Article Text

Abstract
Objective To test the effect of patent foramen ovale (PFO) closure on neurological events in divers.
Design Prospective, non-randomised, longitudinal three-arm study.
Setting Tertiary referral centre.
Population 104 scuba divers with a history of major decompression illness (DCI).
Intervention Transcutaneous PFO closure.
Main outcome measures Baseline and three follow-up examinations with a questionnaire about health status and diving habits/accidents, transoesophageal echocardiography at baseline for PFO grading, cerebral MRI at all examinations.
Results 39 divers had no PFO, 26 had a PFO and chose to undergo percutaneous closure and 39 had a PFO, but decided not to undergo closure. The total number of dives, including those performed before baseline and those during long-term follow-up, was 81 654; 18 394 dives during the follow-up period of 5.3±0.3 years, during which there were a total of five major neurological DCI events–namely 0 in the no PFO group, 0.5±2.5/104 dives in the PFO closure group and 35.8±102.5/104 dives in the PFO no closure group (four events; p=0.045 between the PFO groups). In the groups, no PFO, PFO closure and PFO no closure, there were 1.1±2.6, 0.8±1.4, 3.3±6.9 ischaemic brain lesions, respectively, at follow-up (p=0.039 between the PFO groups)—that is, 16±42/104 dives in the no PFO group, 6±13/104 dives in the PFO closure group and 104±246/104 dives in the PFO no closure group (overall p=0.042; p=0.024 between the PFO groups).
Conclusion PFO closure in continuing divers appears to prevent symptomatic (major DCI) and asymptomatic (ischaemic brain lesions) neurological events during long-term follow-up.
- Patent foramen ovale
- diving
- decompression illness
- neurological events
- coronary stenting
- coronary intervention
- percutaneous valve therapy
- congenital heart disease
- pulmonary hypertension
- echocardiography
- EBM
- cardiac catheterisation
- interventional cardiology
- coronary collateral circulation
- coronary physiology
- coronary flow
- intracoronary Doppler
- Doppler echocardiography
Statistics from Altmetric.com
- Patent foramen ovale
- diving
- decompression illness
- neurological events
- coronary stenting
- coronary intervention
- percutaneous valve therapy
- congenital heart disease
- pulmonary hypertension
- echocardiography
- EBM
- cardiac catheterisation
- interventional cardiology
- coronary collateral circulation
- coronary physiology
- coronary flow
- intracoronary Doppler
- Doppler echocardiography
Introduction
Most of the medical problems in scuba (self-contained underwater breathing apparatus) diving are due to decompression during the diver's ascent. During decompression, gas bubbles grow by expanding pre-existing gas nuclei found at normal atmospheric pressure in joints, the spine, sweat glands and skin pores.1 These tissue bubbles may migrate to the capillary or lymphatic bed and thus, can enter the venous circulatory system. Small gas volumes are filtered by the lungs and exhaled, large ones may escape into the systemic circulation via pulmonary arteriovenous shunts.2 Alternatively, venous gas bubbles may follow the path to the systemic arterial side via an atrial septal defect or a patent foramen ovale (PFO) (figure 1). Of all possibilities for arterialisation of venous gas bubbles, a PFO is the most likely, because a PFO is present in a quarter to one-third of the general population.3
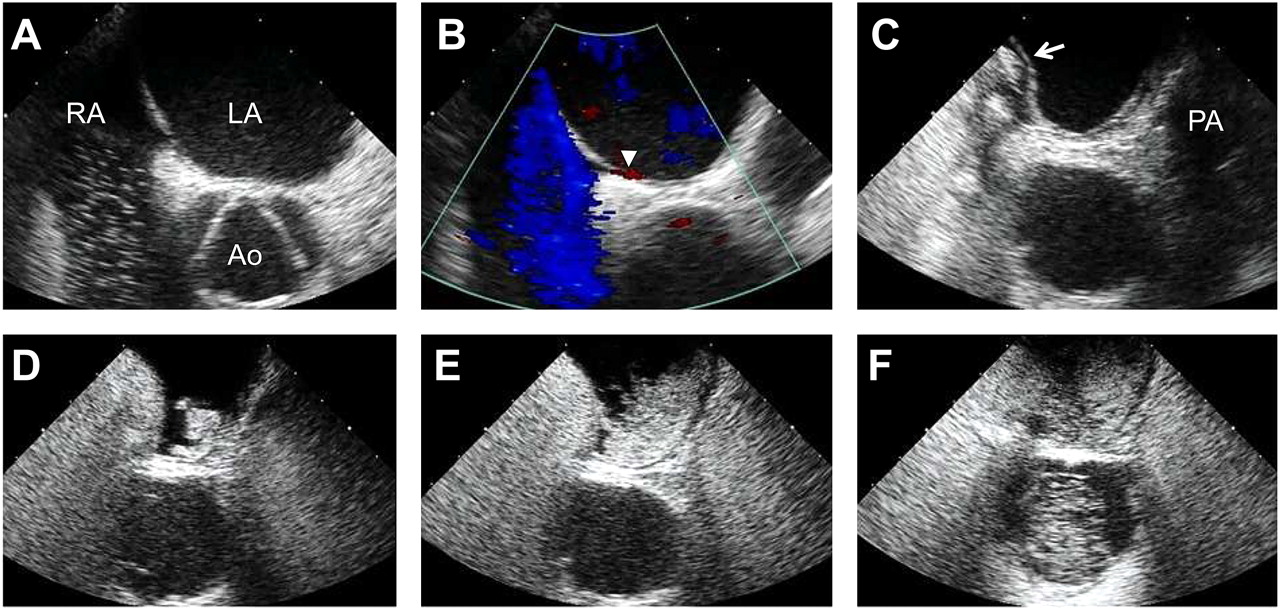
Transoesophageal contrast echocardiography (TOE) in a diver for the detection of patent foramen ovale (PFO; frame rate for echo images=62 Hz, for colour Doppler image=20 Hz). (A) TOE short-axis view showing the left atrium (LA) and the aortic root (Ao) free of ultrasound contrast medium; there are a few contrast bubbles in the right atrium (RA). The image is taken close to the end of the Valsalva strain phase with the interatrial septum bulged towards the RA. (B) Identical TOE image plane as in all other panels showing a red colour Doppler signal at the site of the foramen ovale (white arrowhead)—that is, a left-to-right shunt across a PFO. (C) Image taken immediately after release of the Valsalva strain phase with the interatrial septum (fossa ovalis region) now bulging towards the LA (white arrow), thus indicating a pressure rise in the RA above that in the LA. PA, pulmonary artery. (D) Short-axis view image obtained instantaneously after that in (C) showing a shunt of contrast medium across a PFO from the right to the left atrium. (E) The shunt is even more pronounced on this next image (PFO grade 3). (F) The aortic root is now also filled with contrast medium, which crossed the PFO a few images earlier.
It was suggested in 1986 that a cardiac right-to-left shunt may be important for paradoxical gas embolism in scuba divers.4 Subsequently, the importance of PFO for decompression events in divers has been further investigated.5–9 The most serious symptoms and signs related to decompression are major—that is, neurological decompression illness (DCI) events and the development of ischaemic brain lesions (figure 2). The risk of having a major DCI event is low and has been reported to be 2.5/104 dives, but it is five times higher in divers with a PFO than in those without a PFO.10 11 The average number of ischaemic brain lesions as observed by MRI in experienced divers with a PFO has been reported to be twice as high as in divers without a PFO.12
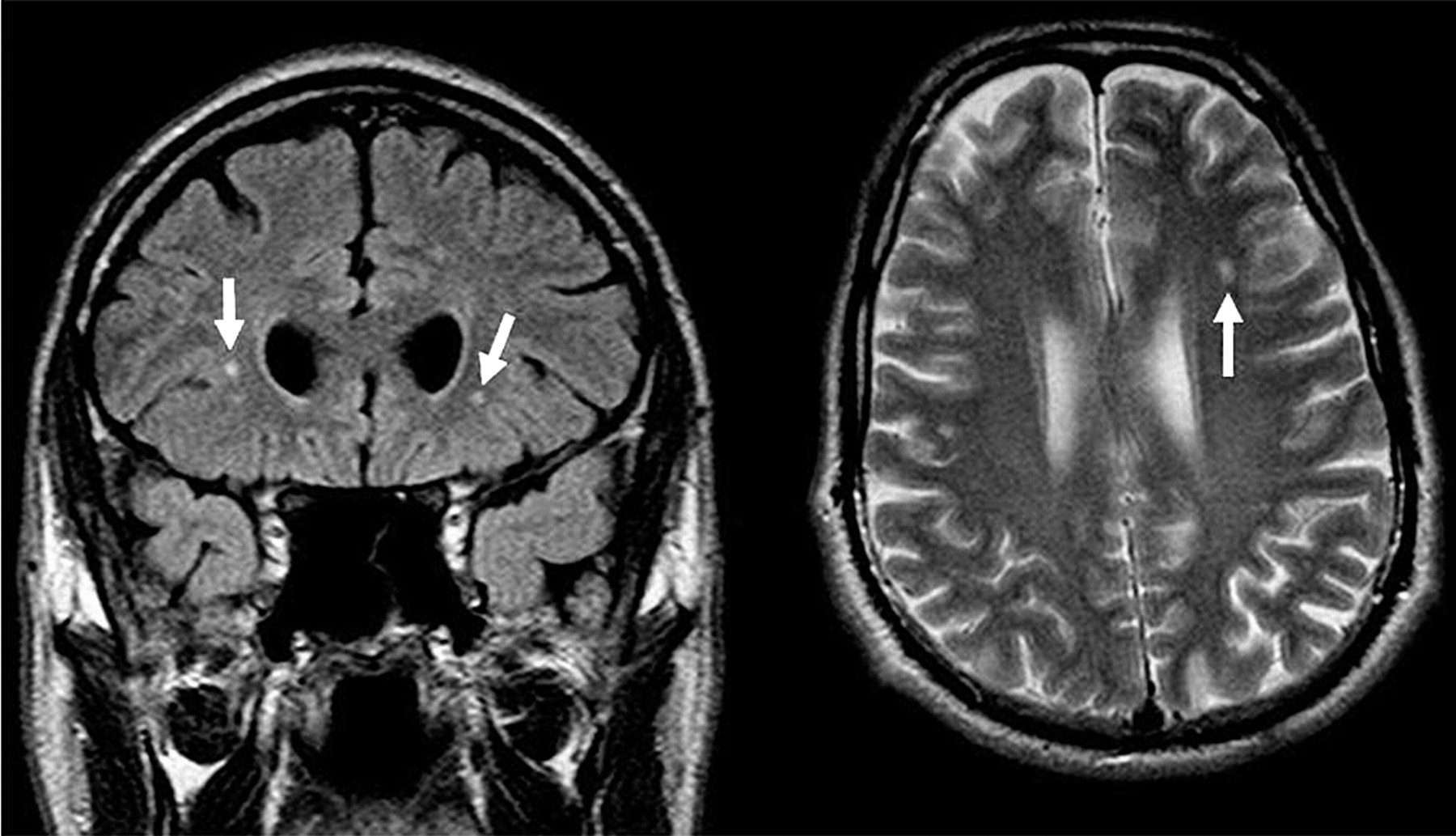
T2-weighted cerebral magnetic resonance images in the frontal (left) and transversal (right) plane showing three ischaemic brain lesions (arrows).
So far, no investigation has been carried out of the effect of PFO closure in divers on the occurrence of symptomatic and asymptomatic neurological events. Our study tested the hypotheses that percutaneous PFO closure reduces major DCI events, and slows down the development of ischaemic brain lesions.
Methods
Study subjects and study design
The participants of this study were recruited from those included in a previous investigation at our institution focusing on the incidence of DCI in divers.11 For inclusion in that study, ≥200 dives and adherence to decompression tables was required, thus, unexpected DCI were reported. Among those 230 scuba divers, 104 agreed to participate in this, prospective long-term study. At the baseline examination, all study subjects underwent contrast transoesophageal echocardiography (TOE; see below) for the diagnosis of absent or present PFO (figure 1). Thirty-nine divers had no PFO (called ‘no PFO’ group) and 65 divers had a PFO. None of the divers with a PFO had agreed to take part in a study designed to randomly allocate them to percutaneous PFO closure or no PFO closure, even when a subsequent PFO closure after study termination was offered to the latter. Twenty-six divers with a PFO chose to undergo PFO closure (called ‘PFO closure’ group), 39 divers selected to have no PFO closure (called ‘ no PFO closure’ group).
Examinations were carried out at baseline and at three follow-up examinations at 1, 3 and 5 years. At each of the four examinations, the study individuals answered a detailed questionnaire about their health and about their diving habits and accidents. Subsequently, the divers underwent a TOE at baseline and a cerebral MRI at baseline and at all follow-up examinations. The doctors performing the different study examinations were unaware of the results of the two primary study end points on the other occasions: major DCI events and number of ischaemic brain lesions by MRI.
The more general term DCI is used instead of decompression sickness and arterial gas embolism (the two subunits of DCI), which, based on self-reported temporal information about diving-related events, are clinically difficult to distinguish.
The study was approved by the ethics committee of the Kanton of Bern, Switzerland and the study subjects gave written informed consent to participate in the study.
Health status, diving habits and accidents
Before examining the study subjects by TOE and/or MRI, their past medical history, including alcohol use, smoking habits and medication was assessed. Special attention was given to a history of diabetes mellitus, systemic hypertension, cardiac disease, respiratory disease, migraine or chronic headache, other neurological disorders, rheumatic illness, previous surgical operations and/or accidents other than diving accidents. At baseline and during each of the follow-up examinations, a detailed diving history was obtained, including duration of engagement in diving, total number of dives, mean diving depth, number of dives >40 m, breathing gas used (compressed air or higher-than-normal partial pressure of oxygen plus nitrogen or helium). Subjects were asked about the presence or absence of DCI and, if it had been present, questions were asked about the signs and symptoms of DCI. A DCI event was classified as minor or major.13 14 Minor DCI events were scored (0–3) according to the frequency of their occurrence (never, rarely, every fourth to third dive, every second dive or more often). Minor DCI symptoms included bends, cutaneous erythema, extreme fatigue, headache, dizziness, paraesthesias and tinnitus. Major DCI events were defined by one or more of the following symptoms: limb weakness, cutaneous sensory level, impaired bladder or bowel control, paresis or paraplegia, blurred vision, dysarthria, amnesia for the event, hemiplegia or loss of consciousness after a dive. The time frame of occurrence and disappearance of DCI symptoms and eventual treatment in a recompression chamber was also registered.
Contrast transoesophageal echocardiography
Before intubation of the TOE probe, the epipharynx was anaesthetised using lidocaine hydrochloride 10% spray. A three-lead ECG and blood pressure were registered during TOE. No sedative drugs were used in any of the study subjects. TOE was performed in the left lateral supine position of the study subject using a Siemens Acuson Sequoia C256 (Mountain View, California, USA) Doppler echocardiography system with a multiplane, 3.5–7 MHz probe. Examination for the presence or absence of PFO occurred in the transversal, short-axis (30°; figure 1) and longitudinal (90°) image plane. A left-to-right atrial shunt via a PFO was screened for by colour Doppler imaging (figure 1B). The echo contrast medium for the detection of a right-to-left atrial shunt consisted of an ad hoc sonicated mixture of 0.5 ml of air and 4.5 ml of a gelatine-containing plasma expander (Physiogel). Echo contrast tests were performed in the two image planes mentioned above by injection of 5 ml of contrast into the right antecubital vein. Using a Valsalva manoeuvre (strain phase starting simultaneously with the contrast bolus injection), a left-ward deviation of the interatrial septum in the fossa ovalis region (figure 1C) was observed immediately after release of the Valsalva strain phase (lasting 5–10 s); this was seen in all individuals and was taken as a sign of a successful Valsalva manoeuvre (short right atrial preload increase and pressure rise).15 Diagnosis of PFO required the crossing of bubbles from the right to the left atrium (figure 1D–F) within four heart beats after release of the Valsalva strain phase. The degree of PFO was qualitatively characterised by a score of 0–3, with a score of 1 representing the cross-over of a few single bubbles and a score of 3 representing the shunt of an entire cloud of bubbles (figure 1D–F); score 2 between 1 and 3.
Cerebral MRI
MRI was performed using a 1.5 T Magnetom Vision system (Siemens, Erlangen, Germany) equipped with a head coil. The imaging protocol included T1-weighted, T2-weighted and proton density-weighted imaging. Images were reviewed independently by two neuroradiologists blinded to the study group, to whether a PFO was present and to treatment of the PFO. A lesion was counted if it was hyperintense on proton density-weighted and T2-weighted images (figure 2).
Statistical analysis
The sample size of the study was estimated on the basis of a previous study examining the occurrence of ischaemic brain lesions by MRI in divers.12 Accordingly, sample size calculated before the study was based on the following assumptions: ability to detect a difference of 1.5 ischaemic lesions (1.5 vs 3.5 lesions per diver) at long-term follow-up between the PFO closure group and the PFO no closure group; SD of ischaemic lesions =4.0, α error level =5%, power =80%. Accordingly, a total sample size of 49 patients for the two PFO groups with unpaired measurements was required. All continuous data are given as mean ± SD. The distribution of the data for normality was tested by the Kolmogorov–Smirnov test. Characteristics between the groups at baseline and at long-term follow-up examination were analysed by factorial analysis of variance (ANOVA) test for continuous data and by χ2/ Fisher's exact tests for categorical data. The post hoc test for the factorial ANOVA statistics was performed by the Scheffé test. Analysis of longitudinal data from baseline to long-term follow-up was carried out by repeated-measures ANOVA. A multivariate analysis was performed using multiple linear regression analysis with the two primary end points as the dependent variables (sum of major DCI events from the first to the third follow-up examination; total number of ischaemic brain lesions at the third follow-up examination) and significant variables of the univariate analysis (at a p value <0.10) as the independent variables. Data were analysed using StatView 4.57 statistical software (Abacus Concepts Inc, Berkley, California, USA).
Results
Baseline: study subjects characteristics, health status and diving habits
Of the 104 study individuals (n=6 professional divers), 39 (38%) had no PFO, 26 belonged to the PFO closure group (24%) and 39 to the PFO no closure group (38%; table 1). The three groups did not differ in age, gender and medical history (table 1), except for a trend towards more frequent cardiac disease (coronary artery disease) in the PFO closure group versus the other groups. The weight of the divers in the three groups was 71±11 kg, 72±14 kg, 71±10 kg, respectively (p=0.82).
Baseline: study subject characteristics
In the PFO closure group, PFO was occluded using the Amplatzer PFO closure device 25 mm.
The PFO degree was higher in the PFO closure group than in the PFO no closure group (table 2). The years of diving experience, cumulative number of dives, average diving depth and the cumulative number of deep dives did not differ among the groups (table 2). There was a trend towards a higher number of annual dives in the PFO closure group than in the other groups. The frequency of use of compressed air as breathing gas as opposed to so called nitrox gas with higher-than-normal oxygen partial pressure (used during deep dives >30 m), was similar among the groups.
Baseline: PFO degree, diving habits, decompression symptoms, ischaemic brain lesions
Baseline: DCI events and their treatment
At baseline, the minor DCI score was similar between the study groups (table 2). The number of major DCI events and major DCI per 104 dives was highest in the two PFO groups (6/104 dives), but did not differ statistically in comparison with the no PFO group. However, the number of DCI events lasting longer than 24 h and requiring treatment in the recompression chamber was higher in the PFO closure group than in the other groups (table 2).
The absolute number of ischaemic brain lesions was highest in the PFO no closure group without being statistically different from the other groups (table 2). There was a trend towards more ischaemic brain lesions per 104 dives in the PFO no closure group.
Follow-up: diving habits, DCI events and ischaemic brain lesions
The total number of dives from before baseline to long-term follow-up in all study participants amounted to 81 654; 18 394 (23%) dives took place during the follow-up period.
The number of individuals lost to long-term follow-up was higher in the no PFO group than in the other groups (table 3). In the PFO closure group, one individual had a residual shunt 6 months after device implantation. Long-term follow-up duration was 5.5 years in the no PFO group, which was significantly longer than in the PFO groups. There was no difference between the groups in the number of dives per year, in the average diving depth and in the number of deep dives. There was a trend towards a higher number of cumulative dives during the entire follow-up in the PFO closure group as compared with the other groups (table 3). The use of compressed air as breathing gas was significantly higher in the no PFO than in the PFO groups.
Long-term follow-up: diving habits, decompression symptoms, ischaemic brain lesions
At long-term follow-up examination, the minor DCI score was similar between the study groups (table 3). The absolute number of major DCI events as experienced during the entire follow-up (total of five events) was 0 in the no PFO group, it was 0.04±0.21 (per person) in the PFO closure group (1 event) and it was 0.18±0.40 in the PFO no closure group (four events; p=0.056; figure 3). The number of major DCI events per 104 dives was significantly higher in the PFO no closure group than in the other groups (table 3; figure 3). There was no difference between the groups in the number of prolonged DCI events and none of the divers had to be treated in the decompression chamber during follow-up.

Symptomatic neurological events. Mean number of cumulative major decompression illness (DCI) events at long-term follow-up examination (vertical axes) in absolute numbers (left panel) and as a rate per 104 dives (right panel) for the different study groups (horizontal axis). PFO, patent foramen ovale.
The absolute number of ischaemic brain lesions at long-term follow-up was highest in the PFO no closure group (table 3; figure 4). The number of ischaemic brain lesions per 104 dives was significantly higher in the PFO no closure group than in the other groups (table 3; figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Asymptomatic neurological events. Mean number of ischaemic brain lesions as detected by MRI at long-term follow-up examination (vertical axes) in absolute numbers (left panel) and as a rate per 104 dives (right panel) for the different study groups (horizontal axis). PFO, patent foramen ovale.
By multivariate analysis, the following were significant predictors for the cumulative number of major DCI events during long-term follow-up (ie, events at baseline not counted; p=0.034 for the entire model): group PFO no closure (p=0.017), number of all dives during follow-up (p=0.031); non-significant determinants were age, PFO grade, number of ischaemic brain lesions at baseline, long-term follow-up duration, frequency of compressed air as breathing gas at long-term follow-up. The following were determinants for the number of ischaemic brain lesions found at long-term follow-up MRI (p=0.006 for the entire model): group PFO no closure (p=0.023), age (p=0.003); non-significant determinants were number of ischaemic brain lesions at baseline, number of all dives, PFO grade and long-term follow-up duration, frequency of compressed air as breathing gas at long-term follow-up.
Discussion
This first study of the efficacy of PFO closure in continuing divers found a trend towards fewer major DCI events and significantly fewer ischaemic brain lesions at 5.5 years after the procedure in comparison with divers without a PFO or those with a PFO but no closure.
Incidence of major DCI and ischaemic brain lesions in divers
The total number of dives performed by our study individuals during their entire ‘career’ was 81 654. There were 24 major DCI events during the baseline and follow-up period. Thus, the rate of major DCI per 10 000 dives was 2.9—that is, 1.1/104 dives in divers without a PFO and 5.6/104 and 6.1/104, respectively, in the PFO closure and PFO no closure groups. These numbers are consistent with those reported previously by our group,11 which is not surprising, because this study population was recruited entirely from the 230 divers from the previous investigation. Focusing on the 5.3-year follow-up period, five major DCI events occurred during 18 394 dives in all groups yielding a rate of 2.7/104 dives and thus, confirming the correctness of the initially described 1.9–2.5/104.10 11 16 Four of the major DCI events in this study occurred in the PFO no closure group and one event in the PFO group undergoing percutaneous closure, resulting in a substantial variability in the DCI rate of 0, 0.5 and 36/104 dives (see figure 3). In commercial divers, irrespective of the presence of a PFO, a similar rate of 35/104 dives has been reported,17 which rather than a confirmation of the result for our PFO no closure group is a reflection of the very low prevalence of major DCI, with large variability of the data. Accordingly, the difference between the two PFO groups at long-term follow-up just reached statistical significance.
Although these rates of major DCI were similar to those reported in the literature, the occurrence of PFO in divers was much higher: 65% in this study versus 25–27% in previous studies.12 In an unselected population of divers, the PFO rate ought to reflect that of the general population, which is 27% without accounting for the age of the individuals.3 The doubled frequency of PFO in our study population is explained by the self-selection process for study participation, which, obviously, tended to prefer divers with a PFO and those who had experienced a major neurological DCI event in the past. As the goal of this study was to investigate the efficacy of PFO closure on major DCI and ischaemic brain lesions, it was not necessary for the frequency of PFO to reflect that in the general population.
At long-term follow-up MRI examination, a total of 150 ischaemic brain lesions were counted in 83 divers (on average 1.8 lesions per diver), which is similar to the 41 lesions in 52 divers (0.8 lesions per diver) reported by a previous study from our laboratory in a different population of divers.12 The divers with a PFO had a slightly higher count of ischaemic lesions than in the previous study (approximately 2 vs 1.2 per diver) which cannot be explained by the above-mentioned self-selection process that preferred symptomatic individuals, because no statistical relation could be found between major DCI and number of ischaemic brain lesions—that is, numerous divers had had asymptomatic cerebral ischaemic events. Also, the study participants did not know whether they had absent or present brain lesions before inclusion. Asymptomatic neurological events in divers is an important subject, because they are likely to occur in a quarter to a half of high volume divers such as ours (on average more than 1000 dives),18 and because they represent potential neurological long-term hazards.19
PFO closure in divers
For both symptomatic and asymptomatic neurological events related to diving, two primary study end points (major DCI and ischaemic brain lesions) were selected for efficacy testing of PFO closure. Initially, our study was designed to randomly allocate the divers with a PFO to percutaneous closure or conservative treatment. None of the individuals with a PFO agreed to participate in a randomised study, but spontaneously selected the treatment arm. This determination concurs with the primary agreement to participate in the study, but is its major shortcoming. However, and to the best of our knowledge, no previous studies have investigated the effect of PFO closure on neurological events in divers. Nevertheless, closure of a PFO with a significant shunt is broadly advocated if the person wishes to continue diving,20 though there is no single piece of evidence favouring the efficacy of closure. The only case reports available on the subject have suggested that PFO closure in divers is more21–23 or less feasible.24 Considering the technical ease of the procedure in the general patient population with device implantation failure in 0.2% and procedural complications in approximately 2% (device embolisation in 0.6%),25 feasibility of PFO closure in divers is not unexpected. In the study by Wahl et al,25 12% of patients had a residual shunt 6 months after PFO closure as compared with 1/26 (4%) divers in this investigation. Interestingly, it was this diver who experienced the one major DCI event occurring in the PFO closure group.
Confounding variables
Naturally, residual shunt after PFO closure is a confounding variable, negatively influencing the primary neurological end points of this study. Since the statistical analysis was based on the intention-to-treat principle, this confounder is—by definition—irrelevant. A further determining factor for neurological events is the degree of bubble load to which the diver puts herself/himself at risk during ascent and shortly after surfacing. Apart from computerised decompression algorithms to which all the divers reportedly adhered, the type of breathing gas used may influence the appearance of bubbles in the systemic circulation. During the follow-up period decompression during the dives was performed more cautiously. This is indicated by the decreasing number of all dives and of deep dives per year and by the lower use of compressed air as breathing gas (see tables 2 and 3). The changes in breathing gas use occurred predominantly in divers with a PFO, but hardly at all in those without. Methodologically, the more cautious behaviour of the divers at higher risk for neurological events represents a conservative action, which heightens the value of the main study results—that is, prevention of neurological events in the PFO closure group. Other potentially confounding variables were entered into the multivariate regression model (apart from the study group) on the basis of their statistical trend of association with the primary end points—namely, age of the diver, number of dives, PFO grade, follow-up duration. The only predictive variable for both symptomatic and asymptomatic neurological events was the group of divers with a PFO but no closure. In addition, the total number of dives played a part in the occurrence of major DCI, and the age of the diver in the number of ischaemic brain lesions found by MRI.
Study limitations and clinical implications
The most important limitation of this study, its non-randomised design, implies that—despite indications of efficacy—PFO closure in divers should not be generally adopted. Divers with a PFO and a history of neurological events should be prompted to stop diving. If unwilling to do so, they should be motivated to take part in a larger, probably multicentre, randomised trial, which extends the present proof of concept investigation.
A further limitation—considering the relatively limited number of divers originally included—is the loss of study individuals to long-term follow-up, which amounted to one-third in the PFO no closure group. Theoretically, divers with DCI in this group might have been more likely to undergo follow-up examination than those without neurological events.
The results of this study do not apply to occasional recreational divers and they have no relevance for stroke prevention in non-diving patients. In the latter context, our study does not provide new evidence supporting efficacy of PFO closure in the prevention of recurrent stroke or in the treatment of migraine.
References
Footnotes
MB and RZ contributed equally to this work.
Competing interests None.
Ethics approval From the ethics committee of the Kanton of Berne, Switzerland.
Provenance and peer review Not commissioned; externally peer reviewed.