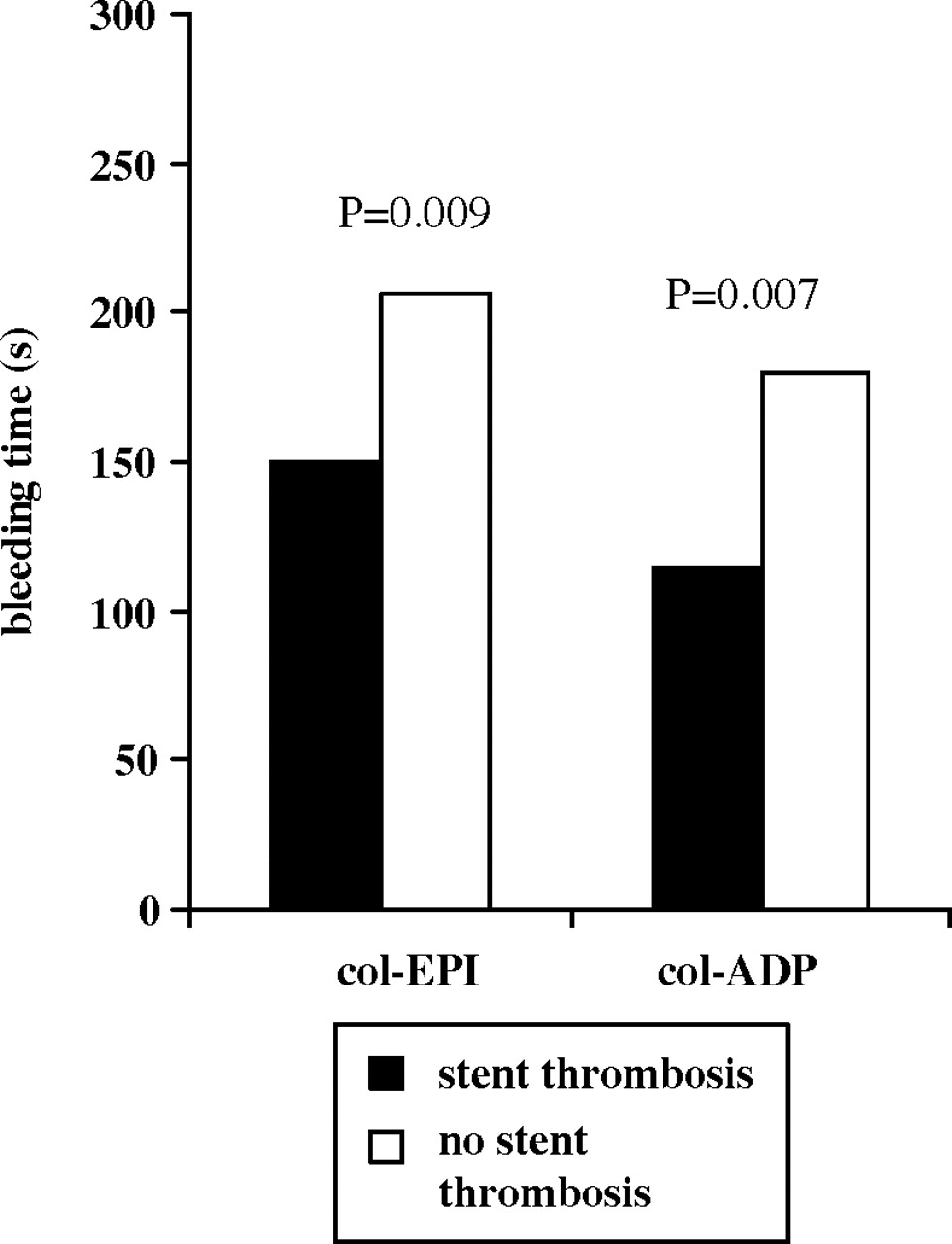
Patients in the highest quartile of platelet aggregation inhibition, using either FIPA or Plateletworks or PFA-100 (col-EPI or col-ADP) had less residual ST segment deviation on the 1 h post PCI ECG (figure 2). In 5.9% of patients a MACE occurred, and in 2.5% an early stent thrombosis occurred. There was a significant relationship between PFA-100 (col-EPI and col-ADP) and MACE and early stent thrombosis (figures 3 and 4). The other two platelet function test did not show a significant correlation with MACE or early stent thrombosis. There was no relationship between PFA-100 and subacute (later than day 1) stent thrombosis.
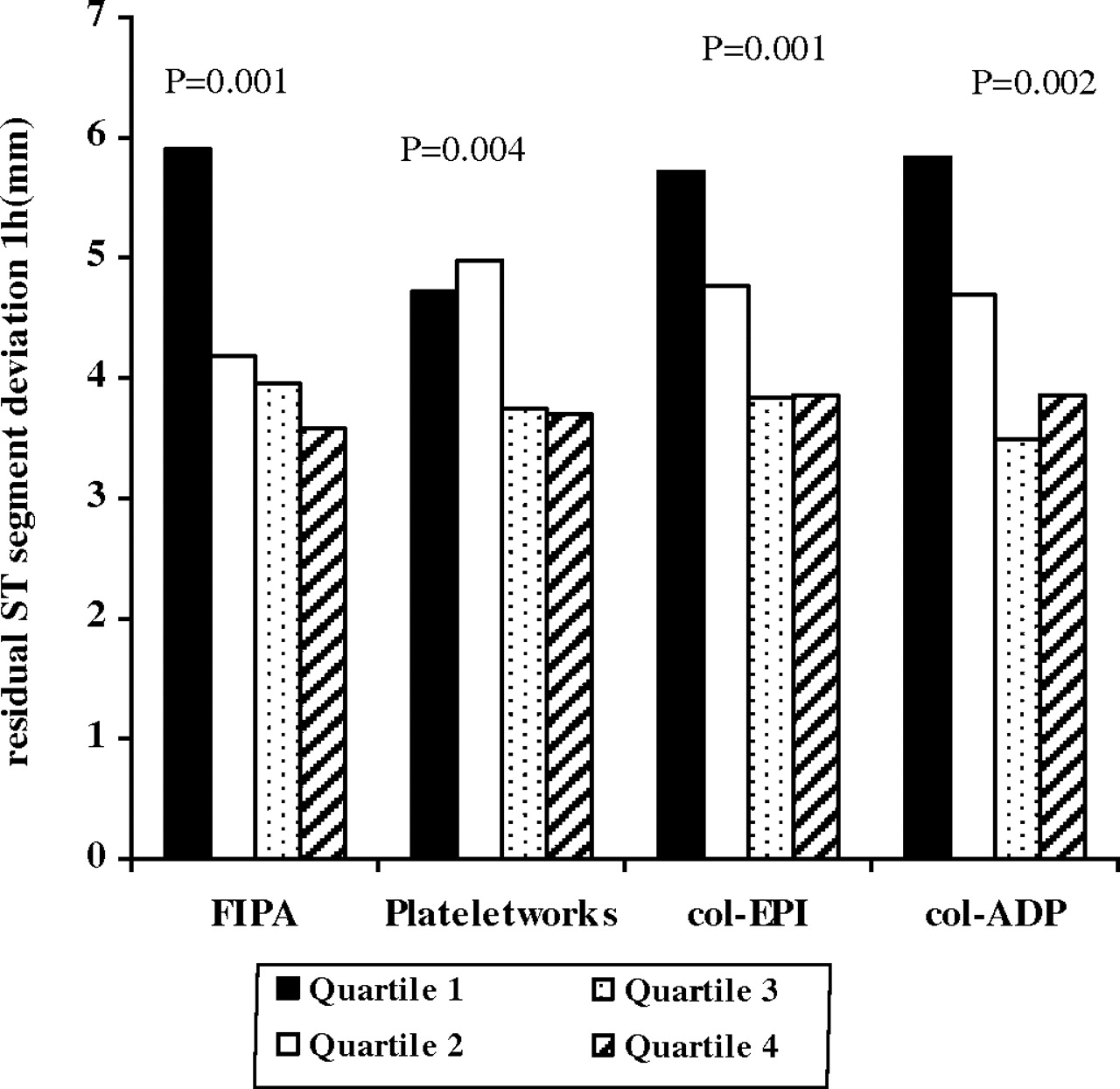
Residual ST segment deviation on the 1 h post-percutaneous coronary intervention according to four quartiles of platelet aggregation inhibition using Fe induced platelet aggregation (FIPA), Plateletworks and platelet function analyser (PFA)-100 (col-EPI and col-ADP) (p value for trend: 0.001, 0.004, 0.001, 0.002, respectively). Median of platelet aggregation inhibition or bleeding time of quartile 1=black, quartile 2=white, quartile 3=dotted, quartile 4=striped. col-EPI, collagen–epinephrine cartridge; col-ADP, collagen–epinephrine cartridge.

Major adverse cardiovascular events (MACE) according to four quartiles of platelet aggregation inhibition using platelet function analyser (PFA)-100 (col-EPI and col-ADP). col-EPI, collagen–epinephrine cartridge; col-ADP, collagen–epinephrine cartridge; IPA, inhibition of platelet aggregation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Early stent thrombosis and bleeding time using platelet function analyser (PFA)-100 (col-EPI and col-ADP). col-EPI, collagen–epinephrine cartridge; col-ADP, collagen–epinephrine cartridge.
Platelet function and bleeding
Bleeding complications occurred in 9.5% in the placebo group and in 10.7% in the tirofiban group (p=0.62). There was no relationship between the level of platelet aggregation inhibition by either of the four platelet function tests used and bleeding complications, neither for the total group (respectively, FIPA, Plateletworks, col-EPI, col-ADP: p=0.99, p=0.31, p=0.23, p=0.89) nor among the two randomised groups: tirofiban (respectively, FIPA, Plateletworks, col-EPI, col-ADP: p=0.73, p=0.21, p=0.47, p=0.93) and placebo (respectively, FIPA, Plateletworks, col-EPI, col-ADP: p=0.87, p=0.40, p=0.31, p=0.14).
Discussion
This is the largest study so far, in which the relationship between platelet aggregation inhibition after dual or triple antiplatelet therapy and clinical outcome was prospectively investigated in STEMI patients undergoing primary PCI. It showed that a median of 60 min of prehospital treatment with triple antiplatelet therapy, including high-dose tirofiban, resulted in significantly higher platelet aggregation inhibition, as compared to dual antiplatelet therapy including high-dose clopidogrel. Longer pretreatment with clopidogrel up to 2 h did not improve platelet aggregation inhibition as compared with shorter pretreatment. Since there was no difference between initiation of dual or triple antiplatelet therapy within 45 min or after 45 min, it might be extrapolated that earlier initiation within 45 min does not change the antiplatelet effect of both high-dose clopidogrel as high-dose tirofiban and there is indeed a rapid effect of as well dual as triple antiplatelet therapy.
Glycoprotein IIb/IIIa receptor blockers, which block the final common pathway leading to platelet aggregation, improve the patency of the infarct related vessel in patients with an acute myocardial infarction, when prehospitally initiated.4 20 It has recently been questioned whether bleeding complications may limit the amount of antithrombotic agents in patients with an acute coronary syndrome.21 22 The On-TIME-2 data, however, did not show an increased bleeding risk in patients pretreated with high-dose tirofiban in addition to high-dose clopidogrel, acetylsalicylic acid and unfractionated heparin. This study showed that a higher inhibition of platelet aggregation was associated with better ST segment resolution 1 h after PCI. Furthermore, PFA-100 bleeding time was related to major adverse events including early stent thrombosis. Therefore, this On-TIME-2 substudy confirmed the main findings of the trial that pretreatment with clopidogrel alone results in suboptimal outcome, even when given at the high 600 mg dose and given well in advance of angioplasty.
Measurement of platelet function to monitor the effect of platelet inhibiting drugs, or to specify high-risk patient groups in myocardial infarction patients did not result in platelet function tests being embedded into daily clinical practice.10 Current platelet function tests might not encompass the complete complexity of platelet biology and function because of inappropriate agonists or lack of multi-pathway activation and reproducibility.10 23 Furthermore, studies investigating the ex vivo platelet variability and clinical outcome after myocardial infarction are of limited patient size.5–9 High platelet reactivity was found in patients who experienced stent thrombosis, and patients with clopidogrel resistance were at increased risk of recurrent atherothrombotic events.5 6 Furthermore, in STEMI patients increased levels of platelet aggregation (related to infarct size) were found as compared to unstable angina or control patients.7 A thrombolysis study reported platelet receptor occupancy to be associated with better angiographic and electrocardiographic outcome.8 Finally, in STEMI patients undergoing primary PCI, increased inhibition of platelet aggregation by abciximab was found to be associated with better myocardial reperfusion.9 In our current study, we also found a relationship between platelet function and the extend of myocardial perfusion, as reflected by improved ST segment resolution. Furthermore, bleeding time using PFA-100 correlated with MACE and early stent thrombosis. This finding was in contrast to our former platelet function substudy in the On-TIME-1 study, in which no relationship was found between the levels of platelet aggregation inhibition and clinical outcome.24 This might be explained by the small number of major adverse cardiac events or it could be due to an insufficient method of platelet aggregation measurement in the On-TIME-1 study. In the On-TIME-1 study we used ADP as an agonist for platelet aggregation inhibition measurement. It is questionable whether this single pathway platelet aggregation agonist is sufficient to simulate the multipathway platelet aggregation in acute coronary syndrome. In the On-TIME-2 study we used the same single pathway platelet function test in a larger patient population in addition to two other multipathway platelet function tests. Both the ADP aggregation test as the FIPA and PFA correlated with ST resolution in the On-TIME-2 study. In addition, PFA bleeding time correlated with MACE and predicted early stent thrombosis after primary PCI. The dynamic flow conditions and shear stress related platelet aggregation in the PFA-100 may provide a better model for platelet aggregation in human coronary arteries as compared to the more static tests such as ADP aggregation and FIPA.
Limitations
Although we studied the largest population so far, it was relatively small for studying the relationship with clinical adverse events which occurred in only 37 patients (5.9%). Therefore, a correlation between platelet microaggregation inhibition and clinical outcome in myocardial infarction patients should be further investigated in a larger population. The conclusion that platelet function cannot predict bleeding complications should be interpreted with caution, since bleeding complications occurred in a small number of patients as well. Furthermore, although PFA-100 might be recommended to be used in future platelet function testing in patients using multiple antiplatelet regimes to select insufficient antiplatelet therapy, the optimal method of platelet aggregation testing remains subject to discussion. It is unknown whether the studied methods of platelet aggregation are the major pathophysiological pathways of platelet aggregation leading to thrombotic complications in an acute coronary syndrome.
Conclusions
Despite pretreatment with high-dose clopidogrel and acetylsalicylic acid for up to 2 h, platelet aggregation inhibition was significantly higher when high-dose tirofiban was added to this regimen. The level of platelet aggregation inhibition was related to reduced residual ST segment deviation 1 h after PCI. Furthermore, PFA-100 bleeding time was related to major adverse events and early stent thrombosis. Therefore, this substudy confirms the results of the main findings of the On-TIME trial that clopidogrel alone is not sufficient, even at high dose and administered well in advance of primary PCI.
Acknowledgments
The authors thank Vera Derks for preparing the manuscript.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Isala Klinieken Zwolle and St Antonius Hospital Nieuwegein, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.