Article Text

Abstract
Background An inadequate response to clopidogrel is mainly attributable to the variable formation of its active metabolite. The CYP2C19*2 loss-of-function polymorphism leads to reduced generation of the active metabolite and is, similarly to high on-treatment platelet reactivity (HPR), associated with recurrent atherothrombotic events following coronary stent implantation.
Aim To determine the relative contribution of CYP2C19*2 genotype to HPR.
Methods and results CYP2C19*2 genotyping and platelet function testing using 5 and 20 μmol/l ADP-induced light transmittance aggregometry (LTA), the PlateletWorks assay and the VerifyNow P2Y12 assay, were performed in 1069 clopidogrel pretreated patients undergoing elective coronary stenting (POPular study, http://clinicalTrials.gov/ NCT00352014). The relative contributions of CYP2C19*2 genotype and clinical variables to the interindividual variability of on-treatment platelet reactivity and the occurrence of HPR were established using multivariate regression models. CYP2C19*2 carrier status was associated with a more frequent occurrence of HPR. CYP2C19*2 genotype alone could explain 5.0%, 6.2%, 4.4% and 3.7% of the variability in 5 and 20 μmol/l ADP-induced LTA, the PlateletWorks assay and the VerifyNow P2Y12 assay, respectively, which increased to 13.0%, 15.2%, 5.6% and 20.6% when clinical variables were considered as well. Besides the CYP2C19*2 genotype, multiple clinical variables could be identified as independent predictors of HPR, including age, gender, body mass index, diabetes mellitus, clopidogrel loading dose regimen, use of amlodipine and platelet count.
Conclusion The CYP2C19*2 loss-of-function polymorphism is associated with a more frequent occurrence of HPR. However, the part of the interindividual variability in on-treatment platelet reactivity explained by CYP2C19*2 genotype is modest.
- Clopidogrel
- CYP2C19
- CYP2C19*2
- genetics
- platelet function testing
- high on-treatment platelet reactivity
- platelets
- antiplatelet treatment
Statistics from Altmetric.com
- Clopidogrel
- CYP2C19
- CYP2C19*2
- genetics
- platelet function testing
- high on-treatment platelet reactivity
- platelets
- antiplatelet treatment
Introduction
The large interindividual variability in the response to clopidogrel is mainly attributable to the variable extent to which its active metabolite is formed. Both a CYP2C19*2 carrier status as well as the presence of high on-treatment platelet reactivity (HPR) have been associated with recurrent atherothrombotic events following coronary stent implantation.1–5 It is unknown whether genotyping or platelet function testing is superior in tailoring clopidogrel therapy in the individual patient. Genotyping and platelet function testing each have potential advantages for the optimisation of clopidogrel therapy. CYP2C19 genotyping provides reproducible results that are stable over time, regardless of clinical presentation, whereas the individual platelet reactivity status represents the sum of multiple clinical factors and CYP2C19 genotype.
We have performed CYP2C19*2 genotyping in the ‘Do platelet function assays predict clinical outcomes in clopidogrel-pretreated patients undergoing elective PCI’ (POPular) study with the aim of determining the relative contribution of CYP2C19*2 carrier status to the interindividual variability in on-treatment platelet reactivity.2
Methods
The study design and methods used for platelet function testing of the POPular study have been described previously.2 In brief, patients with coronary artery disease undergoing elective coronary stent implantation were eligible for inclusion. All patients were adequately pretreated with clopidogrel (75 mg daily for >5 days, or a loading dose of 300 mg ≥24 h or 600 mg ≥4 h before percutaneous coronary intervention (PCI)) and aspirin (80–100 mg daily ≥10 days prior to PCI) unless on long-term anticoagulation with coumarin derivatives. Blood for platelet function testing and genetic analysis was collected from the femoral or radial artery sheath into 3.2% citrate and K3-EDTA anticoagulated tubes, respectively, prior to heparinisation and the administration of glycoprotein IIb/IIIa inhibitors. The primary endpoint was the magnitude of on-treatment platelet reactivity as measured with the VerifyNow P2Y12 assay. A secondary endpoint was on-treatment platelet reactivity as measured with 5 and 20 μmol/l ADP-induced light transmittance aggregometry (LTA) and the PlateletWorks assay. The study protocol complied with the Declaration of Helsinki and was approved by the ethical committee of our institution. All patients gave written informed consent for participation.
Platelet function testing
The absolute level of platelet reactivity during treatment with clopidogrel (ie, on-treatment platelet reactivity) was quantified using ADP-activated, aggregation-based platelet function tests that were able to predict clinical outcome in the POPular study—that is, 5 and 20 μmol/l ADP-induced LTA (n=1005 and n=1006, respectively), the PlateletWorks assay (Helena Laboratories, Beaumont, Texas, USA; n=511, due to irregularities in supply) and the VerifyNow P2Y12 assay (Accumetrics, San Diego, California, USA; n=1010). HPR to ADP was defined according to the receiver operator characteristics curve based cut-offs determined for HPR based on 1-year clinical outcome—that is, aggregation >42.9% for 5 μmol/l ADP-induced LTA, >64.5% for 20 μmol/l ADP-induced LTA, >80.5% for the PlateletWorks, and P2Y12 reaction units (PRU) >236 for the VerifyNow P2Y12 assay.2 5
CYP2C19 genotyping
Genomic DNA was isolated from EDTA blood followed by identification of the CYP2C19*2 (681G→A, rs4244285) allele using real time PCR. DNA sequence analysis was used to validate the genotyping procedure. CYP2C19*2 genotypes were available for 1024 patients. The CYP2C19 wild-type (*1/*1) occurred with a frequency of 72.0%, while 25.4% were heterozygous for CYP2C19*2 (*1/*2), and 2.6% were CYP2C19*2 homozygotes (*2/*2). These genotype frequencies did not deviate from the Hardy–Weinberg equilibrium (χ2=0.50, p=0.48).
Statistics
Data are presented as mean±SD for continuous variables and as counts (%) for categorical variables. The Student t test and χ2 test were used to test the association of various clinical variables with on-treatment platelet reactivity (p<0.10)—that is, age (10 years), gender, body mass index (BMI, kg/m2), current smoking, hypertension (systolic blood pressure (BP) >140 mm Hg or diastolic BP >90 mm Hg), diabetes mellitus, left ventricular ejection fraction (LVEF) <45%, renal failure (creatinine level >1.36 mg/dl), platelet count, mean platelet volume, clopidogrel dosing regimen, proton pump inhibitor use, and use of the calcium channel blocker amlodipine.6 7 Differences in the magnitude of on-treatment platelet reactivity between the three CYP2C19 genotype groups were tested with analysis of variance (ANOVA) followed by the least significant difference (LSD) post-hoc test.
Multivariate linear regression analysis with calculation of the adjusted β coefficient and coefficient of determination (R2) was used to identify the independent contribution of each of the above-mentioned factors to the interindividual variability in on-treatment platelet reactivity. Furthermore, multivariate binary logistic regression analysis was used to compute adjusted ORs with corresponding 95% CIs (ORadj (95% CI)) for exhibiting HPR compared to not exhibiting HPR, adjusting for the above mentioned variables. All statistical analyses were performed with SPSS V.15.0; two-sided p-values <0.05 were considered significant.
Results
Genetic data was available in 1024 of 1069 patients enrolled in the POPular study. Table 1 shows patient characteristics stratified by CYP2C19*2 genotype.
Patient characteristics stratified by CYP2C19*2 genotype
The mean±SD magnitude of on-treatment platelet reactivity was higher in CYP2C19*2 heterozygotes (44±14%, 63±13%, 72±27% and 230±71 PRU) and homozygotes (52±14%, 70±9%, 90±21% and 257±60 PRU) compared to patients not carrying the CYP2C19*2 gene variant (38±14%, 56±15%, 61±30% and 202±76 PRU, for 5 and 20 μmol/l ADP-induced LTA, the PlateletWorks assay and the VerifyNow P2Y12 assay, respectively; figure 1). Furthermore, HPR was more frequent in patients carrying the CYP2C19*2 genetic polymorphism (table 2).
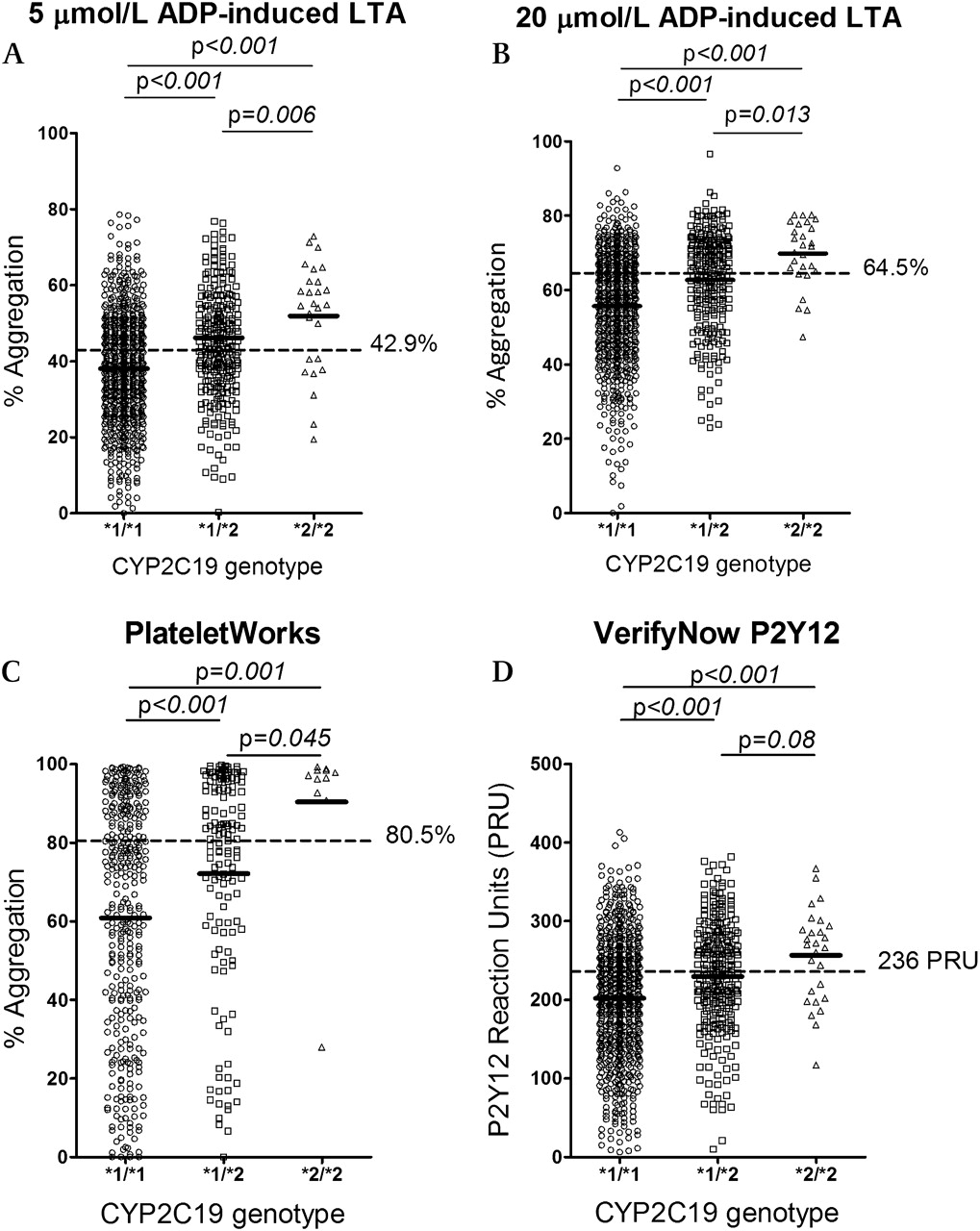
Individual values (n=1024) of on-treatment platelet reactivity stratified by CYP2C19 genotype, as measured with 5 μmol/l ADP-induced light transmittance aggregometry (LTA) (A), 20 μmol/l ADP-induced LTA (B), the PlateletWorks assay (C) and the VerifyNow P2Y12 assay (D). Differences in mean platelet reactivity were tested for significance using analysis of variance (ANOVA) followed by the least significant difference (LSD) post-hoc test. Mean values of platelet reactivity are represented by solid lines and dashed lines indicate cut-off values for high on-treatment platelet reactivity based on 1-year clinical outcome.2
Frequency of HPR stratified by CYP2C19 genotype
Contribution to on-treatment platelet reactivity
CYP2C19*2 carrier status alone could explain 5.0%, 6.2% and 4.4% of the interindividual variability in 5 and 20 μmol/l ADP-induced LTA and the PlateletWorks assay, respectively, compared to 13.0%, 15.2% and 5.6% when clinical factors were included as well (table 3). The whole blood VerifyNow P2Y12 assay demonstrated a smaller contribution of CYP2C19 genotype; 3.7% of the variability in PRU could be attributed to CYP2C19*2 carrier status, which increased more than fivefold to 20.6% after adding clinical variables. The clinical variables independently associated with the magnitude of on-treatment platelet reactivity were age, BMI, gender, diabetes mellitus, clopidogrel loading dose regimen, use of a proton pump inhibitor or amlodipine, and platelet count (table 4).
Percentage of the variability in on-treatment platelet reactivity explained
Contribution to on-treatment platelet reactivity
Predictors of HPR
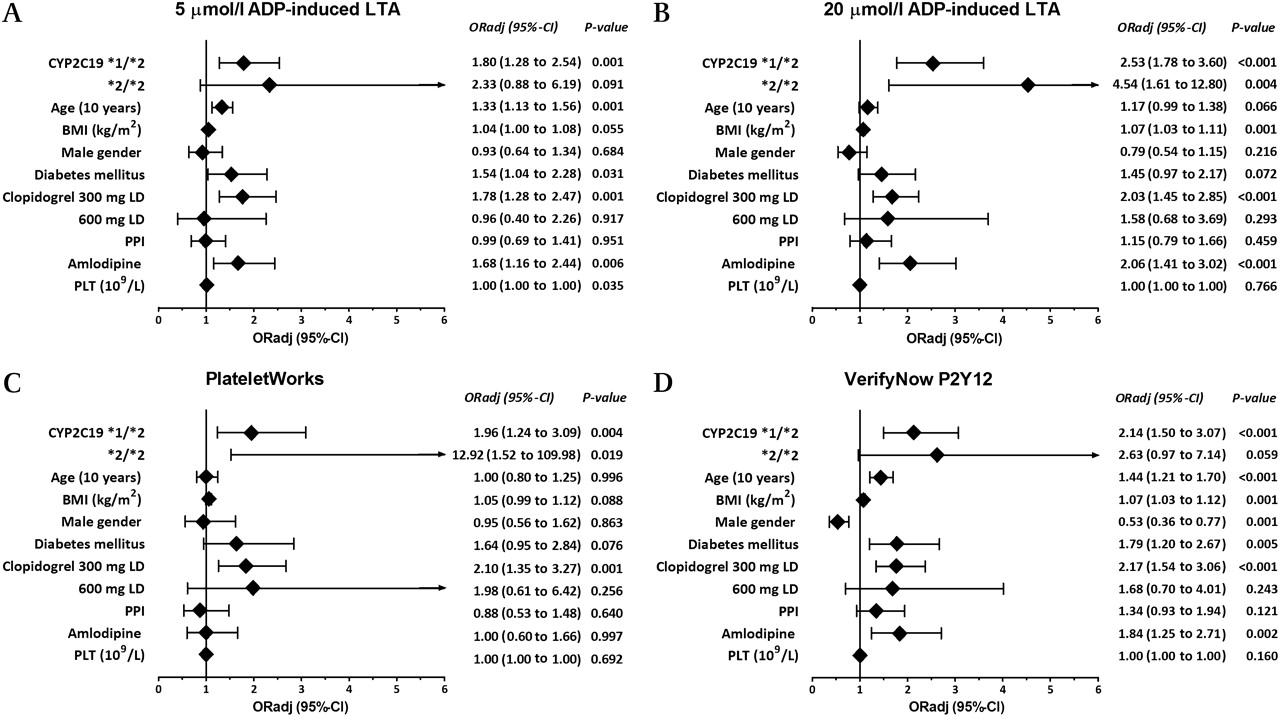
Multivariate logistic analysis showed that the CYP2C19*2 heterozygotes (*1/*2 genotype) had an approximately twofold increase in the occurrence of HPR as compared to the patients with the *1/*1 genotype; this association was stronger for patients carrying two copies of the CYP2C19*2 gene variant. Besides CYP2C19*2 genotype, multiple clinical variables could be identified as independent predictors of HPR, including age, BMI, gender, diabetes mellitus, clopidogrel loading dose regimen, use of amlodipine and platelet count (figure 2).
{kind=link}
{kind=link}
Predictors of high on-treatment platelet reactivity (HPR). Adjusted ORs with corresponding 95% CIs (ORadj (95% CI)), per unit for multinomial and continuous variables) for exhibiting HPR versus not exhibiting HPR as determined with 5 μmol/l ADP-induced light transmittance aggregometry (LTA) (A), 20 μmol/l ADP-induced LTA (B), the PlateletWorks assay (C) and the VerifyNow P2Y12 assay (D), using a multivariate binary logistics model containing CYP2C19*2 carrier status (*1/*1, *1/*2 or *2/*2) in addition to clinical variables that were associated with on-treatment platelet reactivity in multivariate linear regression (p<0.05). CYP2C19 *1/*2 and *2/*2 genotypes were compared with *1/*1 genotype; clopidogrel loading dose, either 300 mg or 600 mg, was compared with 75 mg daily maintenance dose regimen. BMI, body mass index; LD, loading dose; PLT, platelet count; PPI, proton pump inhibitor; PRU, P2Y12 reaction units.
Discussion
An inadequate response to clopidogrel is mainly attributable to the variable formation of its active metabolite. The CYP2C19*2 loss-of-function polymorphism leads to reduced generation of the active metabolite of clopidogrel, and both the loss-of-function CYP2C19*2 genetic polymorphism as well as HPR have repeatedly been shown to be associated with an increased rate of atherothrombotic events following coronary stenting.1–5 Though CYP2C19 is regarded as the most important enzyme in the metabolic activation of clopidogrel, the present study shows that CYP2C19*2 carrier status could only explain approximately 5% of the variability in the pharmacodynamic response to clopidogrel. In addition to CYP2C19*2 genotype, multiple clinical variables could be identified as independent predictors of HPR, with adjusted ORs closely approximating that for heterozygote carriers of the CYP2C19*2 allele. Combining these clinical variables with CYP2C19*2 carrier status yielded a two- to five-fold increase in the percentage of the variability in on-treatment platelet reactivity that could be explained.
Hochholzer and colleagues recently published a similar approach using 5 μmol/l ADP-induced LTA, a platelet function test previously shown to correlate only very modestly with plasma levels of the active metabolite of clopidogrel, which is an important concern when estimating the relative contribution of CYP2C19*2 genotype affecting the generation of the active metabolite of clopidogrel.8 ADP (20 μmol/l) induced LTA and the VerifyNow P2Y12 assay have been shown to correlate better with in vivo plasma levels of the active metabolite of clopidogrel.9 Furthermore, all four platelet function tests included have shown to be capable of predicting clinical outcome in clopidogrel-treated patients.2
The VerifyNow P2Y12 assay is performed in whole blood, thereby more closely mimicking the in vivo situation than LTA, and is not hampered by pre-analytical variables such as pipetting, centrifugation and agonist sources, as is the case for LTA.10 Therefore, we hypothesised that a larger part of the interindividual variability of on-treatment platelet reactivity could be attributed to CYP2C19*2 carrier status when platelet reactivity was measured using the VerifyNow P2Y12 assay. The opposite appeared to be true, as the variation in PRU explained by CYP2C19*2 carrier status alone was lower than for LTA (3.7%), while the combination of CYP2C19*2 carrier status and clinical risk factors could explain as much as 20.6% of the interindividual variability in PRU.
The percentage of variability in on-treatment platelet reactivity as measured with PlateletWorks that could be attributed to CYP2C19*2 genotype and clinical variables was low. Although PlateletWorks has shown to be capable of predicting clinical outcome in the POPular study, the lack of association with different variables known to affect platelet reactivity and to contribute to the interindividual response to clopidogrel, renders interpretation of data difficult.
It has previously been postulated that 73% of the interindividual variability in the pharmacodynamic response to clopidogrel is genetically determined.11 Assuming the straightforward relationship between CYP2C19 and the pharmacodynamic effects of clopidogrel as stated above, it is remarkable that only 5% of the response to clopidogrel could be attributed to the CYP2C19*2 genetic polymorphism. The effects of an impaired enzyme activity associated with the CYP2C19*2 genotype was especially evident in CYP2C19*2 homozygotes. In March 2010, the Food and Drug Administration (FDA) issued a boxed warning to the label of clopidogrel (Plavix), stating that a higher dose of clopidogrel or alternative antiplatelet drugs should be considered in patients who can be classified as poor metabolisers based on CYP2C19 genotyping—that is, patients carrying two CYP2C19 loss-of-function gene variants.12 For CYP2C19*2 heterozygotes, however, the relation with on-treatment platelet reactivity is less profound, and the established on-treatment platelet reactivity in this patient group is characterised by a similar magnitude of intersubject variability as observed in patients without the CYP2C19*2 loss-of-function allele. The present study shows that besides CYP2C19*2 genotype, also clinical variables and the use of concomitant medication known to interfere with generation of the active metabolite of clopidogrel contribute significantly to the degree of on-treatment platelet reactivity. Furthermore, temporary and ongoing clinical disease states alter an individual's intrinsic platelet reactivity status and this may lead to a higher need for platelet inhibition. For example, diabetes mellitus is characterised by a high intrinsic platelet reactivity status, and several lines of evidence suggest that diabetic patients benefit more from stronger antiplatelet therapy compared to patients without diabetes mellitus.13 The genetics substudy of the PLATelet inhibition and patient Outcomes (PLATO) trial constituted the largest cohort of clopidogrel-treated patients in whom CYP2C19 genotyping was performed (n=5148) until now.14 Patients carrying at least one CYP2C19 loss-of-function allele had a worse clinical outcome at 30 days follow-up than patients not carrying such a gene variant (primary endpoint reached in 5.7% vs 3.8%, respectively, p=0.028); however, no clinical consequences were observed at 1-year follow-up (primary endpoint reached in 11.2% vs 10.0%, respectively, p=0.25). The large interindividual variability in the response to clopidogrel can be considered as a matter of systems pharmacology rather than a single-gene determined phenomenon, and prediction of an individual's response to clopidogrel may require integration of information on genetics and clinical variables, both captured in an individual's on-treatment platelet reactivity status. Moreover, the finding that only a small percentage of variability could be attributed to CYP2C19 genotype encourages the search for additional genetic factors explaining the highly variable response to clopidogrel, enabling us to accurately and effectively tailor clopidogrel therapy to the individual patient's need.
In conclusion, the CYP2C19*2 loss-of-function polymorphism is associated with a higher on-treatment platelet reactivity, though the percentage of the interindividual variability in on-treatment platelet reactivity explained by CYP2C19*2 genotype is modest. Prospective studies will have to determine the role of CYP2C19 genotyping and platelet function testing in tailoring clopidogrel therapy and predicting the clinical outcome of clopidogrel treated patients.
References
Footnotes
HJB and AMH contributed equally to this study.
Competing interests JWvW reported speakers fees from Accumetrics and Siemens, The Medicines Company; NJB reported speakers fees from Siemens; JMtB reported speakers fees from Sanofi-Aventis, Eli Lilly, BMS and MSD, Sanofi-Aventis, Eli Lilly, Schering-Plough and GlaxoSmithKline. None of the other authors reported disclosures.
Provenance and peer review Not commissioned; externally peer reviewed.