Article Text

Abstract
Background The exact form of the association between systolic blood pressure (SBP) and heart failure (HF) risk in the elderly remains incompletely defined, especially in individuals not receiving antihypertensive drugs.
Objective To examine the association between SBP and HF risk in the elderly.
Design Competing-risks proportional hazards modelling of incident HF risk, using 10-year follow-up data from two NIH-sponsored cohort studies: the Cardiovascular Health Study (inception: 1989–90 and 1992–3) and the Health ABC Study (inception: 1997–8).
Setting Community-based cohorts.
Participants 4408 participants (age, 72.8 (4.9) years; 53.1% women, 81.7% white; 18.3% black) without prevalent HF and not receiving antihypertensive drugs at baseline.
Main outcome measures Incident HF, defined as first adjudicated hospitalisation for HF.
Results Over 10 years, 493 (11.2%) participants developed HF. Prehypertension (120–139 mm Hg), stage 1 (140–159 mm Hg), and stage 2 (≥160 mm Hg) hypertension were associated with escalating HF risk; HRs versus optimal SBP (<120 mm Hg) in competing-risks models controlling for clinical characteristics were 1.63 (95% CI 1.23 to 2.16; p=0.001), 2.21 (95% CI 1.65 to 2.96; p<0.001) and 2.60 (95% CI 1.85 to 3.64; p<0.001), respectively. Overall 255/493 (51.7%) HF events occurred in participants with SBP <140 mm Hg at baseline. Increasing SBP was associated with higher HF risk in women than in men; no race–SBP interaction was seen. In analyses with continuous SBP, HF risk had a continuous positive association with SBP to levels as low as 113 mm Hg in men and 112 mm Hg in women.
Conclusions There is a continuous positive association between SBP and HF risk in the elderly for levels of SBP as low as <115 mm Hg; over half of incident HF events occur in individuals with SBP <140 mm Hg.
- Epidemiology
- hypertension
- heart failure
- risk stratification
Statistics from Altmetric.com
Hypertension is the most prevalent heart failure (HF) risk factor in the elderly and carries the highest population-attributable risk together with coronary heart disease (CHD).1–4 Anti-hypertensive treatment effectively prevents HF in the elderly,5 6 the population segment with the worst rates of hypertension control.7 The Joint National Committee on Prevention, Detection, and Treatment of High Blood Pressure 7 (JNC-7) identifies systolic blood pressure (SBP) as the primary focus for blood pressure control in the elderly, with a target of <140 mm Hg in the general population and stricter targets for those with diabetes or renal disease.8
Population studies have quantified the impact of high SBP on HF risk. In most studies, SBP has been treated as a categorical factor based on prevailing guidelines.1 3 9–11 However, in younger populations, the association between SBP and HF risk appears to be continuous,12–15 consistent with the concept of ‘prehypertension’.16 To date, studies investigating SBP as a continuous predictor of risk have assumed a linear association.17–19 For prevention efforts, this assumption has drawbacks, because a constant benefit from reduction across the spectrum of SBP values is implied. Importantly, no study has accounted for the competing risk of death in the elderly, in whom mortality may exceed HF risk.3 Thus, a conventional approach can lead to inflated estimates for SBP-associated hazards20 and an unrealistic benefit-to-risk ratio of antihypertensive treatment with the goal of HF prevention. Also, putative reductions in HF risk at low SBP may be offset by increases in risk of stroke or myocardial infarction in the elderly.
In this study, we use 10-year follow-up data from two community-based cohort studies, the Cardiovascular Health Study (CHS) and the Health, Ageing, and Body Composition (Health ABC) Study, to investigate the association between SBP and HF risk among elderly individuals not receiving antihypertensive treatment at baseline. Accounting for the competing risk of death, we examined SBP both as a categorical risk factor, according to the JNC-7 classification, and also as a continuous risk factor in linear and non-linear forms. We also assessed stroke and myocardial infarction as the end point of interest to examine for increases in risk at the lower end of SBP distribution and provided specific data on HF risk for the major demographic subgroups. In secondary analyses, we examined the association of SBP with HF with preserved and reduced left ventricular ejection fraction (LVEF) and explored the potential role of pulse pressure in determining HF risk in SBP subgroups.
Methods
Study population
The design and rationale of CHS has been previously published.21 Briefly, non-institutionalised people aged 65–100 years were recruited from Medicare eligibility lists and examined at four field centres in Forsyth County, North Carolina; Sacramento County, California; Allegheny County, Pennsylvania and Washington County, Maryland). An original cohort of 5201 participants was recruited in 1989–90 and a second cohort of 687 black participants was recruited in 1992–3 (total, 5888 participants; 2495 men, 3393 women). The Health ABC Study is a community-based cohort of 3075 individuals aged 70–79 years at inception. Participants were identified from a random sample of white Medicare beneficiaries and all age-eligible black residents in designated zip codes surrounding Pittsburgh, Pennsylvania and Memphis, Tennessee. To be eligible, participants had to report no difficulty in walking one-quarter of a mile or climbing 10 stairs without resting. Exclusion criteria included difficulties with activities of daily living, obvious cognitive impairment or intention of moving within 3 years. Baseline data were collected in 1997–8. Cardiovascular disease at baseline was based on ICD 9-CM, as reported by Medicare and Medicaid Services for the years 1995–8, self-reported history and use of medication using methods similar to CHS.21
For this analysis, we created an individual-level joint dataset from CHS and Health ABC for participants without prevalent HF who were not receiving anti-hypertensive drugs at baseline—that is, diuretics, β blockers, calcium channel blockers, α blockers, ACE inhibitors, angiotensin receptor blockers or other vasodilators. We did not include participants receiving medication because duration of treatment and class-dependent effects would influence the association. Prevalent HF was adjudicated on the basis of self-report, drugs and review of medical records.22 From the 5888 CHS participants we excluded those (1) with prevalent HF (n=275); (2) receiving (n=2554) or with missing data on (n=7) antihypertensive drugs; (3) of non-white, non-black race (n=19) because of very small numbers and (4) with missing SBP data (n=4). From the 3075 Health ABC participants we excluded those (1) with HF (n=95) or inadequate data to adjudicate HF (n=45) at baseline; and (2) receiving (n=1543) or with missing data on (n=13) anti-hypertensive drugs. The final cohort for this analysis comprised 4408 participants. To align observation periods, we used 10-year data from both studies. In Health ABC, adjudicated outcomes were available for 10 years for the Pittsburgh site and 8 years for the Memphis site at the time of analysis. For incident stroke and myocardial infarction we examined subsets of participants who were free of stroke (n=4270; 96.9%) and myocardial infarction (n=4191; 95.1%), respectively, at baseline.
Risk factor definitions
All definitions were harmonised for the two cohorts except for left ventricular hypertrophy (LVH). Blood pressure was calculated as the average of two seated measurements. In accordance with JNC-7, SBP was classified as normal (<120 mm Hg), prehypertension (120–139 mm Hg), stage 1 (140–159 mm Hg) and stage 2 hypertension (≥160 mm Hg).8 Among those with SBP <140 mm Hg, 20/2930 (0.7%) had diastolic blood pressure ≥90 mm Hg and met the diastolic blood pressure criterion of hypertension; however, for the purposes of this study, these participants were classified according to their baseline SBP. Pulse pressure was defined as SBP minus diastolic blood pressure from the average of two seated measurements.
Race was self-defined. Smoking was classified as current, past (≥100 lifetime cigarettes) or never. Diabetes was defined as self-reported history or use of antidiabetic drugs. Electrocardiographic LVH in CHS was diagnosed with the Minnesota code 3.1 criteria.23 In Health ABC, LVH was diagnosed with the following criteria: R >26 mm in V5 or V6; or R >20 mm in I, II, III, or aVF; or R >12 mm in aVL; or R in V5 or V6 plus S in V1 >35 mm. Heart rate was recorded from the ECG. Prevalent CHD was based on (1) history of bypass surgery or percutaneous intervention; (2) ECG evidence of myocardial infarction and (3) history of myocardial infarction or angina accompanied by use of anti-anginal drugs. In CHS, in addition to a review by the field doctor and classification of pre-baseline events, all information was centrally adjudicated.22
Outcomes
Methods used to assess events in CHS, including HF, have been previously reported.24 25 In Health ABC, all participants were asked to report admissions and every 6 months were contacted to elicit information about interim events. For this analysis, all first admissions with an overnight stay confirmed to be related to HF were classified as incident HF. The CHS events committee adjudicated all events in CHS; in Health ABC, the diagnoses were locally adjudicated. In both studies, the adjudicators reviewed all pertinent data, including history, physical examination, chest radiography report and medication use.25 An HF event was confirmed if, in addition to a doctor's diagnosis, there was (1) documentation of symptoms (such as shortness of breath, fatigue, orthopnoea) and physical signs (such as oedema, rales); (2) supporting clinical findings (such as pulmonary oedema on chest x-ray examination) or (3) HF treatment, including diuretics, digitalis, ACE inhibitors or β blockers. Methods to assess incident stroke and myocardial infarction in CHS and Health ABC have been previously reported.26 27
Neither cohort systematically assessed LVEF during HF hospitalisations. Data on LVEF were extracted from cardiac imaging results (echocardiography, radionuclide ventriculography or angiography) reported in the medical record and therefore refer to various methods. Therefore, LVEF-specific results are subject to selection and method bias. For the purposes of our secondary analyses, we defined LVEF<0.45 as reduced and LVEF ≥0.45 as preserved.
Statistical analysis
We examined the association between SBP and HF in proportional hazards models with death as a competing event using the competing risks model proposed by Fine and Gray,28 a semiparametric model for the subdistribution hazard of the event of interest, interpreted similarly to the Cox model. Cumulative incidence of HF was calculated according to Coviello and Boggess.29 We examined SBP both as a categorical (based on JNC-7) and as a continuous variable. In multivariable models we controlled for all baseline characteristics, as described in table 1, and cohort. To explore the appropriate form of association (linear vs non-linear) of SBP with HF risk, we used fractional polynomial and restricted cubic splines to model SBP.30 Unlike linear associations, the HR (‘subhazard ratio’ for competing risks models) between two points of the curve in non-linear associations varies. Thus, we calculated subhazard ratios (SHRs) between relevant points of the SBP–HF risk curve for these models. We examined interactions of SBP with sex and race in unadjusted and adjusted models. For analyses specific to HF with reduced and preserved LVEF, we treated incident HF with undefined LVEF or LVEF of the opposite type as a competing event. To compare the corresponding SHRs for HF with reduced versus preserved LVEF for each SBP category we used an asymptotic z test. To evaluate the role of pulse pressure in the development of incident HF in conjunction with SBP, we modelled pulse pressure as a continuous variable in the entire cohort and in the SBP <140 mm Hg and ≥140 mm Hg subpopulations in models including SBP. Finally, to examine for regression dilution secondary to the long time frame of the observations (10 years), we obtained hazard estimates for incident HF over the first 5 years and compared these estimates with the 10-year estimates using asymptotic methods. Proportionality of hazards was examined using interaction terms with time. To avoid bias possibly introduced by omission of participants with incomplete data (n=236; 5.4% of the analysis sample), we fitted the multivariable competing risks models in five imputed datasets. For imputation, we used chained equations,31 32 and then obtained parameter estimates by combining the estimates from the five imputed datasets to account for error in missing-value analysis.33 A two-sided p<0.05 was deemed significant. All analyses were performed with STATA 11 (StataCorp).
Baseline participant characteristics
Role of the funding source
The funding agencies had no role in the design and conduct of this study; in the collection, management, analysis and interpretation of the data; and in the preparation of this manuscript.
Results
Study population
Mean age of the subjects was 72.8 (4.9) years; 53.1% were women, 81.7% were white. Table 1 presents the baseline characteristics. Average SBP was 133 (20) mm Hg and was similar between men and women; however, SBP was higher in black than white participants (136 (20) mm Hg vs 132 (20) mm Hg; p=0.001). Among the 4408 participants, 1165 (26.4%) had normal SBP, 1765 (40.0%) had prehypertension, 1049 (23.8%) had stage 1 and 429 (9.7%) had stage 2 hypertension at baseline. The distribution was not different between sexes (figure 1); however, black race was associated with a shift towards more severe SBP categories.

Distribution of baseline systolic blood pressure.
Heart failure incidence
Over 10 years of follow-up, 493 (11.2%) participants developed HF. Figures 2A,B show the probability and absolute number of HF events, respectively, for each SBP category. There was a gradual increase in the proportion of participants developing HF across the escalating SBP categories (figure 2A). Most HF events, however, were observed in those with prehypertension (186/493 (37.7%) HF events); this was consistent in women (87/211 (41.2%)) and in men (99/282 (35.1%)) (figure 2B). Overall, 255/493 (51.7%) HF events occurred in those with SBP <140 mm Hg.

(A) Proportion and (B) absolute number of participants who developed heart failure (HF) over 10 years by baseline systolic blood pressure category (JNC-7 classification).
JNC-7 blood pressure category and heart failure risk
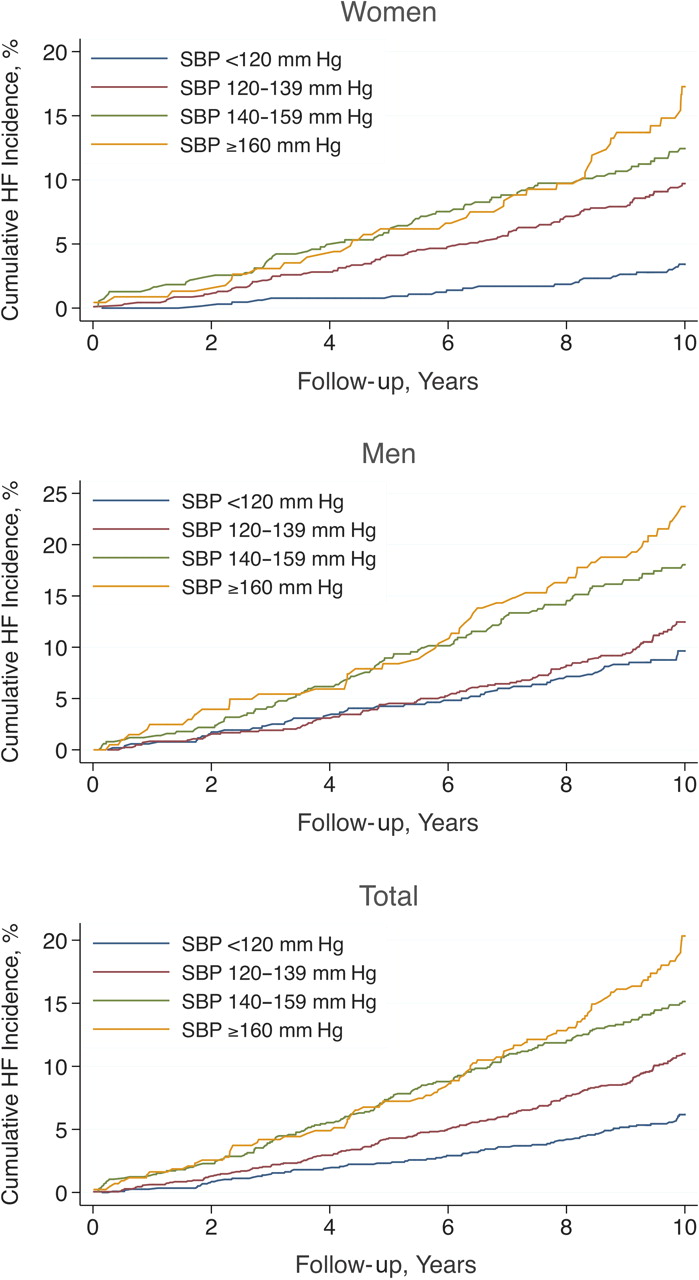
Figure 3 presents the cumulative estimates for incident HF, after accounting for the competing risk of death, according to baseline SBP category. In unadjusted models (table 2), prehypertension was associated with elevated risk for HF (SHR=1.83; 95% CI 1.39 to 2.41; p<0.001); risk was even more pronounced for those with stage 1 and stage 2 hypertension. In models controlling for all characteristics described in table 1, the association of SBP category with HF risk was modestly attenuated (table 2); prehypertension was still associated with increased risk (SHR=1.63; 95% CI 1.23 to 2.16; p<0.001).
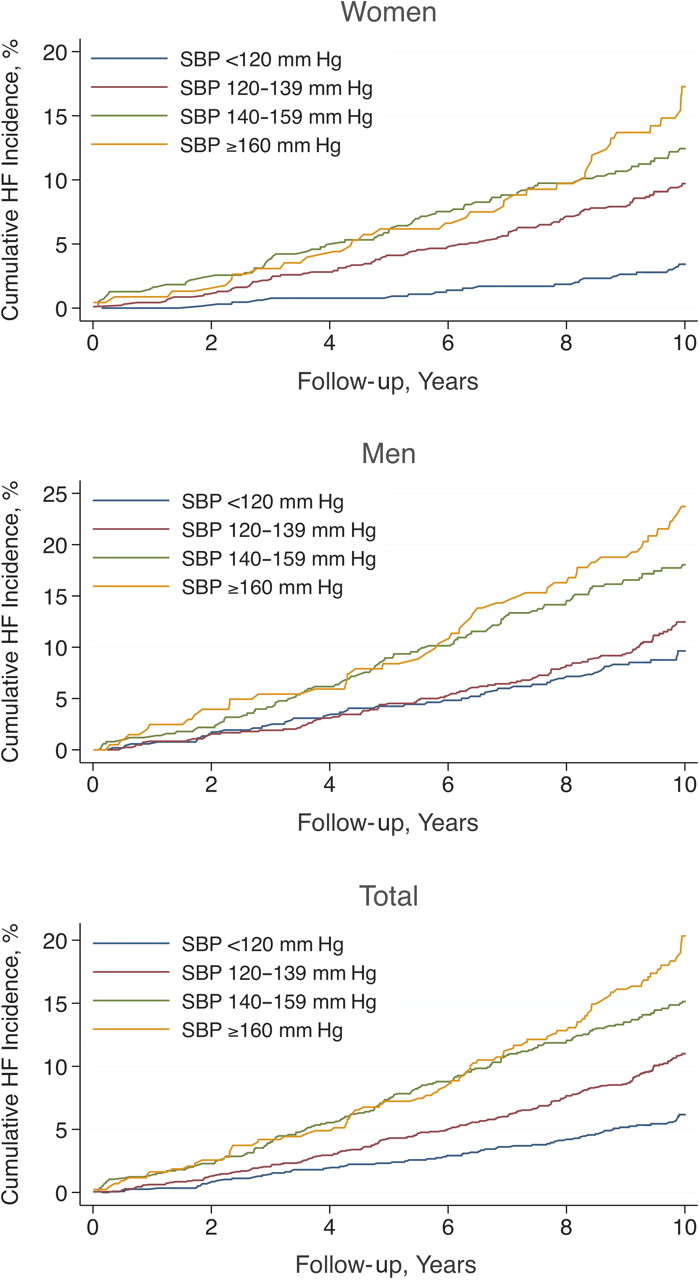
Cumulative incidence of heart failure, adjusted for death as a competing risk, by baseline systolic blood pressure (SBP) category (JNC-7 classification).
Baseline systolic blood pressure by JNC-7 categories and risk for incident heart failure
High levels of SBP were associated with higher HF risk in women relative to men (table 2); the significance of the interaction terms was p=0.004, p=0.028 and p=0.036 in unadjusted and p=0.021, p=0.097, p=0.105 in adjusted models, for prehypertension, stage 1 and stage 2 hypertension, respectively. The elevated HF risk in men with prehypertension did not reach statistical significance (table 2). There was no race-dependent effect of baseline SBP category on HF risk (p>0.7 for all interaction terms in unadjusted and adjusted models). The proportional hazards assumption was marginally violated in unadjusted models (joint significance of SBP category–time interaction terms, p=0.034), mainly because the risk of participants with stage 1 hypertension demonstrated a slight convergence over time (figure 3); this was attenuated in multivariable analyses (joint significance of SBP category–time interaction terms, p=0.060).
Continuous systolic blood pressure and heart failure risk
In multivariable competing risks models, the association between SBP and HF risk was better represented using non-linear forms of association. Model fit significantly improved over the simple linear form when a spline with two knots (three degrees of freedom) was used to express the association of SBP with HF risk. As shown in figure 4, this form assumes a plateau at the ends of the distribution. For SBP values ranging from 113 to 177 mm Hg in men and 112 to 179 in women, HF risk increased continuously (within 95% confidence limits) with increasing SBP. This SBP range represents 84.8% of men and 83.2% of women in the study population. The improvement in model fit with use of restricted cubic splines justified the increase in model complexity (increase in Wald χ2=27.14; increase in degrees of freedom=2; p<0.001). Modelling SBP using a second-degree fractional polynomial resulted in improvement in model fit over the simple linear form but to a lesser degree (increase in Wald χ2=11.72; increase in degrees of freedom=3; p=0.008). There was no evidence of a differential form of association between sex or race subgroups (joint significance for the spline interaction terms, p=0.49 and p=0.89, for sex and race, respectively). SHRs (ie, the HR for incident HF accounting for the competing risk of death) between clinically relevant points of the SBP–HF risk curve in adjusted models are presented in table 3. Among participants with baseline SBP 140 mm Hg, risk for HF was 50% higher (95% CI 28% to 76%) relative to those with SBP 120 mm Hg; this association was stronger in women (table 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Systolic blood pressure at baseline (in mm Hg) and incident heart failure risk adjusted for death as a competing risk. The curves represent restricted cubic splines with two knots (three degrees of freedom). The reference line (HR=1.0) represents risk when systolic blood pressure is equal to the group average (133 mm Hg).
Continuous systolic blood pressure and risk for incident heart failure: multivariable-adjusted subhazard ratios
Continuous systolic blood pressure and risk for stroke and myocardial infarction
In the subset without stroke at baseline (n=4270), 352 (8.2%) participants experienced a stroke over 10 years. There was no evidence of a non-linear association between SBP and risk of stroke in univariate and multivariate competing risks models. A 10 mm Hg increase in baseline SBP was associated with 22% (95% CI 17% to 28%; p<0.001) increase in risk for stroke in univariate and 17% (95% CI 11% to 24%; p<0.001) in multivariate analysis. In the subset without myocardial infarction at baseline (n=4191), 346 (8.3%) participants experienced a myocardial infarction over 10 years. Similar to the association of SBP with HF risk, the association between SBP and risk for myocardial infarction was better represented using a restricted cubic spline. For SBP values ranging from 109 to 169 mm Hg, risk for myocardial infarction increased continuously (within 95% confidence limits) and levelled off beyond these limits. Among participants with SBP 140 mm Hg, risk for myocardial infarction was 46% higher (95% CI 8% to 98%; p=0.014) relative to those with SBP 120 mm Hg; among those with SBP=160 mm Hg, risk for myocardial infarction was 62% higher (95% CI 23% to 113%; p=0.001) relative to those with SBP=140 mm Hg.
Systolic blood pressure and risk for heart failure with preserved and reduced left ventricular ejection fraction
Data on LVEF were available for 297/493 participants (60.2%) at the time of incident HF. Among these events, 158 (53.2%) occurred with LVEF <0.45 and 139 (46.8%) with LVEF ≥0.45. Despite numerical differences in the SHR for HF with preserved and reduced ejection fraction for the escalating SBP categories, there was no statistical evidence of a differential association between SBP and HF of a specific type (online supplementary table 1).
Pulse pressure and incident heart failure risk
The association of pulse pressure with incident HF was linear. In the entire study population, pulse pressure did not add to HF risk prediction when SBP was included in the model (SHR per 10 mm Hg, 1.08; 95% CI 0.98 to 1.20; p=0.12). In the subpopulation with SBP ≥140 mm Hg at baseline, pulse pressure was associated with HF risk independent from SBP (SHR per 10 mm Hg, 1.16; 95% CI 1.02 to 1.32; p=0.023), whereas in the subpopulation with SBP <140 mm Hg no association was observed (SHR per 10 mm Hg, 0.99; 95% CI 0.84 to 1.17; p=0.92); however, the interaction term did not reach statistical significance (p=0.28).
Hazard estimates during 5 versus 10 years of follow-up
In analyses with 5-year HF events as the outcome of interest, the SHR estimates for SBP were not statistically different from those obtained in the main analysis (10-year HF events). Detailed estimates are provided in the online supplementary table 2.
Discussion
In this study, we observed a graded, continuous association between baseline SBP and risk for HF in the elderly. Prehypertension was associated with an increased risk for HF compared with those with optimal SBP (<120 mm Hg) in models accounting for the competing risk of death and controlling for other risk factors. This association was stronger for women. Importantly, >50% of HF events occurred among participants with SBP <140 mm Hg; those with prehypertension accounted for 37.7% of total events. In analyses with SBP as a continuous variable, a non-linear form best represented the association between SBP and HF risk. Pulse pressure contributed to HF risk only in participants with SBP ≥140 mm Hg at baseline.
Increasing levels of SBP within the normal range have been shown to predict death from cardiovascular causes. In the Multiple Risk Factor Intervention Trial, a strong association between SBP >110 mm Hg and CHD mortality was evident among men aged 35–57 years. Prehypertension has been associated with HF risk also.13–15 However, those studies were in younger populations. The vast majority of HF cases occur among the elderly,34 and extrapolating findings from younger cohorts has limitations. In frail populations, mortality exceeds HF incidence,3 35 36 diminishing the benefit of interventions.20 Prehypertension was associated with elevated HF risk in this study despite adjustment for risk factors and competing mortality. Importantly, there was no evidence of a differential association between SBP and HF with preserved versus reduced LVEF in our study, although these findings need to be interpreted with caution because of the lack of systematic assessment of LVEF during HF hospitalisations.
In our study, we observed that the majority of HF events were encountered in participants with SBP <140 mm Hg and that prehypertension was associated with elevated HF risk, especially among women. If these findings are replicated, they may have therapeutic implications. From a pathophysiological perspective, the association between a risk factor and the outcome is rarely characterised by a ‘step’ function; usually it is continuous, but not necessarily linear. We observed that SBP has a continuous association with HF risk for levels as low as 113 mm Hg in men and 112 mm Hg in women. Risk for stroke or myocardial infarction did not increase at these levels of SBP. These findings are consistent with other observational studies37 showing no threshold for the association between SBP and vascular mortality down to 115 mm Hg SBP, with no offset from non-vascular mortality. Notably, the RR associated with SBP diminishes with increasing age37; however, absolute risk was higher among older individuals. Interestingly, augmented blood pressure response to exercise in older individuals is associated with improved survival.38 Whether this has also an impact on HF risk stratification is currently unknown.
In concordance with the ‘prevention paradox’, >50% of HF occurred among participants with baseline SBP below the currently proposed target for treatment. Although both the relative benefit and benefit-to-risk margin from antihypertensive treatment is greater for individuals with SBP ≥140 mm Hg,39 treating only those individuals might lead to a missed opportunity to prevent a large proportion of HF events. Targeting individuals at risk for HF may achieve larger relative benefit and benefit-to-risk margin for HF prevention in elderly individuals with SBP <140 mm Hg, although such a strategy should be prospectively investigated. For example, the ACCORD trial results40 do not support aggressive SBP control in all patients with hypertension and diabetes. These results temper the enthusiasm for SBP control beyond the current guidelines, but also underline the importance of alternative strategies for targeting high-risk individuals. In this respect, a targeted treatment strategy for individuals at high-risk for HF—for example, using the validated Health ABC HF Risk Score,41 42 merits further study. Although one needs to be cautious when extending the results of observational associations to prospective benefit with treatment, it is encouraging that a recent meta-analysis demonstrated that the reduction in risk achieved with SBP lowering in clinical trials is similar to that expected from epidemiological data.39 Importantly, in a recent single-centre randomised study, reduction of blood pressure already in the normal range led to further regression of left ventricular mass, lending further support to our findings.43
Interestingly, in patients with manifest HF there is an inverse association between SBP and mortality.44 The paradoxical effect of high blood pressure in manifest HF is not exclusive to blood pressure (eg, similar trends have been observed for lipid levels and body mass index).45 46 The exact mechanism of this differential association of SBP with risk for incident versus manifest HF outcomes is not well known and needs further study.
There are several limitations in our study. Because we observed outcomes over 10 years, regression dilution due to interim treatment and changes in SBP and incident events (eg, myocardial infarction) may have affected our estimates.47 However, although interim treatment and events obviously modify risk for HF, we intentionally used only baseline information in our analysis. The rationale is that in this study we did not attempt to establish a mechanistic link between SBP and HF, which is a well-established link, but focus on epidemiology and clinical information that might potentially be used for population and individual prevention efforts based on projected risks. Notably, in sensitivity analyses performed with 5-year outcomes, we did not observe substantial differences in comparison with 10-year hazard estimates. Because LVEF during HF hospitalisation was not systematically assessed in either cohort, analyses specific to HF with preserved and reduced ejection fraction are subject to bias. On the other hand, large studies have demonstrated that outcomes and resource utilisation rates are comparable in HF with preserved and impaired ejection fraction, and therefore, discriminating between these two types of HF is less crucial from a public health perspective. Definition of HF was based on hospitalisation in our study; thus, HF incidence was probably underestimated. Our results refer to an elderly cohort and thus do not apply to younger populations. Finally, the number of black participants was relatively small.
In conclusion, over half of the incident HF events in this elderly cohort developed in those with baseline SBP <140 mm Hg. Prehypertension was associated with elevated HF risk, especially among women. A continuous association between SBP and HF risk was observed for levels as low as <115 mm Hg in both sexes. Selected elderly individuals at high risk for HF may benefit from tighter SBP control; however, this strategy needs to be prospectively investigated.
References
Footnotes
Funding This research was supported by contract numbers N01-HC-85079 through N01-HC-85086, N01-HC-35129, N01 HC-15103, N01 HC-55222, N01-HC-75150, N01-HC-45133, grant U01 HL080295 from the National Heart, Lung, and Blood Institute, with additional contribution from the National Institute of Neurological Disorders and Stroke (Cardiovascular Health Study), and contract numbers N01-AG-6-2101, N01-AG-6-2103, N01-AG-6-2106 from the National Institute of Ageing (Health ABC Study). A full list of the Cardiovascular Health Study investigators and institutions can be found at http://www.chs-nhlbi.org/pi.htm. This research was also supported in part by the Intramural Research Program of the NIH, National Institute on Ageing, by an Emory University Heart and Vascular Board grant entitled ‘Novel Risk Markers and Prognosis Determination in Heart Failure’, and by PHS Grant UL1 RR025008 from the Clinical and Translational Science Award program, NIH, National Center for Research Resources.
Competing interests There are no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years, and no other relationships or activities that could appear to have influenced the submitted work.
Ethics approval This study was conducted with the approval of the corresponding study sites of the Cardiovascular Health Study and Health ABC Study.
Provenance and peer review Not commissioned; externally peer reviewed.