Article Text

Abstract
Objective: To assess actual practices and in-hospital outcome of patients with acute myocardial infarction on a nationwide scale.
Methods: Of 443 intensive care units in France, 369 (83%) prospectively collected data on all cases of infarction (within < 48 hours of symptom onset) in November 2000.
Results: 2320 patients (median age 68 years, 73% men) were included, of whom 83% had ST segment elevation infarction (STEMI). Patients without STEMI were older and had a more frequent history of cardiovascular disease. Median time to admission was 5.0 hours for patients with and 6.5 hours for those without STEMI. Reperfusion therapy was used for 53% of patients with STEMI (thrombolysis 28%, primary angioplasty 25%). In-hospital mortality was 8.7% (5.5% of patients without and 9.3% of those with STEMI). Multivariate analysis found that age, Killip class, lower blood pressure, higher heart rate on admission, anterior location of infarct, STEMI, diabetes mellitus, previous stroke, and no current smoking independently predicted in-hospital mortality. At hospital discharge, 95% received antiplatelet agents, 75% received β blockers, and over 60% received statins. Angiotensin converting enzyme inhibitors were prescribed for 40% of the patients without and 52% of those with ST elevation.
Conclusions: This nationwide registry, including all types of centres irrespective of their size and experience, shows continued improvement in patient care and outcomes. Time from symptom onset to admission, however, has not improved in recent years and reperfusion therapy is used for just over 50% of patients with STEMI, with an increasing use of primary angioplasty.
- 4S, Scandinavian simvastatin survival study
- ACE, angiotensin converting enzyme
- CARE, cholesterol and recurrent events
- CONSENSUS, cooperative new Scandinavian enalapril survival study
- ESSENCE, efficacy and safety of subcutaneous enoxaparin in unstable angina and non-Q wave myocardial infarction
- GISSI, Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico
- ISIS-4, fourth international study of infarct survival
- LIPID, long-term intervention with pravastatin in ischaemic disease
- LVEF, left ventricular ejection fraction
- MITI, myocardial infarction triage and intervention
- MONICA, monitoring trends and determinants in cardiovascular disease
- NSTEMI, non-ST segment elevation myocardial infarction
- PCI, percutaneous coronary intervention
- STEMI, ST segment elevation myocardial infarction
- TIMI, thrombolysis in myocardial infarction
- myocardial infarction
- intensive care units
- in-hospital outcome
Statistics from Altmetric.com
- 4S, Scandinavian simvastatin survival study
- ACE, angiotensin converting enzyme
- CARE, cholesterol and recurrent events
- CONSENSUS, cooperative new Scandinavian enalapril survival study
- ESSENCE, efficacy and safety of subcutaneous enoxaparin in unstable angina and non-Q wave myocardial infarction
- GISSI, Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico
- ISIS-4, fourth international study of infarct survival
- LIPID, long-term intervention with pravastatin in ischaemic disease
- LVEF, left ventricular ejection fraction
- MITI, myocardial infarction triage and intervention
- MONICA, monitoring trends and determinants in cardiovascular disease
- NSTEMI, non-ST segment elevation myocardial infarction
- PCI, percutaneous coronary intervention
- STEMI, ST segment elevation myocardial infarction
- TIMI, thrombolysis in myocardial infarction
The 1990s have provided a large amount of information on the optimal management of patients with acute myocardial infarction, both in terms of acute reperfusion therapy and of secondary prevention. Guidelines have been published that specify the optimal treatment strategies for such patients.1,2 Few data, however, are available regarding the way these guidelines translate into real life clinical practice. Several important registries have provided useful information but they usually included only specially motivated centres3 or selected populations,4 and their conclusions therefore may not reflect what truly happens on a wider scale in the real world. The USIC (Unité de Soins Intensifs Coronaires) 2000 survey is a prospective registry of all patients admitted to intensive care units in France for acute myocardial infarction by the end of 2000. The purpose of the present study is to describe the baseline clinical profile of the patients, their initial management and in-hospital outcome, and the medications prescribed at discharge.
METHODS
Population
The objective of the USIC 2000 study was to gather complete and representative data on the management and outcome of patients admitted to intensive care units for acute myocardial infarction over a one month period in France, irrespective of the type of institution to which the patients were admitted (that is, university hospitals, public hospitals, or private clinics). To this purpose, a list of all intensive care units or coronary care units admitting patients at the acute stage of myocardial infarction was established at the beginning of 2000. All physicians in charge of these units were then asked to participate in the study. In all, 443 centres were listed: 49 university hospitals, 271 public hospitals, and 123 private clinics. Of these, 369 finally participated in the study (83%). The participation rate was 90% (n = 44) for university hospitals, 84% (n = 228) for public hospitals, and 79% (n = 97) for private clinics. One physician responsible for the study was recruited in each centre and filled in a case record form for each patient meeting the inclusion criteria and admitted to the intensive care unit during the study recruitment period. The physicians in charge of the patients took care of them according to their usual practice and independently of the study.
Patient selection
All consecutive patients admitted to the participating centres from 1 November through 30 November 2000 were included in the study if they met the following criteria:
-
Diagnosis of acute myocardial infarction based on the presence of an increase of serum markers higher than twice the upper limit of normal for creatine kinase, creatine kinase MB fraction, or troponins; and either chest pain lasting for at least 30 minutes and not relieved by nitrates or ECG changes on at least two contiguous leads with pathological Q waves (at least 0.04 seconds), or persisting ST elevation or depression > 0.1 mV.
-
Time from the beginning of symptoms to admission to the intensive care unit of less than 48 hours.
Patients gave informed consent for participation in the survey and late follow up.
Data collection
The patients’ cardiovascular history, their current medications at the time of admission, their risk factors (smoking status, history of hypertension or treated hypertension, cholesterol concentration > 6.5 mmol/l or treated hyperlipidaemia, family history, diabetes mellitus defined by treatment with insulin or oral antidiabetic medications, or previously documented fasting hyperglycaemia (> 6.99 mmol/l), their in-hospital clinical course including maximum Killip class, and the initial diagnostic and treatment management were recorded for each patient. Furthermore, left ventricular ejection fraction (LVEF), when assessed at any time during the first five days, was recorded. The value of LVEF that was used for the present analyses was determined by the following priority ranking of the method used: firstly, left ventricular contrast angiography; secondly, radionuclide angiography; thirdly, echocardiography based on Simpson’s method, fourthly, echocardiography based on the Berning wall motion index5; and lastly, echocardiography with visual estimation of LVEF.
Statistical analysis
All continuous variables, except time to admission, are reported as mean (SD). All categorical variables are described in absolute and relative frequency distributions. Groups were compared by unpaired t tests for continuous variables and χ2 tests for discrete variables. Time to admission is expressed as median time with 25th and 75th centiles; the Mann-Whitney test was used for comparisons. Multivariate stepwise logistic regression analysis was used to assess the independent prognostic value of baseline parameters on in-hospital outcome. Variables with p < 0.10 on univariate analyses were used in the models. For all tests a p < 0.05 was considered significant.
RESULTS
Baseline parameters
Of the 2580 patients initially considered, 260 had to be rejected because they did not meet the entry criteria (mainly for admission beyond the initial time frame of the study and unconfirmed acute myocardial infarction), so that 2320 patients were included. Median age of the population was 68 years (range 22–101 years), and 27% of the patients were women. Non-ST segment elevation myocardial infarction (NSTEMI) was present in 17% of the patients and 83% had ST segment elevation infarction (STEMI) defined as either Q wave, ST segment elevation, or left bundle branch block on their initial ECG. Table 1 details the initial characteristics according to the type of infarction. Patients with NSTEMI were older, more often hypertensive, and had a more frequent history of cardiovascular disease. Killip class on admission, however, was not different for patients with or without STEMI.
Baseline parameters of patients admitted for STEMI or NSTEMI
Initial management
Median time from symptom onset to hospital admission was longer for patients with NSTEMI; in addition, for patients with STEMI, time to admission was strongly linked to the service that was called first: median time to admission was 4.0 (2.5, 8.3) hours for patients who called the mobile intensive care unit, 6.96 (3.25, 18.0) hours for patients who called their general practitioner first, and 10.7 (4.19, 24.0) hours for those who called their cardiologist first. Pre-hospital intravenous thrombolysis and hospital thrombolysis were given to 9% (n = 180) and 19% (n = 365) of the patients with STEMI or left bundle branch block, respectively. In addition, 484 patients (25%) with STEMI had primary percutaneous coronary intervention (PCI) defined as PCI within 24 hours of admission without intravenous thrombolysis. Both intravenous thrombolysis and primary PCI were strongly related to the age of the patients and to the time from symptom onset. Among patients with STEMI over 70 years of age, 20% received thrombolysis and 18% received primary PCI compared with 34% and 30%, respectively, of younger patients. Likewise, among patients admitted within six hours of symptom onset 39% were given thrombolysis and 34% underwent primary PCI compared with 16% for each method among patients admitted beyond this time frame.
Table 2 lists the medications given at any time during the first 48 hours. Low molecular weight heparin and nitrates were given more often to patients with NSTEMI and glycoprotein IIb/IIIa inhibitors were used less often. There were no differences regarding β blocking agents and statins.
Medications given during the first 48 hours after hospital admission according to type of infarction
In-hospital outcomes
LVEF was evaluated during the first five days in 2066 patients, most often by echocardiography. Overall, 54% of the patients had an ejection fraction > 50% and 13% had an ejection fraction ⩽ 35%; ejection fraction was less altered in patients with NSTEMI (table 3).
Left ventricular ejection fraction measured during the first five days
Table 4 lists in-hospital complications. There were essentially no differences between the two groups regarding most complications. Five day mortality was 6.1% (141 patients) and was lower for patients with NSTEMI (3.8%) than for those with STEMI or left bundle branch block (6.6%). Likewise, in-hospital mortality (8.7%) was lower for patients with NSTEMI (5.5% v 9.3%, p = 0.015).
In-hospital complications
Table 5 lists the predictors of early mortality by univariate analysis. Multivariate regression analysis (table 6), however, showed that only nine variables were independent predictors of five day mortality: older age, higher Killip class on admission, and lower systolic arterial pressure were the three most important predictors of increased mortality (fig 1); anterior location of infarction, higher heart rate, type of infarction (with or without ST segment elevation), and previous stroke also increased the early risk of death. Current smoking and history of hyperlipidaemia were associated with a lower risk. The same variables predicted in-hospital mortality, with the addition of presence of diabetes mellitus.
Univariate predictors of five day mortality in the whole population
Multivariate predictors of five day mortality and in-hospital mortality
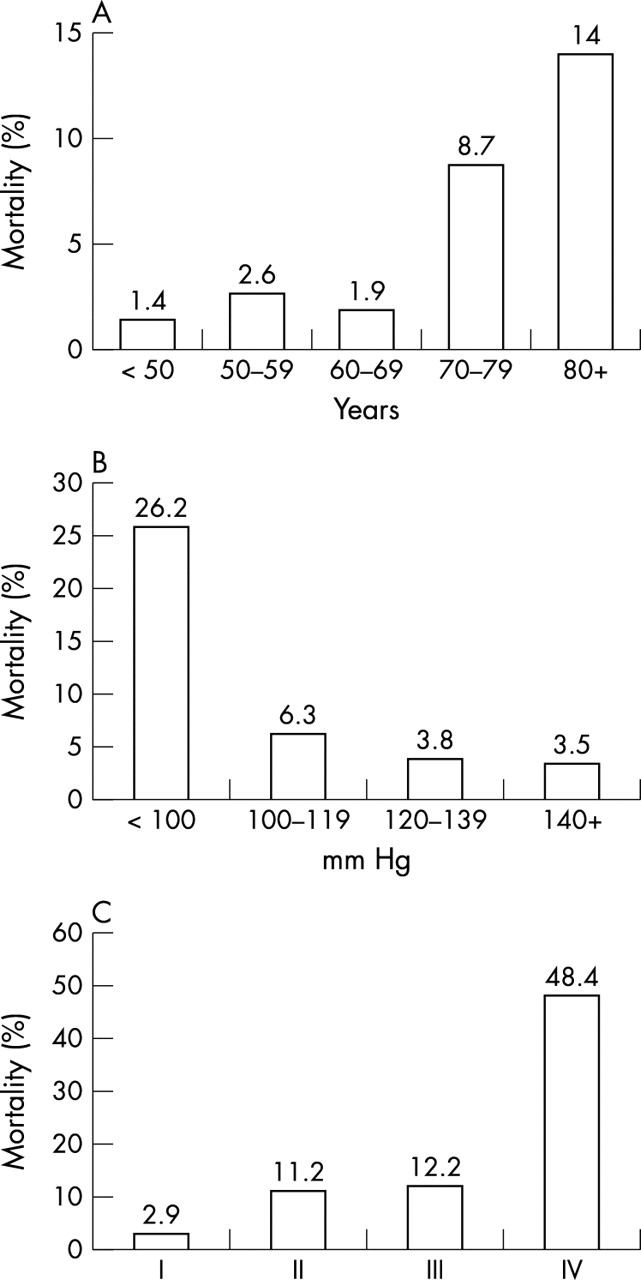
In-hospital mortality according to (A) age, (B) systolic arterial pressure measured at hospital admission, and (C) Killip class.
Medications at hospital discharge
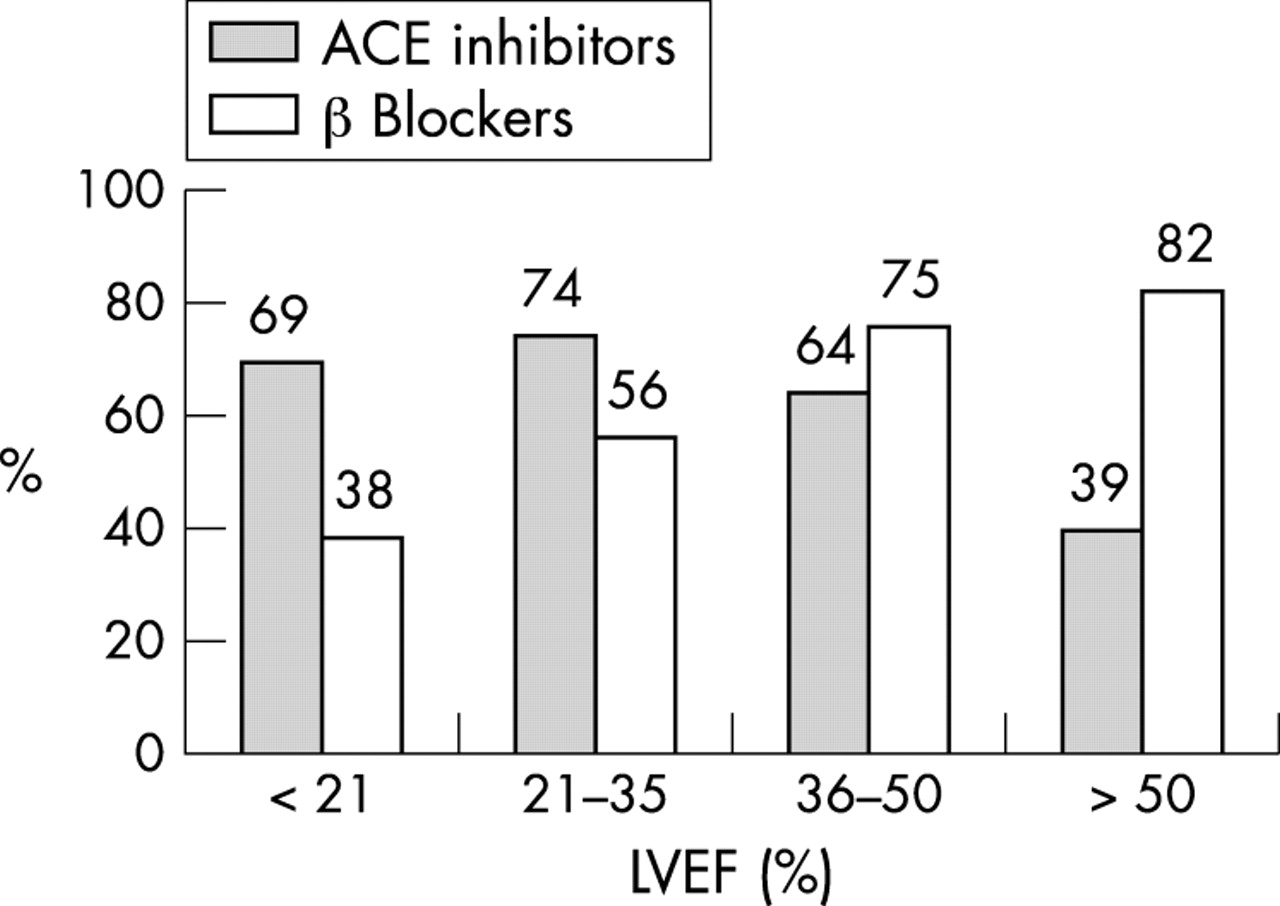
Table 7 lists medications at hospital discharge recorded for the 2119 hospital survivors. About 95% received antiplatelet agents, 75% were taking β blockers, and over 60% received statins. Angiotensin converting enzyme (ACE) inhibitors were prescribed for 40% of the patients with NSTEMI and 52% of those with STEMI. ACE inhibitor prescription was strongly linked to the level of LVEF: 39% for patients with LVEF > 50% and more than 74% for patients with LVEF ⩽ 35%. The reverse trend was observed for β blocking agents (fig 2).
Medications at hospital discharge

{kind=link}
{kind=link}
Prescription of β blockers and angiotensin converting enzyme (ACE) inhibitors at hospital discharge according to left ventricular ejection fraction.
DISCUSSION
Representativeness of the study population
The present study analysed the current management of myocardial infarction in the intensive care unit on the scale of a whole country, irrespective of the type of institution to which the patients were admitted. Participation was high at all types of institutions (academic, general hospitals, private clinics) and no imbalance was seen from one region to another. It may therefore be considered highly representative of the practice in France by the end of 2000. As the new definition of acute myocardial infarction6 was made public at the time of the survey, it is most probable that many patients with NSTEMI were not included in the registry, as they were considered to have unstable angina rather than infarction. In addition, only a minority of French centres systematically measured troponin concentrations of patients with suspected acute coronary syndromes at that time. Lastly, only patients admitted to intensive care units were included in the survey. In France, virtually all patients with STEMI are admitted to intensive care units; in contrast, it is not unusual that patients with non-ST elevation acute coronary syndromes are admitted to general wards. All of these factors probably explain why patients with NSTEMI were only a minority of the patient population in the present registry. Our conclusions therefore apply mainly to patients with STEMI.
Characteristics of the population
Compared with previous surveys carried out in France over the past 10 years, the proportion of diabetic patients admitted for acute myocardial infarction was higher in 2000 (21%) than in 1995 (17%) and similar to the findings of a survey carried out in 1998 of patients with acute coronary syndromes (21%).7–9 Patients were slightly younger than those enrolled in a similar survey carried out in 19957; this finding is in keeping with data from the MONICA (monitoring trends and determinants in cardiovascular disease) programme in France, which also found that patients with acute myocardial infarction in recent years tended to be younger.10
Initial management
Time from symptom onset to hospital admission remained particularly long; for patients with STEMI, the median time to admission was five hours and no progress was observed in this regard compared with the French 1995 survey.7 Several mechanisms may explain this excessive time delay. One important factor may be the tendency of patients to deny the cardiac origin of chest pain, and this factor is probably one of the most difficult to correct.11,12 However, the present study also shows that, once a patient has decided to call a doctor, the first person to be contacted is decisive in the time delay before hospital admission; median times before hospital admission were four hours when emergency medical services were called, compared with nearly seven hours when the general practitioner was called and 11 hours when the cardiologist was called. Continued efforts should be made to encourage patients to contact emergency medical services when they have prolonged chest pain. Recent experiments have shown that a media campaign directed at the public can improve this situation.13,14
Reperfusion therapy was given to only 53% of patients with STEMI, Q waves, or left bundle branch block; this rather low figure is explained mainly by the time delay from symptom onset to hospital admission, but also by a much lower use of reperfusion therapy for older patients, despite the evidence that reperfusion therapy, including thrombolysis, is beneficial for these patients as well.15,16 Similar rates of reperfusion therapy have been reported in other registries reflecting real world practice in various countries.17–19 Intravenous thrombolysis remained the most widely used method of reperfusion and nearly one patient in 10 received thrombolysis before hospital admission (that is, in the mobile intensive care unit). Among patients receiving reperfusion therapy, the proportion of patients treated with primary PCI (47%), however, was higher than previously observed, either in France or in several other countries.7,18–20
A substantial proportion of the patients were treated with low molecular weight heparin, particularly in the case of NSTEMI (40%), which reflects the impact of the results of the TIMI (thrombolysis in myocardial infarction) 11B and ESSENCE (efficacy and safety of subcutaneous enoxaparin in unstable angina and non-Q wave myocardial infarction) trials on everyday practice.21,22 Fewer than 20% of the patients were treated with glycoprotein IIb/IIIa inhibitors, mainly patients who underwent early angiography and PCI. β Blocking agents were given to over 70% of the patients and 45% of patients received statins within two days of hospital admission. This finding may be explained in that statin administered early during acute coronary syndromes has no deleterious effect and that patients who do not receive secondary prevention medications during the initial hospital stay are less likely to be treated later on.23,24 In contrast, no more than 40% of the patients received ACE inhibitors, even though the ISIS-4 (fourth international study of infarct survival) and GISSI (Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico) -3 trials have documented the beneficial effect of early administration of these medications to patients with myocardial infarction.25,26 French cardiologists seem to reserve ACE inhibitors for patients with impaired left ventricular function.
In-hospital complications
Among patients who had in-hospital complications, 3.5% had ventricular fibrillation and 8.4% had atrial fibrillation, a figure lower than what was observed in the previous French survey.7 Five day mortality was 6.1%, which is a 21% relative reduction compared with five day mortality reported in the French 1995 survey (7.7%) and a nearly 100% reduction compared with a previous survey carried out in France in mostly academic institutions in 1984 (12.1%).7,27 In-hospital mortality was 8.7%. Reductions in in-hospital mortality in the past two decades have also been observed in most industrialised countries.28–30 Among predictors of early mortality, anterior infarct location, older age, and Killip class on admission were expected. Interestingly, low blood pressure on admission and high heart rate on admission were also potent prognostic factors for in-hospital mortality, independently of Killip class on admission. This finding emphasises the prognostic importance of haemodynamic parameters reflecting the neurohormonal balance very early in the course of acute myocardial infarction; it also emphasises the potential benefit of early administration of β blockers and the potential deleterious effect of pharmacologically induced hypotension in this setting (CONSENSUS (cooperative new Scandinavian enalapril survival study) II trial).31 In this regard, the fact that over 60% of the patients received nitrates at the early stage, despite the negative results of the GISSI-3 and ISIS-4 trial, appears disturbing.25,26 It is surprising that neither a previous myocardial infarction nor a history of congestive heart failure was associated with early outcome; one might speculate on the role of secondary prevention medications in these patients already known to have coronary artery disease. As previously observed, early reperfusion therapy was not an independent predictor of early outcome, as the benefits of such treatment are usually observed later in the course of the disease.32 Likewise, there was no difference in early outcome between the use of intravenous thrombolysis and the use of primary coronary angioplasty. The lack of an early prognostic impact of reperfusion therapy was already observed in the previous French registry carried out in 1995, as well as in other registries such as the MITI (myocardial infarction triage and intervention) registry.7,33
Medications prescribed at discharge
Much progress has been made in the prescription of secondary prevention medications at hospital discharge. Antiplatelet agents are prescribed for 95% of patients, β blockers for three patients in four, and ACE inhibitors for one patient in two. These figures indicate a slight improvement over previous surveys carried out in the second part of the 1990s.7–9 The prescription of statins, in contrast, has increased dramatically from 10% in 1995 to over 60%. Though the results of the heart protection study were not yet available when the survey was carried out, results of the 4S (Scandinavian simvastatin survival study), CARE (cholesterol and recurrent events), and LIPID (long-term intervention with pravastatin in ischaemic disease) trials seem to have convinced French cardiologists of the appropriateness of prescribing statins for patients who have sustained an acute myocardial infarction.34–37 As a result, half of the patients received triple combination treatment (antiplatelet agents, β blockers, and statins) and a quarter, quadruple combination treatment (antiplatelet agents, β blockers, statins, and ACE inhibitors) at hospital discharge. This is a huge increase in the prescription of combined treatment at hospital discharge, compared with the previous 1995 survey.38 Elderly patients (⩾ 70 years of age) were less often prescribed both β blockers (55% v 81%) and statins (44% v 70%), however, although there is no evidence of a reduced efficacy in this population.
Conclusion
The present survey of 83% of all institutions taking care of patients with acute myocardial infarction in France by the end of 2000 shows continued improvement in in-hospital outcome, compared with previous surveys. Reperfusion therapy, however, was given to barely more than 50% of the patients, a finding partially explained by the still much too long time delay between symptom onset and hospital admission: in this regard, no improvement whatsoever was found, compared with the previous 1995 nationwide survey. In contrast, continued improvement was apparent in the rates of prescription of secondary prevention medications at hospital discharge, with more than half of the population receiving triple (antiplatelet, β blocker, and statin) treatment at that time. Both the improvement in early outcome and the higher rate of prescription of secondary prevention medications at discharge are likely to result in improved long term outcome.
Acknowledgments
The authors are indebted to all physicians in the participating centres, without whose collaboration this study would not have been possible. This study was supported by a grant from Laboratoire Aventis, Paris, France