Article Text

Abstract
Objectives: To identify predictors of operative and postoperative mortality and of functional reversibility after aortic valve replacement (AVR) in patients with aortic stenosis (AS) and severe left ventricular (LV) systolic dysfunction.
Methods and results: Between 1990 and 2000, 155 consecutive patients (mean (SD) age 72 (9) years) in New York Heart Association (NYHA) heart failure functional class III or IV (n = 138) and with LV ejection fraction (LVEF) ⩽ 30% underwent AVR for critical AS (mean (SD) valve area index 0.35 (0.09) cm2/m2). Thirty day mortality was 12%. NYHA class (3.7 (0.6) v 3.2 (0.7), p = 0.004), cardiothoracic ratio (CTR) (0.63 (0.07) v 0.56 (0.06), p < 0.0001), pulmonary artery systolic pressure (63 (25) v 50 (19) mm Hg, p = 0.03), and prevalence of complete left bundle branch block (22% v 8%, p = 0.03) and of renal insufficiency (p = 0.001) were significantly higher in 18 non-survivors than in 137 survivors. In multivariate analysis, the only independent predictor of operative mortality was a CTR ⩾ 0.6 (odds ratio (OR) 12.2, 95% confidence interval (CI) 5.4 to 27.4, p = 0.002). The difference between preoperative and immediate postoperative LVEF (early-ΔEF) was > 10 ejection fraction units (EFU) in 55 survivors. In multivariate analysis, CTR (OR 5.95, 95% CI 3.0 to 11.6, p = 0.006) and mean transaortic gradient (OR 1.05, 95% CI 1.0 to 1.1, p < 0.05) were independent predictors of an early-ΔEF > 10 EFU. During a mean (SD) follow up of 4.6 (3) years, 50 of 137 (36%) 30 day survivors died, 31 of non-cardiac causes. Diabetes (OR 3.8, 95% CI 2.4 to 6.0, p = 0.003), age ⩾ 75 years (OR 2.6, 95% CI 2.1 to 4.5, p = 0.004), and early-ΔEF ⩽ 10 EFU (OR 0.96, 95% CI 0.94 to 0.97, p = 0.01) were independent predictors of long term mortality. Among 127 survivors, the percentage of patients in NYHA functional class III or IV decreased from 89% preoperatively to 3% at one year. The decrease in functional class was significantly greater in patients with an early-ΔEF > 10 EFU than patients with an early-ΔEF ⩽ 10 EFU (p = 0.02). In addition, the mean (SD) LVEF at one year was 53 (11)% in patients with an early-ΔEF > 10 EFU and 42 (11)% in patients with early-ΔEF ⩽ 10 EFU (p < 0.001).
Conclusions: Despite a relatively high operative mortality, AVR for AS and severely depressed LVEF was beneficial in the majority of patients. Early postoperative recovery of LV function was associated with significantly greater relief of symptoms and longer survival.
- AS, aortic stenosis
- AVR, aortic valve replacement
- CAD, coronary artery disease
- CI, confidence interval
- CTR, cardiothoracic ratio
- EFU, ejection fraction units
- LV, left ventricular
- LVEF, left ventricular ejection fraction
- NYHA, New York Heart Association
- OR, odds ratio
- aortic stenosis
- valvar heart disease
- left ventricular dysfunction
- aortic gradient
- aortic valve replacement
Statistics from Altmetric.com
- AS, aortic stenosis
- AVR, aortic valve replacement
- CAD, coronary artery disease
- CI, confidence interval
- CTR, cardiothoracic ratio
- EFU, ejection fraction units
- LV, left ventricular
- LVEF, left ventricular ejection fraction
- NYHA, New York Heart Association
- OR, odds ratio
- aortic stenosis
- valvar heart disease
- left ventricular dysfunction
- aortic gradient
- aortic valve replacement
The average life expectancy of patients with severe aortic stenosis (AS) complicated by overt congestive heart failure is about two years.1 Surgical aortic valve replacement (AVR) is the only effective corrective treatment, prolongs survival, and greatly alleviates symptoms.2 Along with age,3 New York Heart Association (NYHA) functional class,4,5 coexistent coronary artery disease (CAD), and a low transvalvar gradient,5,6 left ventricular (LV) systolic dysfunction appears to be a key operative and postoperative prognostic factor in patients with severe AS.7 However, few recent studies have been conducted in large enough patient populations to re-examine their long term outcomes after surgery. This retrospective analysis was performed to detect factors predictive of operative and postoperative mortality, to identify indicators of rapidly reversible LV systolic dysfunction, and to examine the relation between early recovery of LV systolic function and long term prognosis.
PATIENT POPULATION AND METHODS
Inclusion and exclusion criteria
All patients with LV ejection fraction (LVEF) ⩽ 30% who underwent AVR between 1990 and 2000 for AS with valve area ⩽ 1 cm2 at our institution were included in this analysis. LVEF was measured preoperatively by echocardiography. Patients with histories of previous cardiac surgery, associated grade 3 or 4 aortic or mitral regurgitation, or concomitant operations on other valves, except for mitral valve repair, were excluded from the analysis. Concomitant coronary artery bypass graft surgery was not an exclusion factor.
Preoperative assessment
Preoperative clinical data, including chest x ray, Doppler echocardiography, cardiac catheterisation, and coronary artery anatomy, were collected by review of the medical records of 155 eligible patients (table 1), representing 4.1% of the entire population of patients who underwent AVR for AS (n = 3819) during the same period. All patients underwent two dimensional and Doppler echocardiography ⩽ 30 days before the operation. LVEF was calculated according to the biplane Simpson’s rule for 55 patients. When this method was not feasible in the other 100 patients, LVEF was estimated visually.8,9 The intraindividual and interindividual variabilities for the visual method were estimated as 2 (2)% and 4 (3)%, respectively in our echocardiography laboratory. Aortic valve haemodynamic data were calculated by standard methods and aortic valve area by the continuity equation. CAD was defined as ⩾ 50% luminal diameter narrowing of the left main coronary artery or ⩾ 70% narrowing of one or more major epicardial vessels. Cardiac output, calculated by the thermodilution method, and pulmonary artery pressures, measured with a Swan-Ganz catheter, were recorded at the time of cardiac catheterisation. Renal insufficiency was defined as a serum creatinine concentration > 132 mmol/l. Non-elective operation was defined as urgent or emergent surgery.
Preoperative characteristics of the patient population
Operative data
The type and size of the aortic prosthetic valve, concomitant coronary artery bypass graft surgery, or mitral valve repair and the aortic cross clamp and cardiopulmonary bypass durations were recorded and are presented in table 2.
Operative characteristics
Postoperative assessment
In-hospital assessment
The immediate postoperative LVEF was measured echocardiographically before the patient was discharged from the hospital at a median of seven days (range 4−10 days) after AVR in 123 of 137 patients who survived past 30 days. The difference between immediate postoperative and preoperative LVEF was defined as early-ΔEF and expressed as ejection fraction units (EFU).
Long term assessment
Survival status and NYHA functional class were assessed at 12 months in all patients. Late postoperative LVEF was measured echocardiographically at a median of 12 months (range 9−15 months) after AVR.
Statistical analysis
Quantitative unpaired parametric data, expressed as mean (SD), were compared by Student’s t test. The χ2 test was used to analyse qualitative data expressed as percentages. A multiple logistic regression analysis was performed to identify predictors of operative mortality, defined as death within 30 days after AVR, based on all baseline characteristics listed in tables 1 and 2. The relation between preoperative variables and early-ΔEF was examined by simple and multiple linear regression analyses and presented as an odds ratio (OR) and 95% confidence interval (CI).
Overall survival was estimated by the non-parametric Kaplan-Meier method (follow up was stopped on 31 August 2002). Predictors of mortality were analysed by the Cox proportional hazards model. A probability value of p < 0.05 was considered significant. Data were analysed with SPSS version 10.1 software (SPSS Inc, Chicago, Illinois, USA).
RESULTS
Study population
Tables 1 and 2 present the preoperative characteristics of the patient population and important surgical information.
Thirty day outcomes
Operative mortality
The 30 day mortality was 12% (18 of 155 patients) versus 6.5% in the overall AS surgical database of our institution during the same period. Fourteen (78%) of 18 operative deaths were of cardiac cause: 10 from intractable low cardiac output and four from valve related complications (two cerebral embolisms, one thrombosis, and one sudden unexplained cardiac death). The other four were of non-cardiac causes (three mesenteric infarctions, one infection). In univariate analysis, NYHA functional class (3.7 (0.6) in non-survivors v 3.2 (0.7) in survivors; p = 0.004), cardiothoracic ratio (CTR) (0.63 (0.07) v 0.56 (0.06), p < 0.0001), pulmonary artery systolic pressure (63 (25) v 50 (19) mm Hg, p = 0.03), complete left bundle branch block (22% v 8%, p = 0.03), and renal insufficiency (50% v 9%, p = 0.001) were predictive of operative mortality. In multivariate analysis, CTR ⩾ 0.6 was the only predictor of operative mortality (OR 12.2, 95% CI 5.4 to 27.4). Non-elective surgery and CAD did not appear as predictive of fatal outcome.
Early postoperative ΔEF
LVEF was measured echocardiographically at a mean of 7 (2) days after AVR in 123 of 137 (90%) 30 day survivors. Among the patients whose LVEF was measured postoperatively, 99 (80%) had an early-ΔEF > 0 (fig 1). The mean preoperative LVEF was 25 (5)% versus 36 (12)% postoperatively (mean increase 11 (11) EFU, p < 0.001). The early-ΔEF was > 10 EFU (mean 21 (8), range 11−50) in 55 patients (45%) and ⩽ 10 EFU in 68 patients (mean 3 (6), range −16–10). By multivariate analysis, an early-ΔEF > 10 EFU was positively associated with a higher preoperative mean aortic gradient (OR 1.05, 95% CI 1.0 to 1.1, p = 0.045) and was inversely correlated with a higher CTR (OR 5.95, 95% CI 3.0 to 11.6, p = 0.006).

Distribution of change between early postoperative and preoperative ejection fraction (early-ΔEF) of ⩽10 ejection fraction units (EFU) (dark bars) versus >10 EFU (light bars) among 123 operative survivors after aortic valve replacement.
Long term outcomes
Mortality
No patient was lost to follow up. Among the 137 survivors to 30 days, 50 patients (36%) died during a median follow up of 4.6 (3) years (range 1.8−11.6 days) (fig 2). Late deaths were from non-cardiac causes in 31 patients (62%). The estimated five year survival of the population after AVR was 71%. In Cox proportional hazard analysis, diabetes mellitus (OR 3.8, 95% CI 2.4 to 6.0, p = 0.003), age ⩾ 75 years (OR 2.6, 95% CI 2.1 to 4.5, p = 0.004), and early-ΔEF ⩽ 10 EFU (OR 0.96, 95% CI 0.94 to 0.97, p = 0.01) were independently associated with fatal long term outcomes (fig 3). Mean preoperative aortic gradient (although only 11% of patients had a mean gradient ⩽ 30 mm Hg), preoperative LVEF, presence of CAD, and prosthesis size were not significantly associated with survival. Moreover, in this population with greatly reduced LVEF, the preoperative LVEF did not appear as a significant predictor of long term outcome.

Actuarial survival of 137 operative survivors. The x axis shows the number of patients at risk during follow up.
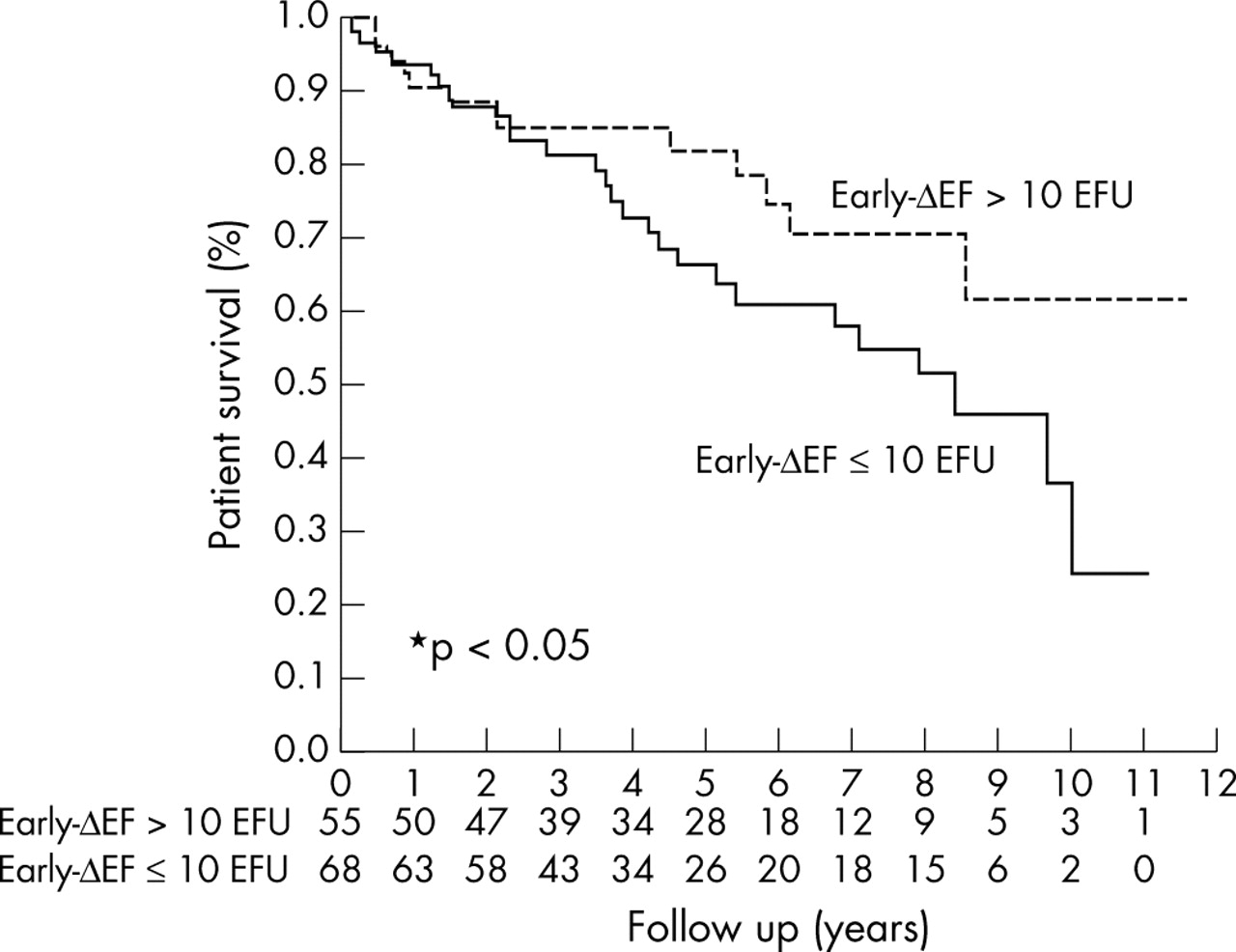
Actuarial survival of patients with early-ΔEF ⩽10 EFU versus early-ΔEF >10 EFU. The x axis shows the number of patients at risk during follow up.
Functional outcomes
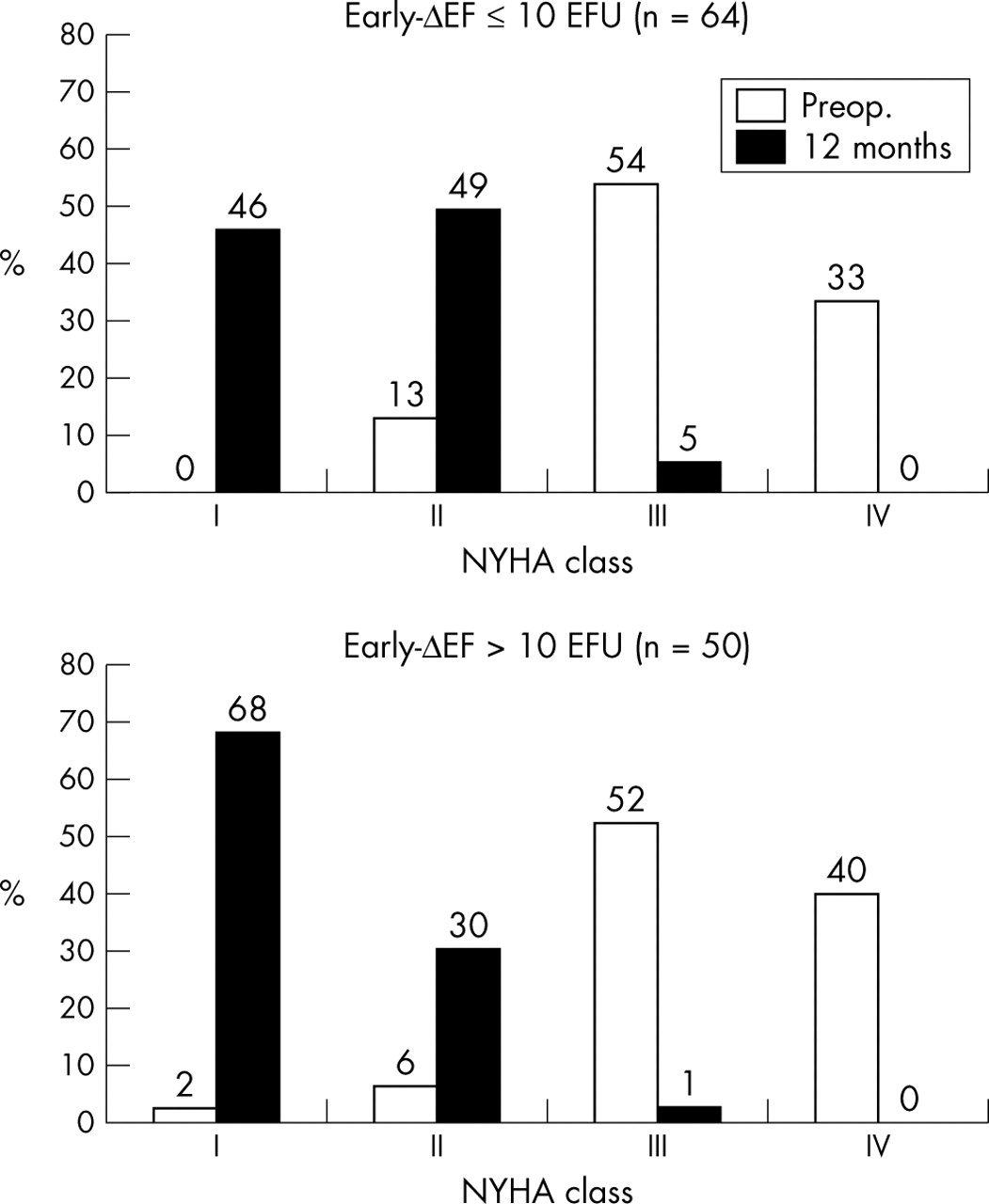
Among the 127 survivors to one year of follow up, the percentage of patients in NYHA functional class III or IV decreased from 89% to 3%. At 12 months, four patients remained in NYHA functional class III and 65% had improved by two or more classes and 95% by one or more classes. The decrease in functional class was significantly greater in patients with an early-ΔEF > 10 EFU than in patients with an early-ΔEF ⩽ 10 EFU (p = 0.02) (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in New York Heart Association (NYHA) functional class between preoperative assessment and 12 month follow up of patients with early-ΔEF ⩽10 EFU versus early-ΔEF >10 EFU.
Late postoperative ΔEF
LVEF was measured by echocardiography at 12 months after AVR in 110 of the 127 (87%) one year survivors. An additional increase was observed in 106 patients (96%). The mean increase was 22 (13) EFU, from 25 (5)% preoperatively to 47 (12)% at 12 months (p < 0.001). The mean LVEF at 12 months was significantly higher in patients with an early-ΔEF > 10 EFU (53 (11)%) than in patients with an early-ΔEF ⩽ 10 EFU (42 (11)%, p < 0.001). The mean preoperative LVEF was similar in both groups (25 (10)% v 26 (5)%, p = 0.54).
DISCUSSION
AS is the most common adult valvar disease in developed countries.10 Its prevalence approaches 5% beyond 75 years of age.11 When AS is symptomatic, its dismal natural course can only be deflected by AVR,12 which is likely to bring about a functional improvement despite the presence of LV systolic dysfunction preoperatively.7 This treatment benefit is greatest when systolic dysfunction is primarily caused by afterload mismatch from actual valvar stenosis and is least likely in the presence of primary contractile dysfunction unrelated to valvar disease (aortic pseudostenosis).13 Few sufficiently powered recent studies have examined the operative and postoperative outcomes of patients with severe AS and profoundly depressed LV function. Furthermore, to our knowledge, none has focused on the identification of predictors of early recovery of contractile function.
Main study findings
The main findings of our relatively large and recent surgical experience are, firstly, that operative mortality was acceptable and proportional to the degree of cardiomegaly; secondly, that the degree of early postoperative recovery of LV systolic dysfunction was correlated with preoperative mean transaortic gradient and CTR, which can be regarded as indirect indices of global LV function status; and, thirdly, the observation of a clear postoperative LV function benefit, which was most pronounced when apparent at the time of discharge from the hospital and when its magnitude was > 10 EFU.
Operative mortality
The 12% operative mortality observed in our population was similar to that previously reported in earlier studies of patients with major LV systolic dysfunction and severe AS.7,14,15 In the present study, among multiple baseline characteristics examined, a CTR ⩾ 0.60 was the only independent predictor of operative mortality, which was increased 12-fold. CTR, therefore, emerged as a more reliable indicator of myocardial failure than NYHA functional class or pulmonary arterial systolic pressure, both greatly increased in our population and therefore less discriminate.
Advanced CAD was not a significant predictor of surgical mortality in our study, in contrast to a study from the Mayo Clinic.7 In that US study, over 50% of patients had ischaemic heart disease (as opposed to about one quarter of our patients) and had undergone concomitant coronary revascularisation (versus 13% of our patients). In addition, 25% (versus 10% of our patients) had a prior myocardial infarction. Therefore, the smaller prevalence of CAD may explain its lack of prognostic value in our study, while strengthening the relation between LV systolic dysfunction and valvar disease.
Only about 10% of our patients presented with a transaortic gradient ⩽ 30 mm Hg, which did not emerge as a prognostic indicator, in contrast to the findings of others.16,17 The persistence of a relatively high mean transvalvar gradient in the face of prominent LV dysfunction was consistent, in the majority of our patients, with a severe stenotic (rather than pseudostenotic) process.18 True AS is associated with a higher likelihood of reversible LV dysfunction, which, in our population, was observed in 80% of survivors.
Early recovery of LVEF
LV systolic dysfunction was more likely to recover rapidly when preceded by a high mean preoperative transaortic gradient and with a smaller degree of cardiomegaly. These observations are consistent with earlier reports where the reversibility of LV systolic dysfunction was most likely in the presence of a mean preoperative transvalvar gradient > 30 mm Hg.16,19 In the study by Connolly et al,7 recovery of systolic function, analysed at a mean of 14 months after surgery, was predicted by the mean transaortic gradient and rate of transvalvar flow in univariate analysis, and by a lower severity of CAD and a narrower preoperative aortic valve area in multivariate analysis. In advanced AS, compensatory LV hypertrophy may be overwhelmed and the maintenance of systolic function near normal values depends on the recruitment of a preload reserve by an increase in LV end diastolic pressure.20 At end stage, when this reserve is exhausted, wall stress continues to increase and systolic dysfunction develops together with afterload mismatch. This secondary LV dysfunction may be reversed by removing the mechanical barrier as shown by our results and those of others.21 However, the degree of LV dilatation, probably an indirect manifestation of myocardial fibrosis, seems to be a determinant in the evolution of the disease, being a predictor of intractable perioperative heart failure as well as of incomplete recovery of systolic function.
Long term outcomes
About two thirds of our patients were alive at the end of over four and a half years of follow up, and 62% of long term deaths were attributable to non-cardiac causes. Whereas nearly 90% of our patients were in advanced heart failure before undergoing AVR, < 5% were in NYHA functional class III or IV at one year. Though the operative risk was increased, AVR in severe AS complicated by advanced systolic dysfunction was clearly beneficial as has been reported by others.6,7,21
Besides the factors regularly identified in multivariate analyses, such as older age and diabetes, the absence of an early and significant postoperative increase in LVEF was also predictive of late mortality—to our knowledge a new observation. In multivariate analysis, patients with an early-ΔEF > 10 EFU survived significantly longer and had a greater functional recovery at one year than patients with an early-ΔEF ⩽ = 10 EFU.
Study limitations
This analysis had several limitations, most of them being inherent to the retrospective study design. Firstly, associated CAD, combined coronary revascularisation, or mean preoperative transaortic gradient was not predictive of operative mortality in our study, in contrast to the findings of others. These results are probably explained by the unusually low prevalence of each of these factors in the present study (respectively, 27%, 13%, and 11%). These particularities may raise the question of possible selection bias in this population. Secondly, because of missing echocardiographic measurements, the degree of LV cavity dilatation was indirectly ascertained from the CTR. Thirdly, although follow up was complete with respect to long term morbidity and mortality, echocardiograms were not recorded at the time of hospital discharge in 10% and at one year in 4% of patients. Fourthly, our choice of a 10% increase in LVEF as a cut off value of early recovery of systolic function may seem arbitrary. This choice was based on the intraobserver and interobserver variabilities generally observed in studies based on measurements of echocardiographic cardiac dimensions.22–24 Lastly, we did not evaluate the presence of contractile reserve by dobutamine or exercise stress echocardiography, a method found useful to predict survival after AVR of patients with severe AS and a low mean transvalvar gradient.15,25
Conclusion
The high long term survival, significant decrease in NYHA functional class, and major improvement in LV function observed in this analysis indicate that most patients with severe AS and depressed LVEF should be considered candidates for AVR. Interestingly, early postoperative recovery of LV function was associated with significantly greater relief of symptoms and with longer survival.