Article Text

Abstract
Background The European Society of Cardiology (ESC) recently published revised criteria for ECG interpretation in the athlete.
Objective To examine the performance of the 2010 ESC ECG criteria in a population of athletes undergoing preparticipation cardiovascular disease screening.
Methods University athletes (n=508) underwent routine medical history/physical examination and ECG before athletic participation. Transthoracic echocardiography (TTE) was also performed on each participant to detect or exclude cardiac findings with relevance to sport participation. Screening test statistics were calculated to determine the performance of the 2010 ESC criteria, and the performance of the 2010 criteria was compared with the 2005 criteria.
Results Application of the 2010 ESC criteria, compared with the 2005 criteria, reduced the number of participants with abnormal ECG findings from 83/508 (16.3%) to 49/508 (9.6%). The reduction in the number of abnormal ECGs was driven by the reclassification of participants with isolated QRS voltage criteria for left ventricular hypertrophy from abnormal to normal. Of the 49 participants with abnormal ECGs, 14/49 (29%) had a single ECG abnormality and 35/49 (71%) had two or more abnormalities. The use of the 2010 criteria was associated with improved specificity (reduction in the false positive rate) and preserved sensitivity when compared with the 2005 criteria.
Conclusion Application of the 2010 ESC criteria for ECG interpretation in the athlete improves the accuracy of an ECG-inclusive preparticipation screening strategy by reducing the rate of false positive ECGs.
- Electrocardiography
- risk stratification
Statistics from Altmetric.com
Introduction
Although athletic preparticipation cardiovascular disease screening is universally recommended, guidelines that delineate screening protocols are not uniform.1–3 The most controversial and widely debated issue is whether to add a 12-lead ECG to medical history and physical examination.4 5 The European Society of Cardiology (ESC) and the International Olympic Committee endorse ECG use, whereas the American College of Cardiology (ACC) and the American Heart Association (AHA) do not.
It was recently shown that sudden cardiac death is the leading medical cause of death in university student athletes in the USA.6 In addition, important observational data from the Italian national experience suggest that ECG is an integral component of effective athletic preparticipation screening,7–9 since ECG may identify athletes harbouring cardiovascular disease which increases the risk of sudden cardiac death.10 11 Furthermore, we recently reported the results of a prospective athlete screening study and demonstrated that ECG inclusion significantly improved the sensitivity of preparticipation screening.12 However, the addition of ECG to medical history and physical examination led to a substantial increase in the rate of false positive screening. At the time this previous study was designed, we used the only available consensus-based criteria for ECG interpretation in the athlete.9
Recently, updated recommendations for ECG interpretation in the athlete have been published by the ESC.13 An important objective of this document is to differentiate the benign ECG findings attributable to exercise training from those associated with heart disease. To our knowledge, the performance of these criteria has not been prospectively assessed in a large cohort of echocardiographically phenotyped athletes. Therefore we conducted an analysis to determine the performance of the 2010 ESC criteria in the context of athlete screening. We hypothesised that application of the newly released ECG criteria would lead to a favourable reduction in the rate of false positive testing during ECG-inclusive preparticipation screening.
Methods
Study design
Full methodology of the original study has been previously reported.12 Briefly, athletes were enrolled during 3 consecutive years (2006–2008) and were eligible to participate if they were 18 years or older and were newly matriculated university student athletes. All participants underwent a standardised, non-investigational screening medical history/physical examination based on current ACC/AHA and National Collegiate Athletic Association recommendations.1 Immediately after medical history/physical examination, ECG was performed using standard 12-lead placement and equipment (MAC 5500; GE Healthcare, Milwaukee, Wisconsin, USA). ECG was performed and interpreted by study investigators blinded to the results of medical history/physical examination findings. All participants were followed clinically during sport participation for a minimum of 2 years after enrolment. The institutional review boards of the Partners Human Research Committee and Harvard University approved our study protocol. Written informed consent was obtained from all participants.
Criteria for 12-lead ECG abnormality
Table 1 presents initial and revised ESC criteria for ECG interpretation in the athlete.9 13 For the present analysis, we used the revised ESC criteria.13 These criteria differentiate abnormal ECG patterns into two groups. Group 1 contains common and training-related ECG changes, and group 2 consists of uncommon and training-unrelated ECG changes. A positive (ie, abnormal) ECG was defined on the basis of the presence of one or more of the group 2 findings.
Summary of the 2005 and 2010 European Society of Cardiology criteria for ECG interpretation in the athlete
Cardiac structure, function and pathology
Transthoracic echocardiography (TTE) was used to determine the presence or absence of underlying structural or valvular heart disease with relevance to sports participation risk.14 Each participant underwent focused TTE with commercially available equipment (Vivid I; GE Healthcare) by investigators blinded to the results of medical history/physical examination and ECG. TTE data were used to classify individuals as normal, mildly abnormal (findings consistent with benign exercise-induced cardiac remodelling) or abnormal (findings suggestive of, or diagnostic for, cardiac disease relevant to sport participation risk) using previously reported definitions.12 All participants categorised as abnormal (11/508) were referred for comprehensive non-investigational testing to confirm or exclude true pathology.
Statistical analysis
We calculated screening test statistics, including sensitivity, specificity, negative and positive predictive values, and accuracy, by using 2×2 contingency tables. Specifically, we examined the performance of ECG-inclusive screening for identifying athletes with findings suggestive of, or diagnostic for, underlying cardiac abnormalities. Exact Clopper–Pearson methods were used to calculate 95% CIs. SPSS V.16.0 was used for all analyses.
Results
Study population and echocardiographic findings
There were 508 participants with complete medical history/physical examination, ECG and TTE data. The mean age was 19±0.3 years, and 311/508 were male. The primary ethnicity of participants was characterised as follows: Caucasian (68%), Asian (12%), black/Afro-Caribbean (10%), Latino (5%) and other (5%). Sport-type participation was diverse and typical for a university-level competitive athletics program (figure 1). By TTE, 375/508 (73.8%) participants had structurally normal hearts, 122/508 (24.0%) had evidence of physiological remodelling, and 11/508 (2.2%) had findings suggestive of, or diagnostic for, cardiac disease relevant to sport participation risk. Of these 11, six had valvular heart disease and five had structural abnormality that exceeded the limits of physiological remodelling (marked left ventricular hypertrophy (LVH) (n=2), marked left ventricular dilation (n=2) and right ventricular dilation (n=1)). After further clinically indicated testing in these 11 participants, three met criteria for recommended sport participation restriction with diagnoses of moderate pulmonic stenosis, hypertrophic cardiomyopathy and post-viral myocarditis. On the basis of the finding that 3/508 (0.6%) participants were ultimately found to have pathology necessitating sport restriction, our data suggest that one case of relevant pathology will be detected for every 170 athletes subjected to preparticipation screening. Among the remaining 505 participants (99.4%) who were ultimately cleared for sport participation, no adverse cardiovascular events have occurred through a minimum follow-up period of 2 years.

Distribution of sport-type participation among the 508 participants studied.
Findings during cardiovascular screening
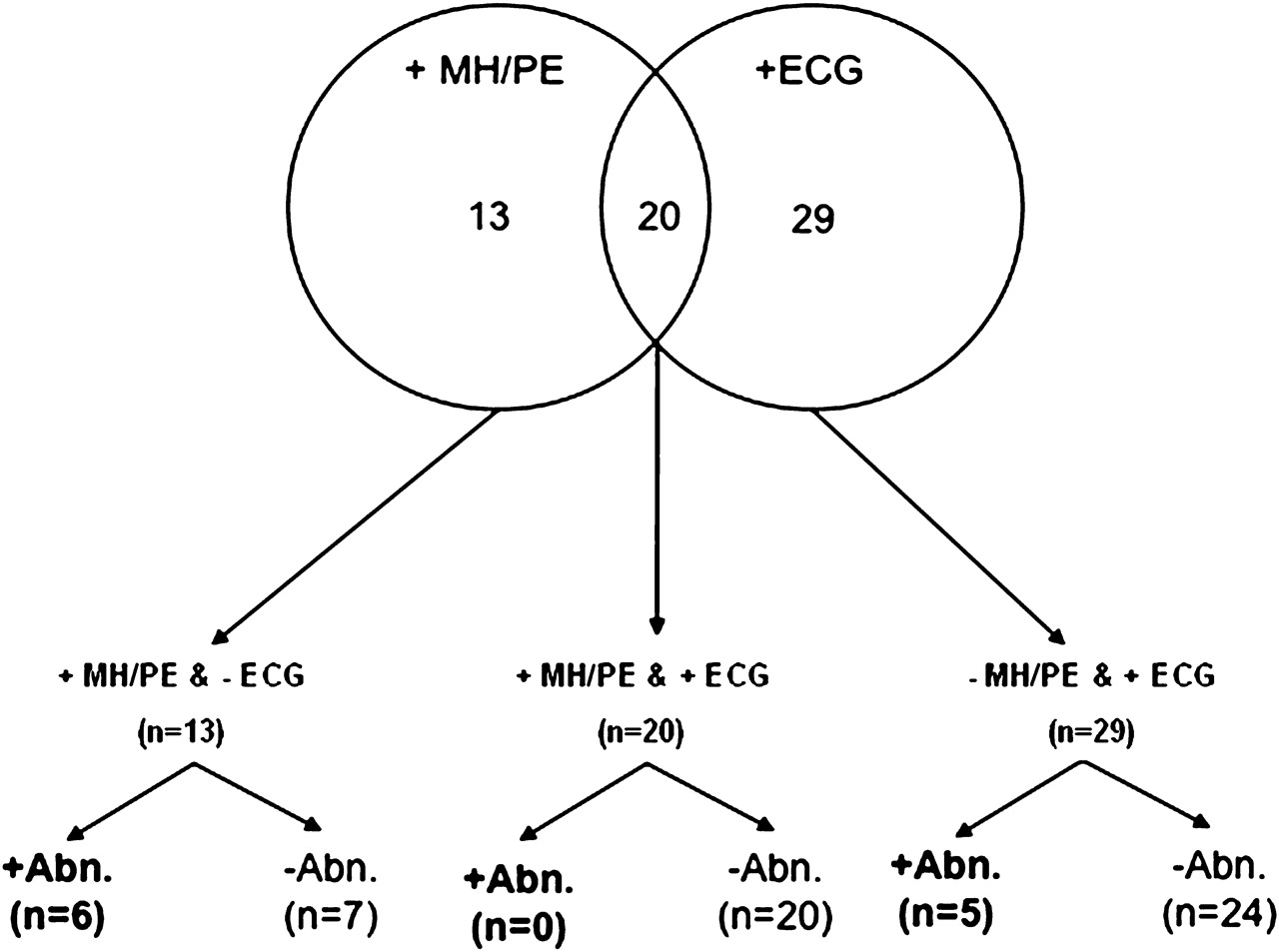
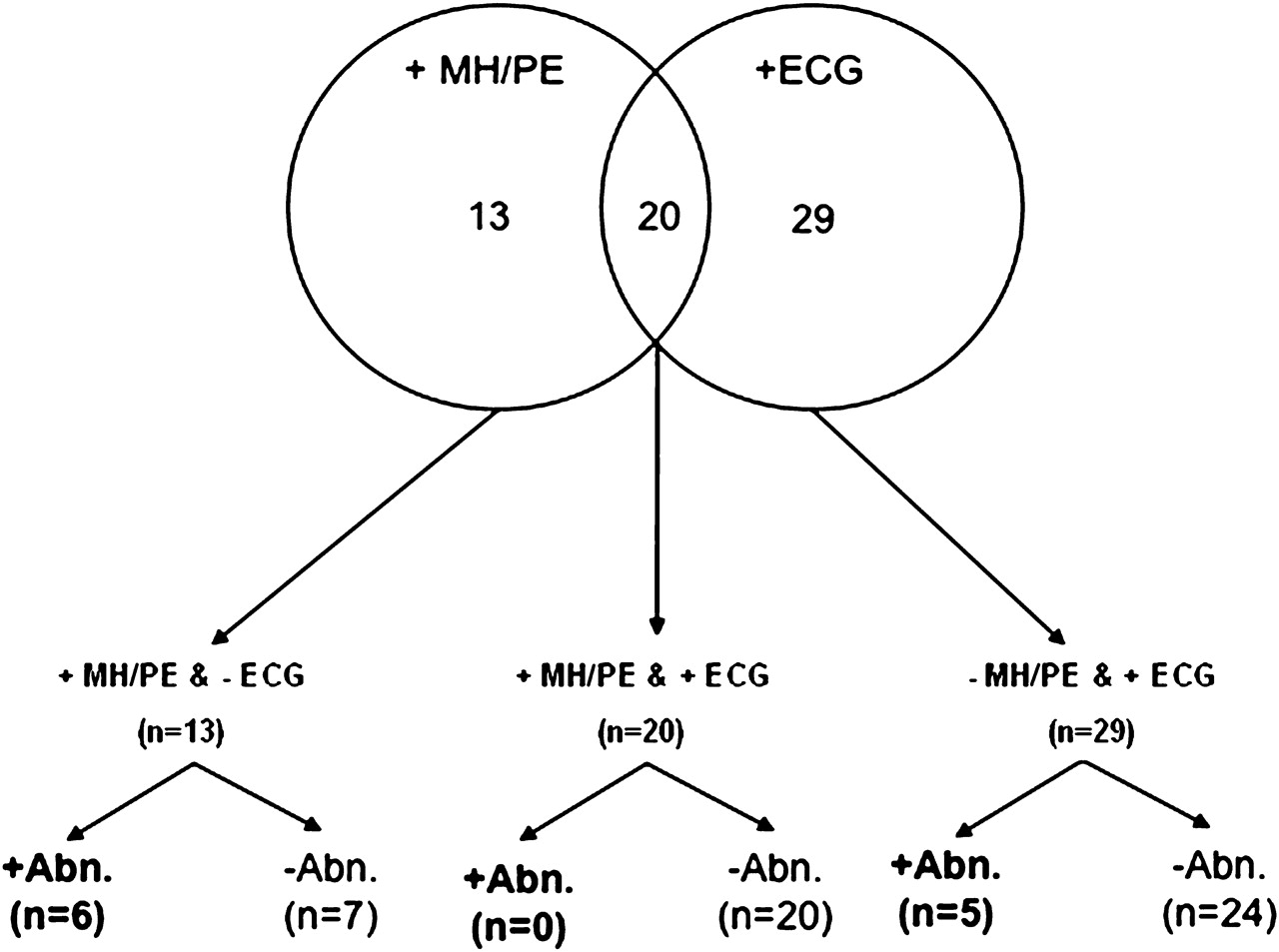
Results of preparticipation screening using medical history/physical examination and the 2010 ESC criteria for ECG interpretation in the athlete are summarised in figure 2. Overall, 62/508 athletes were found to have abnormal findings on either medical history/physical examination and/or ECG. Specifically, 13 participants had abnormal findings only during medical history/physical examination, 29 participants had positive findings only by ECG, and 20 participants had abnormalities both during medical history/physical examination and by ECG. Individuals with valvular heart disease were detected by auscultation during physical examination, and none had abnormal ECG findings. Therefore, of the 11 participants referred for comprehensive non-investigation evaluation based on TTE findings, the six with valvular disease did not have any ECG abnormalities, and the five participants with structural concerns were identified by ECG abnormalities.
{kind=link}
{kind=link}
Results from preparticipation cardiovascular disease screening in 508 athletes using the 2010 European Society of Cardiology criteria for ECG interpretation in the athlete. Abn, participants with transthoracic echocardiographic data suggestive of, or diagnostic for, cardiovascular pathology with relevance to sport participation risk; MH/PE, medical history/physical examination.
Further detail of ECG abnormalities and corollary TTE findings are summarised in table 2. Of the 49 participants with abnormal ECGs, 14/49 (29%) had a single ECG abnormality, and 35/49 (71%) had two or more abnormalities. Seven participants had structurally normal hearts, 37 had physiological remodelling, and five had TTE findings warranting further diagnostic testing. When relegated to further diagnostic testing, pathology with relevance to sport participation was confirmed in two, and the remaining three were judged to have marked physiological remodelling.
Abnormalities discovered on 12-lead ECG in athletes undergoing cardiovascular screening
Comparison of the 2005 and 2010 ESC criteria for ECG interpretation in the athlete
ECG-inclusive preparticipation screening performance characteristics comparing the use of the 2005 with the 2010 ESC criteria are shown in table 3. For identifying subjects (n=11) with findings suggestive of, or diagnostic for, underlying pathology, the 2010 ESC criteria demonstrated improved specificity and preserved sensitivity when compared with the 2005 ESC criteria. Use of the 2010 ESC criteria improved the overall accuracy of ECG-inclusive preparticipation screening by reducing the number of false positive ECG results.
Performance characteristics of athlete preparticipation screening using medical history and physical examination in conjunction with ECG as dictated by the 2005 and 2010 ESC criteria for ECG interpretation in the athlete
Application of the 2010 ESC criteria reduced the number of participants with abnormal ECG findings from 83/508 (16.3%) to 49/508 (9.6%). This reduction was driven solely by reclassification of participants with isolated QRS voltage criteria for LVH (n=34) from the abnormal to the normal ECG group.
Discussion
We recently reported the results of a prospective athlete screening study which demonstrated that the addition of ECG to medical history and physical examination significantly improves the sensitivity of preparticipation screening. However, the inclusion of ECG came at the cost of increased false positive testing and thus reduced overall screening specificity.12 Since the design and execution of this previous study, recommendations for ECG interpretation in the athlete have been updated,13 but have yet to be assessed in a population of athletes phenotyped by non-invasive imaging. We now report an analysis examining the performance of the 2010 ESC ECG criteria in the context of preparticipation screening in a cohort of competitive university athletes. In summary, we found that use of the 2010 ESC criteria resulted in improved specificity (decrease in false positive testing) with preservation of high sensitivity (low rate of false negative testing).
The use of ECG during athlete preparticipation screening remains controversial. Proponents of an ECG-inclusive screening strategy cite limitations of the medical history and physical examination, the ability of ECG to detect occult conditions most commonly associated with sudden cardiac death, and the theoretical argument that detection of underlying disease may reduce the incidence of sudden cardiac death.4 15 16 In contrast, opponents criticise ECG-inclusive screening on the basis of arguments of cost, diagnostic accuracy (low specificity/high false positive rate) and logistical feasibility.5 17 The ability of ECG-inclusive screening to both correctly indentify disease (specificity) and simultaneously clear healthy individuals for sport (sensitivity) remains a central uncertainty in all aspects of this debate. A fundamental determinant of ECG performance in this setting is the definition of what constitutes normal versus abnormal findings on the ECG of a trained athlete.
Increasing recognition of the fact that repetitive exercise training and sport participation lead to physiological cardiac remodelling and attendant ECG changes prompted a recent consensus committee effort to revise athlete-specific ECG normality criteria.13 The principal difference between the recently published 2010 criteria13 and previously proposed criteria9 is the differentiation of the common, exercise-training-related ECG patterns from those more likely to be reflective of underlying cardiac disease. Results from the present analysis confirm that use of the updated ECG criteria improves the performance of ECG when used during preparticipation evaluation of athletes. In our cohort, the improvement in the performance of ECG was attributable to reclassification of athletes with the ECG finding of isolated voltage criteria for LVH from abnormal to normal. There is also emerging evidence that exercise induced cardiac remodelling may have a pathological component.18 19 Further study is warranted to determine if such ‘pathological’ findings have a clinical impact and if any ECG findings may help to identify this type of remodelling.
There are several distinct implications of the present findings. First, our results demonstrate that use of the 2010 ESC criteria reduce the number of false positive ECG tests among trained athletes. Thus, implementation of these criteria during preparticipation screening is warranted if ECG is to be included in screening protocols. Second, data from this analysis may assist individuals involved in the organisation and execution of athlete screening. The reported screening performance characteristics, specifically the reduced but still non-trivial false positive testing rate, may assist with resource allocation including financial budgeting and the provision of follow-up testing. The finding that screening 170 athletes is necessary to detect one relevant case of pathology is consistent with the findings of another recent study evaluating the performance of an ECG-inclusive athlete screening strategy.20 Third, our data confirm the notion that some ECG findings, such as isolated increase in QRS voltage, are common and most often benign among trained athletes. Of the 34 participants in our study with isolated QRS voltage for LVH, none harboured cardiovascular disease. In addition, isolated left atrial enlargement (n=4) and isolated right bundle branch block without repolarisation abnormality (n=8) were not associated with cardiac pathology in any participant. Finally, it is noteworthy that use of the 2010 ESC criteria still resulted in a significant rate of false positive screening (10%). This important fact must be taken into account by the sport organisations and national governing agencies involved in the continued debate over the merits of ECG-inclusive screening.
Study limitations
First, our study population is relatively small compared with previous reports of athlete screening.7 However, the cohort examined in this analysis is the largest athlete group prospectively studied to compare screening strategies for which complete echocardiographic data are available. The ability to examine correlations between screening findings and underlying cardiac structure is required for sound conclusions about screening performance. Second, although no participant had an adverse outcome through 2 years of clinical follow-up, this analysis was not powered to examine the impact of the 2010 ESC criteria on the incidence of sudden cardiac death. The rarity of this catastrophic outcome will necessitate large, ideally multinational efforts for a valid prospective study. Third, we acknowledge the inherent limitations of TTE for the detection of subtle forms of pathology relevant to the athlete, including arrhythmogenic right ventricular cardiomyopathy and hypertrophic cardiomyopathy, which at times can only be detected with MRI.21 22 However, TTE was the only feasible non-invasive imaging technique for this study, and criteria for abnormalities were set conservatively to maximise the likelihood that any participant with potential disease would undergo definitive non-investigational testing (eg, exercise testing, MRI). Finally, the ethnic composition of our study population may not reflect athletes in all geographic regions, and ECG findings in athletes are known to differ based on ethnicity.23–25 Therefore our results may not be directly applicable to screening in all regions.
Conclusions
Compared with previous criteria, application of the 2010 ESC criteria for ECG interpretation in the athlete improves the accuracy of an ECG-inclusive preparticipation screening strategy. The improved performance of ECG was driven by improved specificity (reduced false positive rate), which was attributable to the reclassification of athletes with isolated voltage criteria for LVH, a finding now recognised as common and training-related. Further research aimed at better discriminating training-related from training-unrelated ECG changes may further improve the overall performance of an ECG-inclusive preparticipation screening strategy.
References
Footnotes
See Editorial, p 1540
Competing interests None.
Ethics approval This study was conducted with the approval of the Partners Healthcare and Harvard University.
Provenance and peer review Not commissioned; externally peer reviewed.