Article Text

Abstract
Objective To determine the calcium score and coronary plaque burden in asymptomatic statin-treated patients with heterozygous familial hypercholesterolaemia (FH) compared with a control group of patients with low probability of coronary artery disease, having non-anginal chest pain, using CT.
Design, setting and patients 101 asymptomatic patients with FH (mean age 53±7 years; 62 men) and 126 patients with non-anginal chest pain (mean age 56±7 years; 80 men) underwent CT calcium scoring and CT coronary angiography. All patients with FH were treated with statins during a period of 10±8 years before CT. The coronary calcium score and plaque burden were determined and compared between the two patient groups.
Results The median total calcium score was significantly higher in patients with FH (Agatston score=87, IQR 5–367) than in patients with non-anginal chest pain (Agatston score=7, IQR 0–125; p<0.001). The overall coronary plaque burden was significantly higher in patients with FH (p<0.01). Male patients with FH, whose low-density lipoprotein cholesterol levels were reduced by statins below 3.0 mmol/l, had significantly less coronary calcium (p<0.01) and plaque burden (p=0.02).
Conclusion The coronary plaque burden is high in asymptomatic middle-aged patients with FH despite intense statin treatment.
- CT
- coronary plaque burden
- atherosclerosis
- familial hypercholesterolaemia
- CT scanning
- lipids, coronary artery disease (CAD)
Statistics from Altmetric.com
- CT
- coronary plaque burden
- atherosclerosis
- familial hypercholesterolaemia
- CT scanning
- lipids, coronary artery disease (CAD)
Introduction
Familial hypercholesterolaemia (FH) is an autosomal dominant disorder caused by mutations in the low-density lipoprotein (LDL) receptor gene and is characterised by raised serum levels of LDL cholesterol, tendon xanthomas and high risk of coronary artery disease (CAD).1–4
Recently, we demonstrated that statin treatment greatly reduces the risk of CAD in patients with FH who were detected in our nationwide screening programme; the risk of myocardial infarction in these treated patients with FH was not significantly higher than that of the general population, while the mean treated LDL cholesterol level was much higher than current target levels.5 Although these data suggest that asymptomatic treated patients with FH have only mild CAD, it provides no direct evidence of the presence and severity of residual CAD in treated patients with FH. The use of cardiac CT enabled us to anatomically verify these findings.
Over the past few years cardiac CT has emerged as a safe, non-invasive modality for imaging coronary atherosclerosis. A non-enhanced scan shows the total amount of coronary calcium; while contrast-enhanced CT coronary angiography (CTCA) permits evaluation of both calcified and non-calcified plaques as well as narrowing of the vessel lumen.
To date the presence of subclinical CAD in an asymptomatic high-risk FH population has only be studied by Miname et al6 in relatively young patients with FH, of whom only 66% were receiving previous statin treatment and all underwent a washout period of 6 weeks before evaluation.
The purpose of this single-centre study was to determine the presence and extent of coronary plaques in asymptomatic statin-treated patients with FH by CTCA and to compare these results directly with the CTCA findings in patients with non-anginal chest pain as a substitute for asymptomatic non-FH patients. Additionally, the relation between patient characteristics, risk factors and cholesterol levels and the extent of CAD was assessed.
Materials and methods
Study population
Between February 2008 and February 2009 we included 101 consecutive, asymptomatic patients with FH and 126 patients with non-anginal chest pain in our CTCA study, as the radiation exposure limits the choice of controls to patients with an indication for CTCA.
The patients with FH were recruited from our outpatient lipid clinic. The following diagnostic criteria for FH were used: either (1) the presence of a documented LDL receptor mutation, or (2) an LDL cholesterol level above the 95th percentile for sex and age in combination with at least one of the following: (a) the presence of typical tendon xanthomas in the patient or in a first-degree relative or (b) an LDL cholesterol level above the 95th percentile for age and sex in a first-degree relative or (c) proven CAD in the patient or in a first-degree relative under the age of 60.7 From this group, patients who were symptomatic for CAD, defined as the presence of symptoms suggestive of ischaemic heart disease or known CAD in their history, and patients with secondary causes of hypercholesterolaemia such as renal, liver, or thyroid disease were excluded from the study.
The patients with non-anginal chest pain were recruited from a patient population without a history of CAD referred by their general practitioner for evaluation of chest pain and underwent stress testing and cardiac CT. Non-anginal chest pain was defined as chest pain or discomfort that met one or none of the following typical angina characteristics: (1) substernal chest pain or discomfort that is (2) provoked by exertion or emotional stress and (3) relieved by rest and/or nitroglycerin.8
The inclusion age was 40–70 years, except for women with FH where it was 45–70 years. Exclusion criteria were renal insufficiency (serum creatinine >120 μmol/l), known contrast allergy and irregular heart rhythm (atrial fibrillation).
The institutional ethical review board approved the study protocol. All patients gave written informed consent.
Scan protocol
Just before the scan all patients received nitroglycerin (0.4 mg/dose) sublingually.
All scans were performed with a dual-source CT scanner (Somatom Definition, Siemens Medical Solutions, Forchheim, Germany). For the non-enhanced scan a prospective ECG-triggered scan protocol was applied. The CTCA scan protocol, contrast protocol and reconstruction procedure have been described previously.9 Briefly, the CTCA was obtained using a retrospective ECG-gated scan protocol with optimal heart rate-dependent ECG pulsing10 to lower the radiation dose. The maximum tube current was 380 mA and the tube voltage was 120 kV. The mean estimated radiation dose per CTCA, calculated by multiplying the dose–length product by the conversion coefficient of 0.014 mSv/mGy/cm for the chest, was 7.9±2.4 mSv (range 3.9–16.4 mSv).11 Iodinated contrast agent (Ultravist 370 mgI/ml, Schering AG, Berlin, Germany), with a scan time-dependent volume (94 ml (80–100 ml)), was administered for enhancement of the coronaries. The calcium score datasets were reconstructed with a slice thickness of 3 mm and an increment of 1.5 mm at 70% of the RR-interval. CTCA datasets were reconstructed using a slice thickness of 0.75 mm and an increment of 0.4 mm at an automatically or manually determined optimal phase of the RR-interval. All datasets were sent to a dedicated workstation (MMWP, Siemens).
CT analysis
The calcium score was calculated semiautomatically using dedicated software and expressed as the Agatston score per patient.12
All CTCA scans were evaluated separately by two experienced readers and all discrepancies in evaluation were resolved during a consensus reading. Coronary plaque was defined as a separate structure within the vessel wall that could be clearly distinguished from the contrast-enhanced lumen and the surrounding pericardial tissue. For each segment, using the American Heart Association 16-segment model,13 the absence or presence of a coronary plaque was determined, as was the severity of the lumen narrowing (0, >0–50% and >50% diameter stenosis). For each patient the extent of CAD, defined as the number of segments with a non-obstructive (>0–50% diameter stenosis) or obstructive (>50% diameter stenosis) lesion, was determined. The plaque composition was also documented and classified as (1) calcified: plaque containing highly attenuating tissue that could be clearly separated from the contrast-enhanced coronary lumen and (2) non-calcified: low attenuating lesions that could be clearly separated from the coronary lumen and the surrounding epicardial fat and myocardium. Vessel segments <1.5 mm in diameter were excluded from all analyses. The coronary plaque burden was expressed as the severity of coronary obstructions, the extent of CAD, the number of diseased coronary arteries, segments and plaque composition.
Management of patients with FH
All included patients with FH were regularly seen in the outpatient clinic for monitoring of their lipid levels and subsequent optimisation of the medical treatment and early detection of complications of FH. They all received statins. Intense statin treatment was defined as the daily use of either 80 mg atorvastatin, 80 mg simvastatin or 40 mg rosuvastatin. We used a cut-off value of LDL cholesterol of <3.0 mmol/l to define patients with a substantial lowering of LDL cholesterol and to relate this to the extent of CAD.
Statistical analysis
Continuous variables are shown as mean (±SD) or median (IQR). Categorical variables are expressed as number (frequency). We used the t test or Mann–Whitney U test to compare continuous variables and the χ2 test or the Fisher exact test for the comparison of categorical variables. A p value <0.05 was considered significant. The relationship between the extent of CAD in patients with FH, and the duration of statin treatment, the achievement of an LDL cholesterol level <3 mmol/l, the high-density lipoprotein, the maximum total cholesterol levels before treatment and the age at the start of statin treatment was assessed using a multivariate linear regression model.
Interobserver and intraobserver variability are described with the κ statistics. Intraobserver variability was conducted in a subgroup of 30 randomly selected scans scored twice by one observer, with a minimum of 2 months between the two evaluations. All analyses were performed using SPSS for windows (version 15.0, SPSS).
Results
Baseline
Figure 1 shows the inclusion flow chart. During the recruitment period 153 patients with FH were eligible for the study, of whom 101 gave informed consent. From the symptomatic population scheduled for cardiac CT, 146 patients were classified as having non-anginal chest pain, of whom 126 were eligible for inclusion.

Patient inclusion flowchart. CAD, coronary artery disease; CTCA, CT coronary angiography; FH, familial hypercholesterolaemia.
The patient characteristics are shown in table 1. All included patients with FH received statins; 31 patients (32%) did not receive intense statin treatment because of severe side effects. Most patients with FH (42%) used atorvastatin 80 mg (mean 68 mg), simvastatin (29%, mean 58 mg) and rosuvastatin (24%, mean 35 mg). Less commonly used lipid-lowering drugs were pravastatin, colestyramine and ciprofibrate, ezetimibe was combined with statins in 59% of cases.
Patient characteristics
Of 126 controls, 72 patients had dyslipidaemia. All these patients were treated with a cholesterol-lowering diet and 67% also used low-dose statins: 31% used atorvastatin (mean 33 mg), 54% used simvastatin (mean 28 mg), 10% used rosuvastatin (mean 14 mg), pravastatin and ezetimibe were both used with a mean dose of 10 mg by 4% and 10% of controls, respectively. Gender distribution was comparable between the patients with FH and the non-anginal patients (62 (61%) and 80 (63%), respectively, p=0.78). The mean age of the non-anginal controls was slightly higher (56±7 vs 53±7 years, p=0.01). By selection, dyslipidaemia and positive family history for cardiovascular disease were more frequently found in the patients with FH, who had significantly fewer other risk factors.
No complications occurred during or after scanning. All scans were included in the analysis. We excluded 43 segments because of insufficient image quality owing to motion artefacts, leaving 3621 segments available for analysis. The κ statistics of the interobserver and intraobserver variability for the evaluation of the stenosis severity per plaque were 0.80 and 0.82, respectively, and for the evaluation of plaque composition 0.83 and 0.83, respectively.
CT calcium score
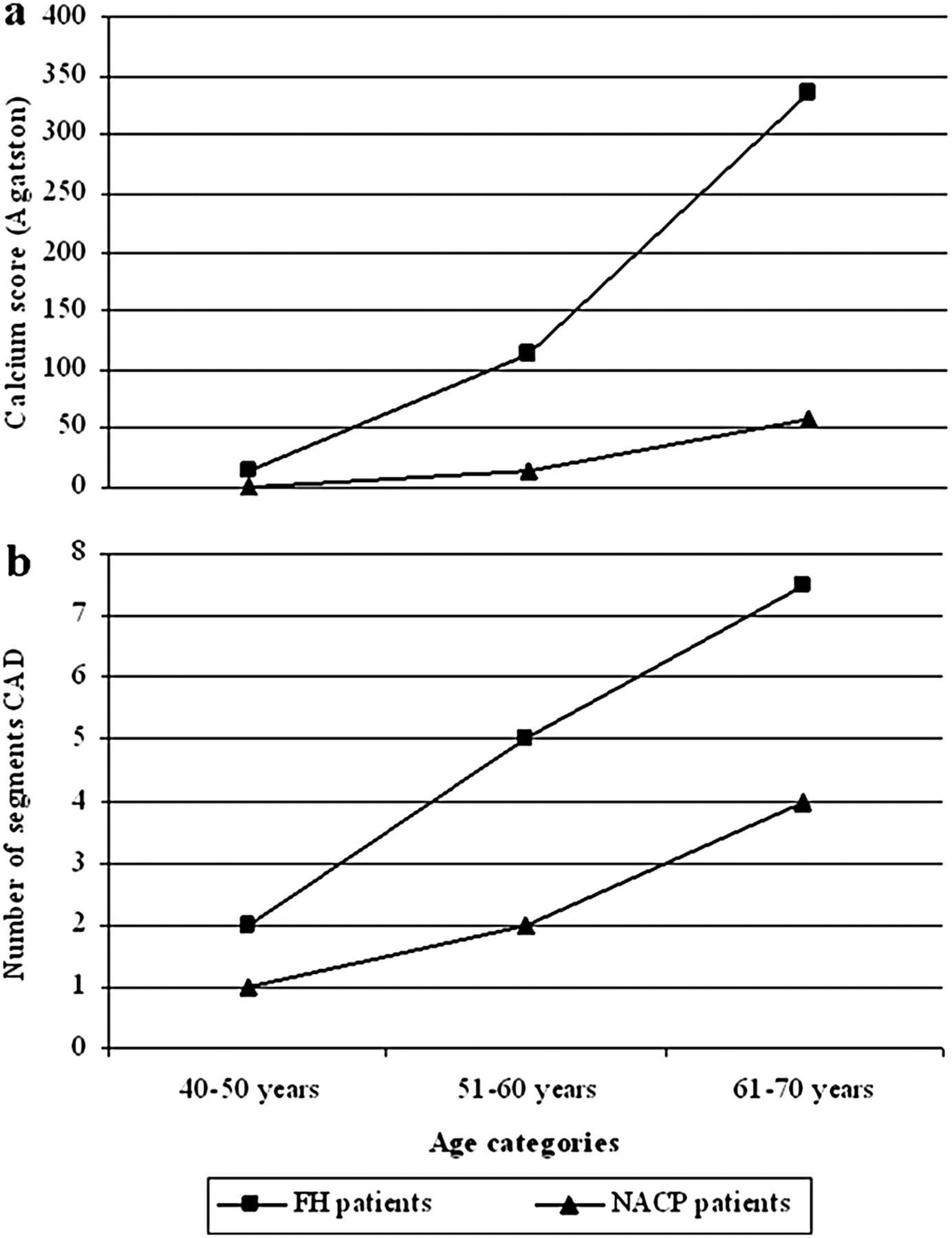
The median total calcium score was significantly higher in patients with FH (87, IQR 5–367) than in patients with non-anginal chest pain (7.3, IQR 0–125; p<0.001), with less negative calcium scores in patients with FH (20, 20±4%) than in patients with non-anginal chest pain (49, 39±4%, p<0.001) (table 1). In patients with FH men had a significantly higher total calcium score (149, IQR 24–430) than women (21, IQR 0–171; p=0.003) while in patients with non-anginal chest pain this difference was not evident (13, IQR 0–153 and 1, IQR 0–99, respectively; p=0.221). The total calcium score was higher in patients with FH in all age groups and increased with higher age (figure 2A).
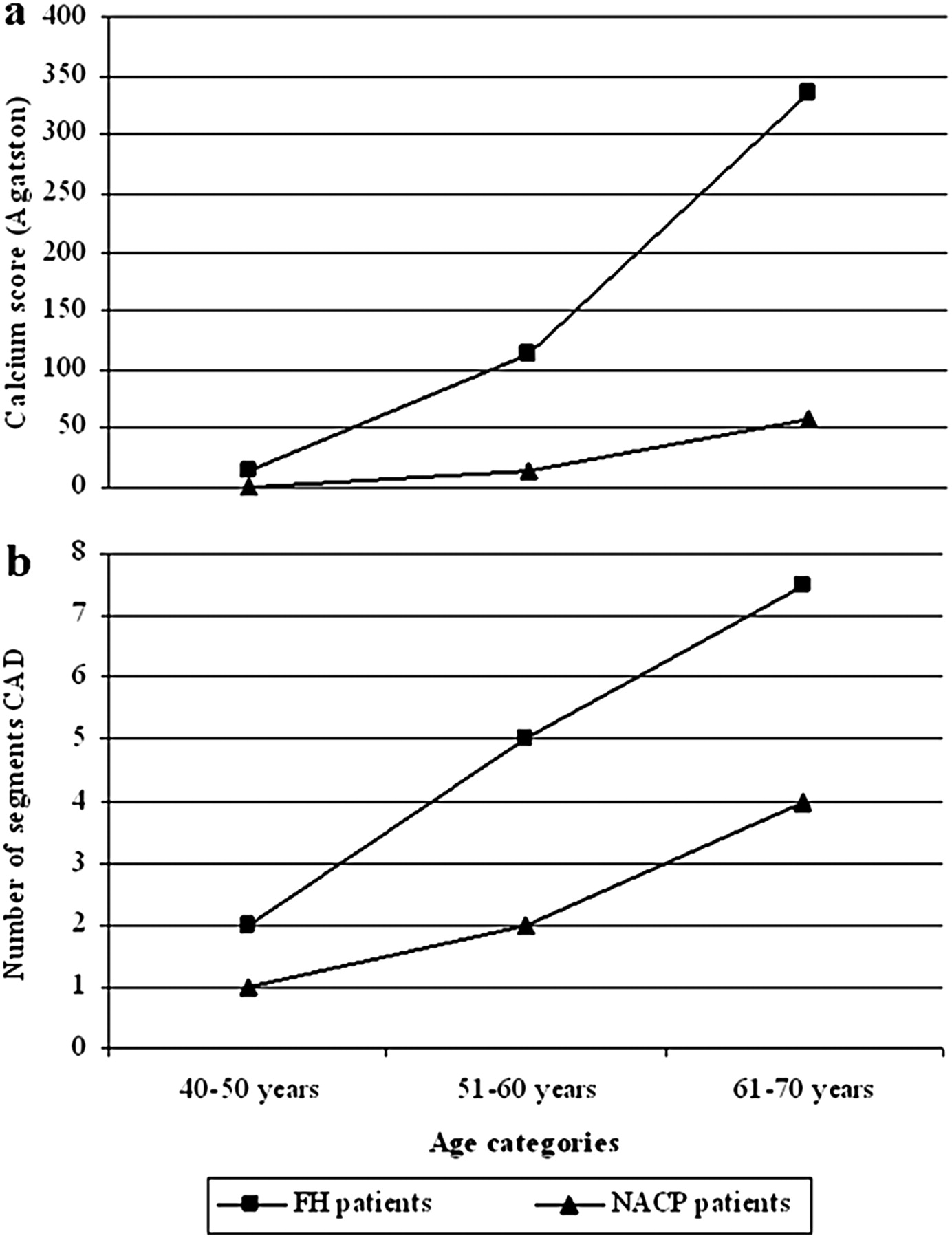
Calcium score and plaque burden according to different age categories. Calcium score and number of plaque-containing segments are expressed as median for each age group. CAD, coronary artery disease; FH, familial hypercholesterolaemia; NACP, non-anginal chest pain.
CT coronary angiography
In table 2 the coronary plaque burden on a per patient and a per segment level is shown.
CTCA plaque burden per patient and per segment
The severity and extent of CAD on a per patient and a per segment level was significantly higher in patients with FH than in patients with non-anginal chest pain. In the FH group 15 (15%) patients did not have any signs of CAD and in the group with non-anginal chest pain 41 (33%) patients presented with non-diseased coronary arteries (p=0.002). On a per segment level the severity of CAD and composition of plaque were significantly different between patients with FH and controls for both men and women. The number of coronary segments with non-obstructive or obstructive CAD was higher in patients with FH in all age groups and increased with higher age (figure 2B).
Table 3 shows the relation between the calcium score and the presence of non-obstructive and obstructive plaque in patients with FH.
Calcium score in relation to CAD severity per patient
In male patients with FH, achieving LDL cholesterol <3.0 mmol/l during statin treatment was significantly (p<0.01) associated with a lower plaque burden (table 4). In female patients with FH we did not observe such a relationship between statin-induced LDL cholesterol levels and coronary plaque burden.
Coronary plaque burden according to achievement of the target value of 3.0 mmol/l LDL-cholesterol in the blood of treated men with FH
Multivariate analysis revealed that age, gender, highest untreated total cholesterol levels and treated high-density lipoprotein cholesterol levels predicted the magnitude of the severity and extent of CAD in patients with FH (data not shown).
Discussion
In this study we demonstrated, using CT, that subclinical coronary atherosclerosis was present in the majority (85%) of asymptomatic patients with FH, despite ‘normalisation’ of cholesterol levels with long-term (10±8 years) statin treatment (figure 3).

{kind=link}
{kind=link}
{kind=link}
Curved multiplanar reconstructed (cMPR) CT images and cross sections of the left anterior descending coronary artery of four asymptomatic patients with familial hypercholesterolaemia showing a non-diseased vessel (1a, 1b), a non-obstructive calcified lesion (2a, 2b), an obstructive partly calcified lesion (3a, 3b) and an obstructive severely calcified lesion (4a, 4b).
Asymptomatic patients with FH, at different ages (40–50 years, 51–60 years and 61–70 years), had a higher calcium score and coronary plaque burden than our control group of patients with non-anginal chest pain having low probability of CAD, and a higher score and plaque burden than other coronary asymptomatic populations who underwent CT calcium scoring14–17 and CTCA.18 Previous studies revealed that in 2–4% of symptomatic and asymptomatic patients with a calcium score of 0 an obstructive coronary lesion is present.19 20 In our study none of the 20 patients with FH with a calcium score of 0 presented with an obstructive lesion or exhibited non-obstructive CAD in more than two segments. However, our study comprised only 20 patients with FH without coronary calcium, and larger studies are required to determine the prevalence of obstructive CAD in these patients.
Despite the absence of symptoms, 26% of the patients with FH exhibited obstructive CAD occurring at relatively young age averaging 53±7 years. This was in a similar range to the presence of obstructive CAD detected by CTCA in 17–39% of asymptomatic diabetic patients21–23 and 25% of our non-anginal chest pain group and also within the range of 16–62% in symptomatic coronary patients.24 25 The presence of obstructive CAD in 26% of our FH population, however, was a little higher than the 19% in a younger (45±13 years) FH population6 and much higher than the approximately 5% in other high-risk asymptomatic populations.18 26
The extent and severity of CAD, as established with CTCA, was higher in patients with FH than in the patients with non-anginal chest pain, but these differences were less striking in women, where the differences were not statistically significant. This may be explained by the relatively small numbers of women, which may preclude reaching the level of significance. In addition, we found an unexpectedly relatively high prevalence of obstructive lesions in women with non-anginal chest pain.18 27 This may be related to the fact that complaints of women often are misinterpreted as non-specific chest pain, which may result in a delay in diagnostic testing and progression to a more advanced stage of CAD.
Clinical CAD in untreated patients with FH usually manifests in men between the ages of 30 and 50 years and in women between 50 and 70 years.28 Statin treatment has been shown to reduce the clinical manifestations in patients with FH.5 6 29 In our study we studied middle-aged patients with FH who were free of coronary symptoms during approximately 10 years of statin treatment. Yet, CTCA revealed that the coronary plaque burden was substantial and that CAD was present in the majority (85%) of these patients. Apparently, intense treatment with statins prevented progression to clinical expression of CAD but did not reduce the extent of CAD as was shown by the relatively high calcium scores, the presence of extensive non-obstructive CAD (more than two coronary segments involved) in more than 60% of the patients and the presence of obstructive CAD in 25% of these patients. This suggests that the coronary plaques in patients with FH have been stabilised by statin treatment preventing the occurrence of coronary events. In our study we observed a higher prevalence of calcified plaques in the FH population than in the non-anginal chest pain population. Calcified plaques are known to be less vulnerable and less prone to rupture.30 31
Notably, statin treatment was more effective in men, reducing LDL cholesterol levels to <3 mmol/l. These men had a lower calcium score and less CAD than men with higher LDL cholesterol levels.
Longer-term follow-up studies are necessary to demonstrate that statin treatment is associated with sustained reduction of symptomatic CAD and prolongation of life in these patients with FH.
Limitations
We used patients with non-anginal chest pain as controls instead of a group of healthy people, who might have had a smaller coronary plaque burden, because CT-associated radiation exposure makes it unethical to perform CTCA in asymptomatic volunteers. We selected this group of patients with non-anginal chest pain because we expected a prevalence of obstructive CAD of approximately 8% (women) to 22% (men).27 However, we found a higher prevalence of obstructive CAD in women (24%) but a comparable prevalence in men (26%). Nevertheless, we still observed a significantly higher coronary plaque burden in male and female treated patients with FH.
It is known that CTCA is less able to detect small non-calcified plaques and therefore our reported prevalence of non-calcified lesions may be underestimated.32 33 Furthermore, it should be noted that CTCA, particularly in the case of calcified lesions, may overestimate the severity of coronary stenosis,34 and hence the prevalence of obstructive lesions in our study population may have been overestimated.
Ideally, we would have confirmed our CT findings with conventional invasive coronary angiography and intravascular ultrasound, which is the standard of reference for plaque detection, but our FH population was asymptomatic and thus additional coronary angiography was considered unethical. However, it has been shown that moderate to large coronary plaques can be reliably detected by CTCA.35 36
Our study was a cross-sectional observational study and does not allow evaluation of the progression of CAD in patients with FH receiving statin treatment. And finally, our study was restricted to patients aged between 40 and 70 years, and findings may be different in elderly patients.
Conclusion
Despite long-term intense statin treatment of middle-aged patients with FH, the occurrence of CAD was higher in this group than in a control group of patients with non-anginal chest pain as well as other asymptomatic populations. Non-invasive low radiation exposure CT coronary imaging by demonstrating the extent and severity of underlying CAD may have a future role in the early detection of CAD, clinical management and prediction of risk in patients with FH.
References
Footnotes
EJS and PJF contributed equally to this article.
Funding This study was supported by a grant from the Dutch Heart Foundation, The Hague, the Netherlands and the Interuniversity Cardiology Institute of the Netherlands, Utrecht, the Netherlands.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the ethical review board of the Erasmus Medical Center Rotterdam.
Provenance and peer review Not commissioned; externally peer reviewed.