Article Text

Abstract
Background Bivalirudin reduces bleeding events and is associated with a lower mortality than the combination of unfractionated heparin (UFH) and glycoprotein IIb/IIIa inhibitor during primary percutaneous coronary intervention (PCI). However, the effect of adding UFH in patients with ST elevation myocardial infarction (STEMI) treated with bivalirudin during primary PCI is unknown.
Methods Patients enrolled in the national Swedish Coronary Angiography and Angioplasty Registry who underwent primary PCI due to STEMI with bivalirudin as anticoagulant were evaluated. Patients were divided into two groups: those treated with bivalirudin only and those treated with bivalirudin plus a bolus dose of UFH.
Results 2996 patients were included in the study: 1928 (64%) received only bivalirudin and 1068 (36%) received bivalirudin plus a bolus dose of UFH. The primary combined endpoint of death or target lesion thrombosis at 30 days occurred more often in the bivalirudin group (11.3% vs 6.5%, OR 0.55, 95% CI 0.41 to 0.72, p<0.001). This difference remained significant after adjustment (HR 0.64, 95% CI 0.44 to 0.95, p=0.03). Death at 30 days and definite target lesion thrombosis at 30 days did not differ between the two groups after adjustment (9.2% vs 5.1%, adjusted HR 0.66, 95% CI 0.42 to 1.03, p=0.07 and 2.3% vs 1.5%, adjusted HR 0.59, 95% CI 0.27 to 1.33, p=0.21, respectively).
Conclusion An additional bolus dose of UFH is associated with a lower rate of death or definite target lesion thrombosis at 30 days in patients undergoing primary PCI with bivalirudin as anticoagulant.
- Coronary angioplasty (PCI)
- anticoagulation
Statistics from Altmetric.com
Background
Primary percutaneous coronary intervention (PCI) is the treatment of choice for patients presenting with ST elevation myocardial infarction (STEMI) within 12 h from onset of symptoms.1 Anticoagulation is needed during the procedure in order to minimise the risk of thrombotic complications. The combination of unfractionated heparin (UFH) with a glycoprotein IIb/IIIa platelet receptor inhibitor is considered the gold standard antithrombotic treatment for this type of patient.1–3 Bivalirudin is a direct thrombin inhibitor that reduces bleeding events when administered during PCI in patients with stable angina or non-STEMI.4 5 The HORIZONS-AMI open-label prospective randomised trial recently showed that bivalirudin reduced the rate of major bleeding in patients treated with primary PCI due to STEMI compared with the combination of UFH and a glycoprotein IIb/IIIa inhibitor.6 Patients treated with bivalirudin had significantly higher rates of acute stent thrombosis (1.3% vs 0.3%), but this had no effect on the balance between safety and efficacy at 30 days. The mortality at 30 days was also lower in the bivalirudin group, probably because of a reduction in the major bleeding rate. Although the administration of UFH was not part of the study protocol, more than 65% of the patients randomised to bivalirudin received a bolus dose of UFH before randomisation. The aim of this study was to evaluate retrospectively the effect of the addition of bolus UFH administration to bivalirudin in patients undergoing primary PCI for STEMI.
Methods
All patients with STEMI treated with primary PCI and receiving bivalirudin as anticoagulant in Sweden between 1 May 2005 and 15 September 2009 were evaluated. Patients who received a glycoprotein IIb/IIIa inhibitor or low molecular weight heparin before or during the procedure were excluded from the study. For patients with several primary PCI procedures during the time period, only the first was included in the analysis. Patients who received UFH before or during the procedure were assigned to the bivalirudin plus UFH group. The UFH was administered either at the first medical contact (eg, in the emergency department) or in the catheterisation laboratory after the coronary angiography was performed and the decision to perform primary PCI was taken. Although the doses of UFH were not recorded in the registry, most hospitals in Sweden administer UFH to this group of patients at a dose of 70 IU/kg with a maximum dose of 5000 IU per patient. The decision to administer UFH and the dose regimen was at the discretion of the treating physician. The remaining patients, who received only bivalirudin, were assigned to the bivalirudin group. Patients received a bolus aspirin dose (320–500 mg) and a bolus clopidogrel dose (300 or 600 mg) if not already on these medications, according to local practice.
The interventions were performed according to the widely accepted medical standards and with routine use of stents. Access site (femoral or radial), use of thrombus aspiration devices, distal protection devices and femoral closure devices were at the operating physician's discretion. All data were collected from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). A detailed description of the registry has been presented in previous publications7 and on the registry site (http://www.ucr.uu.se/scaar). SCAAR has recently been incorporated in the larger national SWEDEHEART registry to which all patients hospitalised in cardiac intensive care units and those undergoing cardiac surgery are enrolled.8 In summary, all Swedish patients undergoing coronary angiography and/or angioplasty are registered by the operating physician in the national registry immediately after the procedure. Clinical characteristics, procedural details and outcomes are entered immediately after the procedure. Complications and adverse outcomes observed during hospitalisation are collected. Follow-up of patients is performed by merging the SCAAR registry with other national registries. Date of death was obtained from the national population registry.
Study endpoints
The primary endpoint of the study was the composite of death or definite target lesion thrombosis at 30 days after the index procedure. Definite target lesion thrombosis was defined as new angiographically-verified coronary occlusion in a previously treated lesion leading to a new acute coronary event. In practice, this is the combination of definite stent thrombosis at 30 days according to the Academic Research Consortium definition plus angiographically-proven new target lesion occlusions in patients treated with percutaneous old balloon angioplasty without stent implantation. Secondary endpoints were the separate components of the primary composite endpoint.
Statistical analyses
Baseline characteristics were summarised with medians and IQR for continuous variables and percentages for discrete variables. Cumulative event rates were estimated by the Kaplan–Meier method. To compensate for the non-randomised design of this observational study, propensity score methods were used. The individual propensity scores, defined as the conditional probability of obtaining UFH based on available covariables, were estimated with a multiple logistic regression model. All covariates shown in tables 1 and 2 together with the treating hospital and the year of the procedure were included in the statistical model.
Baseline clinical characteristics of the study population
Procedural characteristics of the study population
Adjusted HRs were estimated from Cox regression models where the propensity score and UFH treatment were entered as covariates. In separate landmark analyses, Cox regression models including propensity score were used for studying events between 30 days and 12 months. A statement of significance implies statistical significance at the 5% level and all reported p values are two-sided. All statistical analyses were performed with the SPSS Version 15.0 software.
Results
During the study period, 19 687 primary PCI for STEMI were performed in 19 153 patients in Sweden. Bivalirudin was given during 3379 procedures. A total of 2996 patients fulfilled the inclusion and exclusion criteria and comprised the study population. Of these, 1928 (64%) received bivalirudin only (bivalirudin group) and 1068 (36%) also received a bolus dose of UFH either before (552 patients) or during (516 patients) the procedure (bivalirudin plus UFH group). The demographic data of the patients are shown in table 1. The patients in the bivalirudin group were older and had higher rates of diabetes, prior myocardial infarction and prior coronary artery bypass surgery than the patients in the bivalirudin plus UHF group.
Procedural characteristics are presented in table 2. Patients in the bivalirudin group had lower rates of complete revascularisation, drug eluting stent implantation, transradial approach during the procedure, use of closure devices (for procedures performed through the femoral approach), use of thrombectomy and a higher rate of concomitant treatment with an intra-aortic balloon pump during the PCI procedures compared with patients in the bivalirudin plus UHF group.
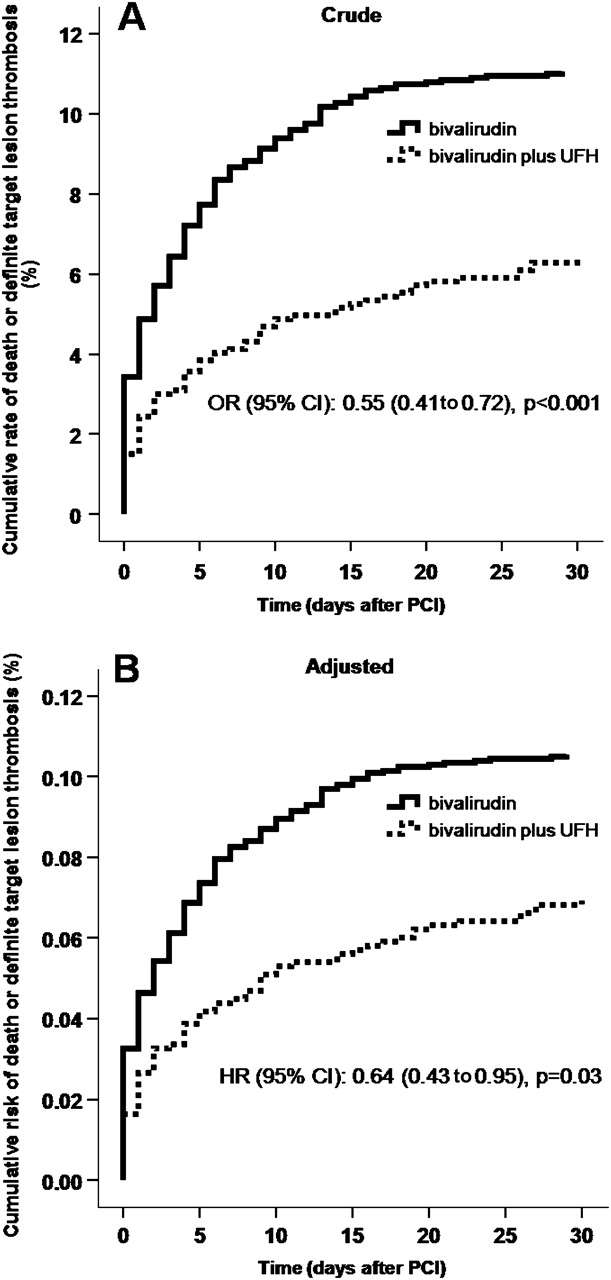
The primary endpoint of death or definite target lesion thrombosis at 30 days was met in 217 patients (11.3%) from the bivalirudin group and 69 patients (6.5%) from the bivalirudin plus UFH group (OR 0.55, 95% CI 0.41 to 0.72, p<0.001, figure 1A).

(A) Crude rate and (B) adjusted risk of death or definite target lesion thrombosis. PCI, percutaneous coronary intervention; UFH, unfractionated heparin.
The secondary endpoint of death within 30 days after the index procedure was met in 177 patients (9.2%) from the bivalirudin group and 54 patients (5.1%) from the bivalirudin plus UFH group (OR 0.52, 95% CI 0.39 to 0.72, p<0.001). At the same time point, 45 patients (2.3%) from the bivalirudin group and 16 patients (1.5%) from the bivalirudin plus UFH group met the second secondary endpoint of definite target lesion thrombosis (OR 0.64, 95% CI 0.36 to 1.01, p=0.12).
Multivariable analyses including a propensity score for receiving UFH were performed in order to compensate for potential confounders inherent to the non-randomised nature of this study. The primary endpoint remained in favour of the bivalirudin plus UFH group (HR 0.64, 95% CI 0.43 to 0.95, p=0.03, figure 1B). The adjustment showed no significant differences in the secondary endpoints of death at 30 days (HR 0.66, 95% CI 0.42 to 1.03, p=0.07, figure 2A) and definite target vessel thrombosis at 30 days (HR 0.59, 95% CI 0.27 to 1.33, p=0.21, figure 2B).

(A) Adjusted risk of death and (B) definite target lesion thrombosis. PCI, percutaneous coronary intervention; UFH, unfractionated heparin.
A landmark analysis from 30 days up to 12 months was performed in order to identify possible differences after 30 days from the index procedure. This analysis showed that all the differences that were seen between the bivalirudin and the bivalirudin plus UHF groups developed within the first 30 days and that thereafter there were no differences in the combined endpoint of death or definite target lesion thrombosis or in any of the separate composites after adjustment (figure 3A–C).

{kind=link}
{kind=link}
{kind=link}
Landmark analysis for (A) the composite of death or definite target lesion thrombosis, (B) death and (C) definite target lesion thrombosis. PCI, percutaneous coronary intervention; UFH, unfractionated heparin.
Bleeding complications, defined as intracranial bleeding, bleeding requiring transfusion or treatment (eg, surgical or prolonged external compression) or leading to prolonged hospitalisation were registered for 23 (1.2%) patients in the bivalirudin group and 16 (1.6%) patients in the bivalirudin plus UFH group (p=0.407).
Discussion
The main finding of this study is that the additional administration of bolus UFH compared with no heparin administration in patients treated with primary PCI for STEMI and receiving anticoagulation with bivalirudin was associated with a lower incidence of death or definite target lesion thrombosis within 30 days after the procedure. A possible explanation is that bivalirudin only cannot provide the appropriate level of anticoagulation in these high-risk patients, mainly due to its short half-life (approximately 30 min in patients with normal renal function).
As mentioned above, approximately two-thirds of the patients randomised to bivalirudin in the HORIZONS-AMI study received a bolus dose of UFH before PCI. Heparin administration, although used in a non-randomised way, resulted in a reduced rate of major adverse cardiovascular events at 30 days after the procedure (4.6% in patients who received UFH vs 7.2% in patients who received only bivalirudin, p=0.08 for interaction of UFH vs not).6 This beneficial effect was not followed by a concomitant increase in the rate of the protocol-defined major bleedings (4.8% in those treated with UFH plus bivalirudin vs 5.2% in those receiving only bivalirudin). Furthermore, this post hoc analysis showed that patients randomised to bivalirudin and treated with an additional bolus UFH dose had a lower rate of acute stent thrombosis than those not receiving a bolus UFH dose (0.9% vs 2.6%, p=0.006).9
The results of our study provide further data on the role of UFH in addition to bivalirudin in a large-scale real-life population of patients undergoing primary PCI for STEMI, adjusted for differences in baseline characteristics with a multivariable analysis including propensity score. These results suggest that bivalirudin used as the antithrombotic regimen during primary PCI for STEMI can be supplemented with a bolus dose of UFH. The fact the UFH and bivalirudin co-administration was not associated with more bleeding complications provides a favourable safety profile in this combination.
Although primary PCI is generally accepted as the preferred reperfusion treatment for STEMI, the optimal antiplatelet and anticoagulation treatment for these patients needs to be defined. Despite the large amount of evidence supporting the beneficial effect of glycoprotein IIb/IIIa inhibitors,10 we should keep in mind that most of these studies were performed in patients not pretreated with clopidogrel and even without the routine use of stents.11 12 The previously published BRAVE 3 study,13 which showed no benefit from abciximab versus placebo in reducing infarct size in patients treated with primary PCI receiving a preprocedural loading dose of 600 mg clopidogrel, questioned the role of glycoprotein IIb/IIIa inhibitors during primary PCI. Potent and rapidly acting oral platelet inhibitors such as prasugrel and ticagrelor have recently been shown to reduce thromboembolic events in patients with STEMI when compared with clopidogrel.14 15 Bedside platelet aggregation and coagulation tests may help us to identify patients in whom intensified antiplatelet and anticoagulation treatment may be of benefit.
In this rapidly changing environment, bivalirudin shows a promising profile for the treatment of patients undergoing primary PCI. The reduction of bleeding complications and the simplicity of its use (one bolus dose plus infusion during PCI and discontinuation in the laboratory immediately after the procedure without the need for active clotting time measurements) makes bivalirudin a very attractive regimen. This is particularly true in patients at high risk for bleeding complications such as elderly patients, women and those with renal failure.16 The results of our study indicate, however, that bivalirudin may be inadequate as monotherapy in patients undergoing primary PCI, and the addition of a bolus dose of UFH may be helpful in achieving better efficacy without significant negative interaction with the safety profile. Prospective randomised trials are needed to define this need and to establish the optimal doses and timing of adjunctive heparin in combination with bivalirudin in primary PCI for STEMI.
Limitations of the study
The non-randomised retrospective design of our study is its major limitation. The study population represents only a small proportion of all patients treated with primary PCI during the study period. The fact that the study period began before the publication of the HORIZONS AMI study and that the combination of UHF and a IIb/IIIa inhibitor is still very popular among PCI operators in Sweden may provide an explanation for this finding. The different strategies followed in different Swedish hospitals in treating these patients may also represent a possible bias. The hospital of treatment was entered as a parameter in the propensity score model in order to compensate for this bias. In all observational studies comparing different medical treatments, the result may be influenced by differences in the study groups that are not registered and therefore not possible to include in the statistical model used. The lack of data about the UFH dose used and the different time points of administration (before or during the procedure) may further compromise these study findings.
Conclusion
Compared with no heparin, a bolus dose of UFH was associated with a lower rate of death or definite target lesion thrombosis in patients treated with bivalirudin in the setting of primary PCI in a large real-life population of patients with STEMI. Further prospective randomised clinical studies are needed to clarify the optimal way of using bivalirudin in this group of patients.
References
Footnotes
See Editorial, p 1459
Competing interests None.
Ethics approval This study was performed according to the rules of the Declaration of Helsinki. The participation of the patients in the registry was approved by all hospital ethics committees and informed consent was obtained from all patients before entering their data in the registry.
Provenance and peer review Not commissioned; externally peer reviewed.