Article Text

Abstract
Objective To study the prevalence and medium term outcome of subclinical rheumatic heart disease (RHD) in India.
Design Cross sectional echocardiographic screening study.
Setting School children aged 5–15 years living in rural areas of north India.
Patients A cross sectional echocardiographic screening study was carried out among 6270 randomly selected school children aged 5–15 years (10.8±2.6 years; 52.7% male). Of all the abnormal cases, 100 children (78%) were restudied at a mean follow-up of 15.4±6.6 months.
Intervention Echocardiographic screening.
Main outcome measure Echocardiography–Doppler criteria based prevalence of RHD.
Results Clinical examination detected mitral regurgitation in five patients and the estimated prevalence of clinical RHD was 0.8/1000 school children. Echocardiography–Doppler diagnosed RHD in 128 cases, giving a prevalence of 20.4/1000 school children (95% CI 16.9 to 23.9/1000 children). On multivariate analysis, older age (OR 1.93, 95% CI 1.29 to 2.88; p=0.001), female sex (OR 1.84, 95% CI 1.25 to 2.72; p=0.002) and government funded school student, which is a surrogate measure of lower socioeconomic status (OR 1.55, 95% CI 1.02 to 2.34; p=0.039) were found to be independent predictors of RHD. On follow up, the severity of subclinical RHD was non-progressive in 68 children (68%) while it worsened in four (4%) and regressed in 28 children (28%).
Conclusions The prevalence of RHD is several fold higher using echocardiographic screening compared with clinical examination. The prevalence is higher among girls and children of lower socioeconomic status. In the majority of cases, subclinical RHD appears to be non-progressive on medium term follow up. Routine echocardiographic screening may be indicated in populations at high risk of RHD.
Statistics from Altmetric.com
Introduction
Rheumatic heart disease (RHD) remains a significant cause of cardiovascular morbidity and mortality in the developing countries.1 2 Epidemiological studies from India in the past decade have shown a consistent decrease in the prevalence of RHD.3–5 However, all of these studies are based on clinical screening followed by echocardiographic confirmation. Recent studies from Africa, using echoardiographic screening, have reported a nearly 10-fold higher prevalence of subclinical RHD in children.6 7 The prevalence of subclinical RHD among asymptomatic school children in India is not known. It is suggested that institution of secondary prophylaxis for children with subclinical RHD diagnosed by echocardiography may lessen the burden of RHD.1 8 However, the natural history of subclinical RHD, identified using an echocardiographic screening protocol, is not known.
The suggested risk factors for RHD include overcrowding, poverty and unhygienic living conditions.9 10 Risk factors for RHD in the current era are not well defined. We therefore carried out a large echocardiographic screening survey among asymptomatic school children living in rural areas of north India. The objectives of the study were to estimate the prevalence of clinical and subclinical RHD, to identify risk factors associated with RHD and to study the natural history of children with echocardiographically detected RHD.
Material and methods
This cross sectional epidemiological survey was conducted in primary and secondary schools in the rural areas under Ballabhgarh Block of Haryana, a state located in north India. A scheme called Comprehensive Rural Health Services Project (CRHSP) was established at Ballabhgarh in 1965. Twenty-eight villages with a total population of 85 000 are covered under this comprehensive programme. The estimated number of children aged 5–15 years attending the various primary and secondary schools in this area is approximately 20 000. We randomly selected six out of these 28 villages in the area using a cluster sampling method. We intended to enrol all of the children studying in both government aided and private schools in these six villages. Government aided schools do not charge any fee and provide books, clothing and midday meals to the students free of charge. These facilities do not exist in private schools which charge a monthly fee of approximately US$15–20. The principals of these schools were initially approached with the project details and consent forms. Once the principal agreed, the consent forms were distributed to the parents of children aged 5–15 years. The project team visited the schools prior to the survey to collect consent forms and answer any queries. Parents of only two children refused to undergo the study; the reasons for refusal could not be ascertained. All students aged 5–15 years in the selected schools were examined. Absentees were tracked and included in the study during subsequent visits to the school. The study was approved by the All India Institute of Medical Sciences ethics committee. Enrolment commenced in November 2008 and ended in March 2010.
During the survey, paramedical staff documented demographic and anthropometric data, including height, weight and waist circumference. Using Indian growth charts,11 children below the 25th percentile for age were identified. Body mass index was calculated and a corresponding z score was calculated from age and sex based WHO charts.12 Family history included number of family members, type of house and number of rooms in the house. Houses made of mud and bamboos, which are less robust than a brick built dwelling, were classified as ‘Kutcha’ (a local language term) houses. A brief history was recorded which included history suggestive of rheumatic fever and any cardiovascular symptoms. The on-site cardiologist clinically examined the child. The examination included general physical examination and cardiovascular examination for respiratory distress, cyanosis, cardiomegaly, congestive heart failure, abnormal heart sounds and murmurs. Echocardiography, including colour Doppler, was performed using a portable echocardiography machine (Sonosite M Turbo Model). A standard set of loops and images were stored in digital format for later review. To validate the portable echocardiography machine, the initial 55 children with abnormal finding were brought to the echocardiography laboratory of the Department of Cardiology, All India Institute of Medical Sciences, and were restudied using Philips iE 33 echocardiography equipment (Philips, Bothell, WA, USA). The severity of mitral regurgitation changed from mild to trivial in only one child; in the rest there was excellent agreement. Children with a murmur suggestive of RHD, which was confirmed on echocardiography, were categorised as ‘clinically detected RHD’.
The echocardiography was performed by one of the cardiology investigators with sufficient experience in echocardiography of RHD cases. Images and loops of all cases considered abnormal were analysed independently by two additional cardiologists with extensive experience in diagnosing RHD patients.
Echocardiographic criteria
Criteria to define subclinical RHD using echocardiography (modified WHO criteria)3 included a combination of pathological regurgitation and at least one morphological change suggestive of RHD. Doppler criteria for pathological regurgitation included a regurgitant jet seen in at least two planes, regurgitant jet of >1 cm in length, a mosaic colour jet with a peak velocity of >2.5 m/s and jet persisting throughout systole or diastole. Morphological criteria included leaflet thickening, restricted or excessive motion of leaflets and subvalvular thickening. Other criteria for diagnosing RHD by echocardiography included mitral stenosis, mitral valve involvement with aortic regurgitation and isolated mitral regurgitation with documented history of rheumatic fever. A bicuspid aortic valve was excluded in all children who showed isolated aortic valve involvement on echocardiography. Tricuspid and pulmonary regurgitation were frequent but were not considered as evidence of RHD. If any abnormality was detected either on clinical examination or by echocardiography, the parents were counselled. These children were kept on a 6 monthly medical and yearly echocardiographic surveillance. Children with clinical RHD and those with moderate regurgitation on echocardiogram were advised about antibiotic prophylaxis. Parents of children with subclinical RHD were advised to report sore throat, fever or joint pain immediately to the local health centre.
An attempt was made to restudy all children with abnormal echocardiographic findings suggestive of RHD. A brief history which focused on sore throat, joint pain and cardiovascular symptoms was noted followed by focused clinical examination. A detailed echocardiogram was recorded as in the initial examination.
Statistical methods
The data are presented as mean (SD) or number (%). Prevalence is reported with 95% CIs. A multivariate logistic regression analysis was performed to identify the predictors of RHD in this population. Age, gender, type of school (government or private) overcrowding (defined as >4 persons living in a room), type of house (Kutcha or brick), height/weight below 25th percentile and body mass index z score less than −2 were the pre-identified factors used in the final model. A p value of <0.05 was considered significant. The data were analysed using Stata V.9.0 (College Station).
Results
A total of 6270 children were included in this school survey, of whom 52.65% were boys and mean age was 10.78±2.63 years (range 5–15). Nearly one-third (1908) of children were studying in government funded schools. Baseline characteristics are given in table 1. There was no history of current cardiac symptoms (such as dyspnoea, palpitations, chest pain, syncope, etc) in any of the children. Three children complained of joint pain during the visit but the arthralgia was not suggestive of rheumatic fever. Physical examination revealed a systolic murmur indicative of mitral regurgitation in five subjects, which was subsequently confirmed by echocardiography, accounting for a clinical RHD prevalence of 0.8/1000 school children. None of these children had evidence of cardiac decompensation.
Baseline characteristics of the study subjects
Echo-Doppler diagnosed valvular involvement suggestive of RHD in 128 cases, giving a prevalence of 20.4/1000 school children (95% CI 16.9 to 23.9/1000 children). Thickening of the mitral and/or aortic valve was present in all cases. Of the 128 children, mild mitral regurgitation was found in 101 children and moderate mitral regurgitation in 11 children. Two children had mitral regurgitation and mitral stenosis. One child had isolated mitral stenosis, and it turned out that this child had undergone balloon mitral commissurotomy previously. Eleven children with mitral regurgitation also had aortic regurgitation. Isolated aortic regurgitation in the absence of a bicuspid aortic valve was detected in 14 children. Overall, trivial mitral regurgitation was seen in 255 children. Doppler revealed mild mitral regurgitation in 130 and moderate mitral regurgitation in 11 children. Echocardiographically detected abnormalities are summarised in table 2.
Doppler abnormalities noted in study subjects
Risk factors for RHD
Univariate analysis revealed older age (p<0.001), female gender (p<0.001), studying in government funded school (p<0.001), living in Kutcha houses made of mud/bamboos (p<0.005) and overcrowding as significant predictors of RHD (figure 1). Height or weight <25th percentile, low body mass index z score, waist circumference, history of joint pain and auscultatory abnormalities were not associated with RHD.

The prevalence of rheumatic heart disease (RHD) among various subgroups of children. BMI, body mass index.
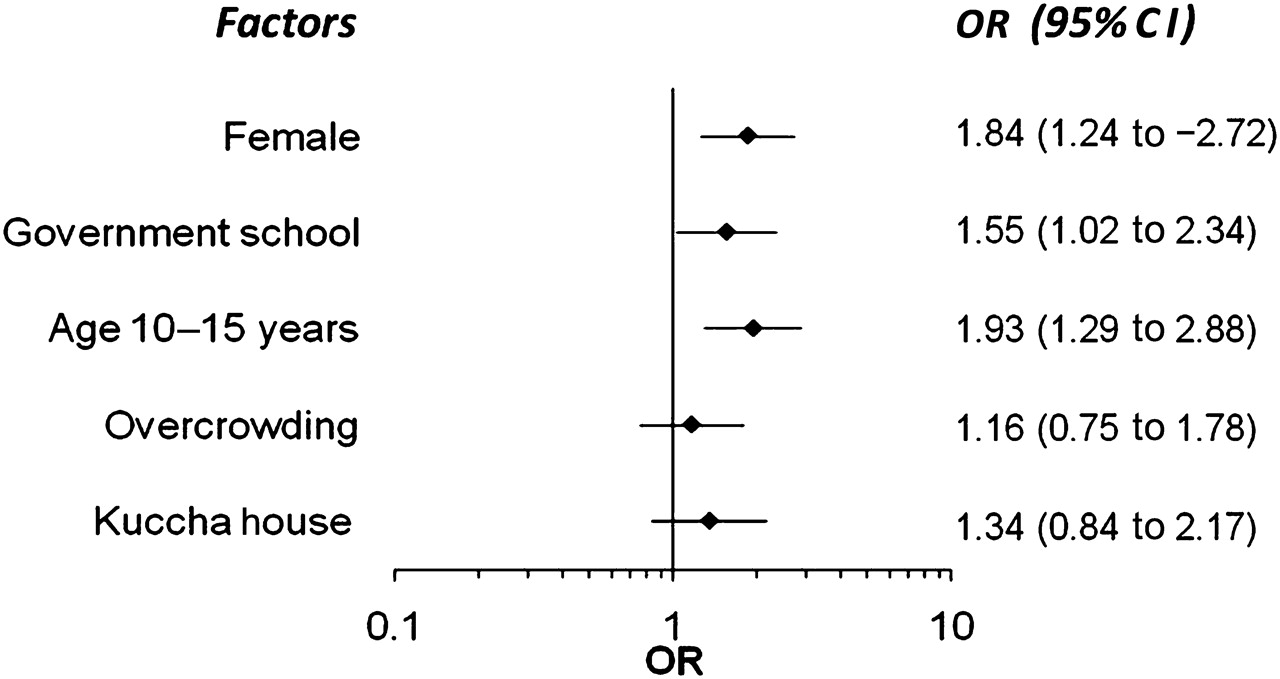
On multivariate analysis, older age (OR 1.93, 95% CI 1.29 to 2.88; p=0.001), female sex (OR 1.84, 95% CI 1.25 to 2.72; p=0.002) and studying in a government funded school (OR 1.55, 95% CI 1.02 to 2.34; p=0.039) were independent predictors of RHD (figure 2). RHD was twice as prevalent among children aged 11–15 years (prevalence of 26.5/1000 children) compared with children aged 5–10 years (12.6 per 1000 children). Girls had a higher prevalence of RHD (27.9/1000 girls; 95% CI 22.3 to 34.5) compared with boys (13.3/1000 boys; 95% CI 9.7 to 17.9). Studying in a government school was the most important factor that nullified the effects of other lower socioeconomic indicators, including living in a Kutcha house, more persons in a family, less number of rooms, more members per room and malnourishment, as quantified by lower waist circumference, lower body mass index z score and <25th percentile for height and weight. The prevalence of RHD among 1908 children studying in Government funded school was 32.5/1000 school children (95% CI 25.0 to 41.5/1000) compared with 15.2 (95% CI 11.8 to 19.2/1000) among 4362 children studying in a private school.
{kind=link}
{kind=link}
Risk factors associated with rheumatic heart disease (RHD) on multivariate analysis. OR and 95% CIs are presented.
Follow-up
Of the 128 cases with RHD, 100 children (78.1%) were restudied at a mean follow-up of 15.4±6.6 months (range 3–27). The other 28 children could not be followed because of refusal by parents (n=6), migration to other cities (n=4) and inability to track despite several house visits (n=18). Of the 100 children followed, one complained of polyarthralgia, but anti-streptolysin O titre and erythrocyte sedimentation rate were normal. None of the children reported worsening of clinical symptoms. On echocardiography, 68 children (68%) had non-progressive valve disease compared with the baseline echocardiograms. The grade of mitral regurgitation worsened from mild to moderate in four cases (4%), without any obvious episode of clinical worsening, sore throat or rheumatic fever. In 28 children (28%), the grade of mitral regurgitation decreased by at least one grade but the structural changes in the valve persisted in 25 of 28 of these children. In one child, aortic regurgitation also regressed.
Discussion
This school survey of children done in a rural area of North India reveals a much higher prevalence of RHD using echocardiography compared with clinical screening. RHD is thought to be on the decline in India because of improving standards of living but the estimated prevalence of echocardiograpically detected RHD in India is comparable with that measured in Mozambique (21.5 cases/1000) but lower than that reported in Cambodia (30.4 cases/1000) in studies similar to ours.6 The exact aetiopathogenesis of rheumatic fever and RHD is not known. It is believed that the genetic and immune system in the host, virulence of the organism, environmental factors and healthcare accessibility determine the prevalence of RHD in a particular region. The fact that the observed prevalence of RHD in India is similar to sub-Saharan Africa suggests that economic betterment may not have translated to improvement in healthcare systems across India.
The reported prevalence of RHD based on clinical evaluation in India varied from 1.8 to 11/1000 school children (average 6/1000) during the 1970s and 1980s, and 1–3.9/1000 during the 1990s.3 Studies in the past decade using echocardiographic validation of clinical diagnosis showed a prevalence of 0.6–0.8/1000, similar to the prevalence of clinical RHD observed in the present study.4 5 It is now well known that the prevalence of echocardiograpically detected RHD is nearly 10 times that of clinically identified cases.6 7 A recent echocardiographic screening study from Bikaner, Rajasthan, India, involving 1059 children, reported a prevalence of 51/1000 using the WHO Doppler criteria alone.13 However, use of Doppler criteria alone may be over sensitive and non-specific for diagnosing RHD. The prevalence of RHD in the Indian subcontinent remains high. A clinical screening study from Pakistan, involving 25 000 children, reported a similar prevalence (21.9 cases/1000)14 and the prevalence may be even higher if echocardiographic screening is done in all children. Previous studies have estimated that the number of children, 5–14 years of age, with RHD in Asia is 1.96 and 2.21 million.15 However, using data from the present study, the estimated number of children with echocardiographically diagnosed RHD in India alone would be nearly 6 million. Hence RHD should be prioritised in developing countries where it remains a leading cause of cardiac morbidity and mortality.16
Recent studies using echocardiographic screening have redefined epidemiological identification of RHD.6 7 It is suggested that early recognition of RHD and institution of penicillin prophylaxis may reduce the clinical impact of RHD. However, this study shows that subclinical RHD remains clinically and echocardiograpically stable in the majority at about 2 years of follow-up, although this is relatively short in the life cycle of RHD which may take decades to manifest itself clinically. Subclinical RHD progressed in only 4% over 2 years and mitral regurgitation regressed in 28% of children in our study. Longer term follow-up is needed, but the outcome on longer term follow-up may be similar as previous studies have shown that patients with ‘mild RHD’ during an episode of rheumatic fever have a favourable prognosis in the long term.17 18 There is no consensus as yet on the management of such subclinical RHD, even though the WHO recommends that in areas where RHD is endemic, echocardiography may be used to diagnose “silent but significant rheumatic carditis of insidious onset” and it is suggested that that such cases be managed as RHD until proved otherwise.1 The cost effectiveness and feasibility of echocardiographic screening and institution of secondary prophylaxis as a population based strategy is not known. Given the favourable prognosis of subclinical RHD, it may be wiser to restrict secondary prophylaxis to patients with clinically detected RHD and/or moderate mitral regurgitation on echocardiography. Patients with morphological abnormalities with trivial or mild regurgitation may be advised to undergo regular medical/echocardiographic surveillance and to report sore throat, joint pain or cardiac symptoms.
The echocardiographic criteria used in this study are modified from the WHO criteria, initially developed for diagnosing subclinical rheumatic carditis.1 Various reports published on echocardiographic screening for RHD have used different sets of criteria.6 7 19 It seems that a combination of Doppler and morphological criteria would be most ideal and will avoid overestimation. However, in regions with a high burden of RHD, these criteria may be too strict and may miss some cases.
Subclinical RHD was more frequent among girls, children of older age and lower socioeconomic status. A higher rate of RHD among girls is well known6 20 but whether it is due to healthcare related gender disparity or to genuine gender related predisposition is not known. An increased risk of RHD with increasing age may represent increased cumulative risk exposure.7 Lower socioeconomic conditions are thought to be important predisposing factors for RHD.9 10 Even though living in Kutcha houses made of mud and bamboos and overcrowding were found to be significant predictors of RHD on univariate analysis, the only independent socioeconomic predictor of RHD was studying in a government funded school.
The major advantage of the present study is that all echocardiograms and clinical evaluation were done by cardiologists with extensive experience of performing echocardiography in RHD patients. The population covered under the area of survey, the number of schools and the number of school children are well defined for the Ballabgarh Comprehensive Rural Health Services Project.
Limitations include the subjective nature of the echocardiographic criteria for diagnosing RHD; the fact that we did not measure the thickness of the mitral leaflets as has been suggested recently.21 The study was carried out in a specific part of India and the results may not be applicable to other parts of India. Furthermore, the follow-up information was only of medium term duration.
Conclusions
Our study confirms that subclinical RHD is present in about 20/1000 children in rural areas near to Delhi. The majority of subclinical RHD lesions did not progress in the medium term follow-up. We do not know the long term impact of these findings but recommend that further cross sectional surveys are performed in other parts of India and cohorts of children are followed-up to understand the long term epidemiology of subclinical RHD.
References
Footnotes
Funding Partial funding from the United Kingdom India Education and Research Initiative (UKIERI). The funding agency had no role in the design or conduct of the study, collection, management, analysis or interpretation of the data, or the preparation, review or approval of the manuscript.
Competing interests None.
Ethics approval The study was approved by the All India Institute of Medical Sciences ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.