Article Text

Statistics from Altmetric.com
- ACC, American College of Cardiology
- ACS, acute coronary syndromes
- AHA, American Heart Association
- CI, confidence interval
- FRISC, Fagmin and fast revascularisation during instability in coronary artery disease
- GRACE, global registry of acute coronary events
- LMWH, low molecular weight heparin
- OR, odds ratio
- TIMI, thrombolysis in myocardial infarction
- acute coronary syndromes
- risk stratification
- non-ST segment elevation myocardial infarction
- recurrent ischaemia
- outcomes
Early risk assessment is crucial to the management of patients presenting with unstable angina or non-ST segment elevation myocardial infarction. The importance of this approach is emphasised in current guidelines for the management of patients with acute coronary syndromes (ACS) without persistent ST segment elevation from the European Society of Cardiology1 and the American College of Cardiology/American Heart Association (ACC/AHA).2 These guidelines recommend that patients judged to be at high risk can be offered more aggressive pharmacological and interventional treatment, whereas those thought to be at low risk may be managed acutely in a less intensive manner.
“Low risk” does not mean “no risk”, with a three year cardiac event rate as high as 12% being noted in troponin negative patients in selected study populations.3 However, the incidence of events in a lower risk population has not been well described in patients routinely encountered in clinical practice.
The most commonly applied methods of risk stratification include identification of patients with haemodynamic instability, dynamic ECG changes, or increases in serum enzymes such as troponin. Troponin assays play an integral part in risk stratification, with troponin positive patients noted to be at higher risk of subsequent events. These events can be reduced by the use of glycoprotein IIb/IIIa antagonists, low molecular weight heparins (LMWHs), and early revascularisation strategies.4–6 Although multivariable models derived from clinical trial datasets such as the TIMI (thrombolysis in myocardial infarction) risk score have been used to develop global assessments of risk,5 currently most clinicians use simple criteria such as troponin rise and ST segment change on an ECG to identify high risk patients. We therefore determined how reliably these criteria identified patients at greatest likelihood of an event by quantifying the risk among the lower risk population. A secondary goal was to document approaches to further risk stratification and management strategies in this lower risk group: risk assessment, management practices, and outcomes were compared with those in the high risk population.
METHODS
Full details of the GRACE (global registry of acute coronary events) methods have been published.7–9 GRACE is designed to reflect an unbiased population of patients with ACS, irrespective of geographical region. More than 120 hospitals located in 14 countries in North and South America, Europe, Australia, and New Zealand have contributed data to this observational study.
To ensure the enrolment of an unbiased population, the first 10–20 consecutive patients (depending on each site’s patient throughput) were recruited from each site every month. Patients entered in the registry had to be at least 18 years old and alive at the time of hospital presentation, be admitted for ACS as a presumptive diagnosis (that is, have symptoms consistent with acute ischaemia), and have at least one of the following: ECG changes consistent with ACS, serial increases in serum biochemical markers of cardiac necrosis, and documentation of coronary artery disease. The qualifying ACS must not have been precipitated or accompanied by a significant non-cardiovascular co-morbidity, trauma, or surgery. At about six months after hospital discharge, patients were followed up to ascertain the occurrence of selected long term study outcomes. Where required, study investigators received approval from their local hospital ethics or institutional review board.
Trained coordinators collected data on standardised case report forms. Demographic characteristics, medical history, presenting symptoms, duration of pre-hospital delay, biochemical and ECG findings, treatment practices, and a variety of hospital outcome data were collected (full definitions are provided at www.outcomes.org/grace). Standardised definitions of all patient related variables and clinical diagnoses were used. Standardised definitions were also used for selected hospital complications and outcomes.8
Patients presenting with ST segment elevation myocardial infarction or new left bundle branch block were excluded from this study. Lower risk was defined as unstable angina as the discharge diagnosis in the absence of dynamic ST segment changes, positive troponin assay (or other cardiac markers), and haemodynamic or arrhythmic instability. High risk patients had one or more of the above features noted on presentation.
Statistical methods
Descriptive statistics (percentages for discrete variables, and medians with 25th and 75th centiles for continuous variables) were generated for the patients’ baseline characteristics, ECG data, cardiac markers, and clinical outcomes. Baseline characteristics and clinical outcomes were compared between patient groups by χ2 tests for differences in proportions of categorical variables and Wilcoxon sum rank test for differences in continuous variables. All tests were two sided and considered significant at α ⩽ 0.05.
The lower risk population was analysed by multivariable Cox regression to determine the factors associated with death from the hospital discharge to six months’ follow up. Multivariable logistic regression was used to ascertain the variables associated with rehospitalisation for cardiac related illness and readmission for revascularisation at six months after discharge. Statistical analyses were performed with the SAS software package (version 8.2, SAS Institute, Cary, North Carolina, USA).
RESULTS
In-hospital outcome data were available for 11 885 consecutive patients with non-ST segment elevation ACS enrolled in GRACE between July 1999 and September 2002. A total of 4252 patients (36%) were defined as being at lower risk. Table 1 shows the baseline characteristics of the lower risk and high risk groups. The lower risk patients were slightly younger (mean age 65 v 67 years, p < 0.0001) and were more likely to be women (1675 of 4232 (40%) v 2765 of 7577 (36%), p = 0.0009) than patients in the high risk group. Hypertension (2795 of 4227 (66%) v 4783 of 7588 (63%), p = 0.0008) and hyperlipidaemia (2396 of 4219 (57%) v 3363 of 7550 (45%), p < 0.0001) were noted more often in the lower risk group. No significant difference between groups was noted in the incidence of diabetes mellitus or smoking. Lower risk patients were more likely to have documented coronary artery disease (1814 of 3961 (46%) v 1965 of 7357 (27%), p < 0.0001). New ECG changes were more frequent in the high risk group (5373 of 7237 (74%) v 1719 of 3917 (44%), p < 0.0001). Increased troponin concentrations were noted in 4038 of 5379 (75%) of the high risk group. On admission, lower risk patients were more likely to be taking long term angiotensin converting enzyme inhibitors (135 of 4195 (32%) v 2089 of 7556 (28%), p < 0.0001), aspirin (2558 of 4247 (60%) v 3191 of 7617 (42%), p < 0.0001), β blockers (1903 of 4226 (45%) v 2335 of 7599 (31%), p < 0.0001), calcium channel blockers (1165 of 4180 (28%) v 1639 of 7521 (22%), p < 0.0001), nitrates (1590 of 4232 (38%) v 1870 of 7589 (25%), p < 0.0001), and statins (1468 of 4207 (35%) v 1608 of 7557 (21%), p < 0.0001).
Patients’ baseline characteristics on admission
Hospital risk stratification and management
Non-invasive testing to further aid risk stratification of patients was used in 1163 of 4207 (28%) of lower risk patients and 1531 of 7521 (20%) of the high risk population (p < 0.0001) (table 2). Angiography (3860 of 7544 (51%) v 1930 of 4190 (46%), p < 0.0001) and echocardiography (4348 of 7533 (58%) v 1692 of 4190 (40%), p < 0.0001) were more likely to be performed in the high risk group (fig 1). Overall, neither coronary angiography nor functional assessment for coronary ischaemia was performed during hospital admission in 2746 of 7437 (37%) of the high risk and 1499 of 4148 (36%) of the lower risk patients.
In-hospital procedures

Investigations performed in risk stratification of lower risk and high risk patients.
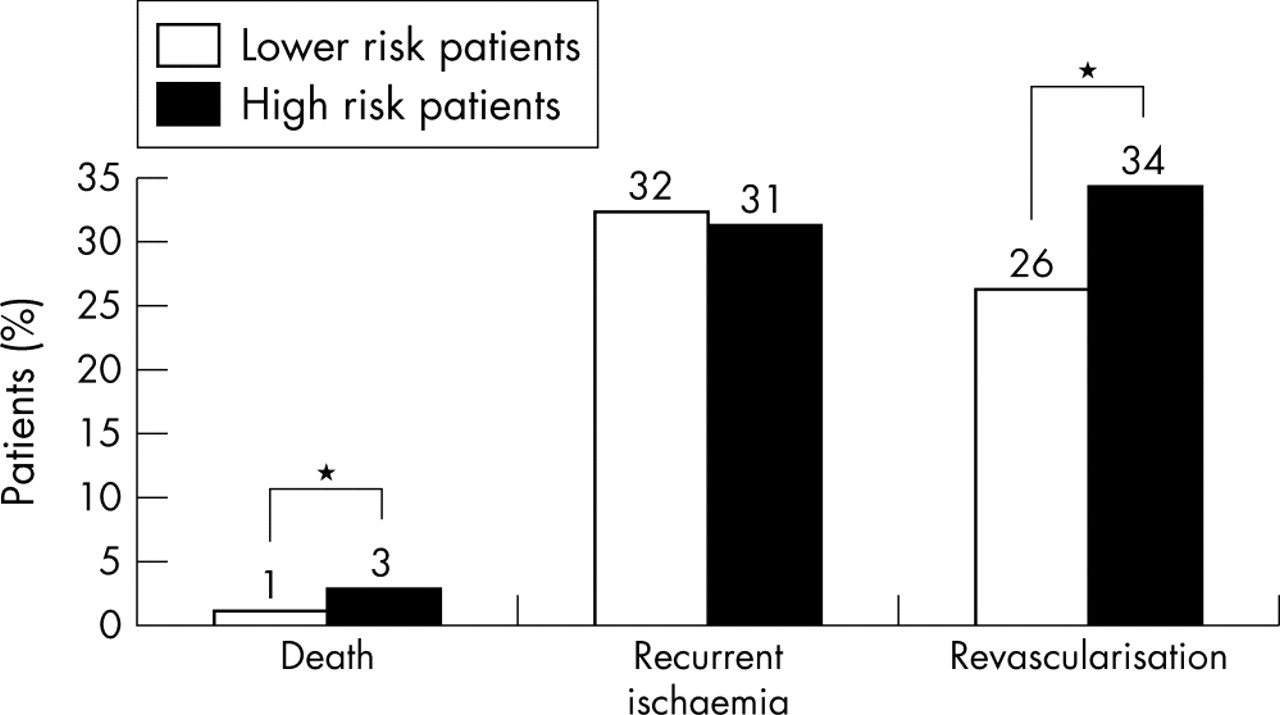
One in four lower risk patients underwent either angioplasty or coronary artery bypass grafting before discharge, although statistically more revascularisation procedures were performed in the high risk group (2567 of 7519 (34%) v 1094 of 4161 (26%), p < 0.0001) (fig 2).

In-hospital events. *p ⩽ 0.0001.
In-hospital administration of unfractionated heparin, LMWH, and glycoprotein IIb/IIIa antagonists differed between high risk and lower risk groups, as table 1 shows. In both groups, all classes of medication were prescribed more often on discharge than on admission. Similar proportions of patients on discharge were taking aspirin (3348 of 3856 (87%) v 5798 of 6603 (88%), not significant) and statins (2009 of 3822 (53%) v 3401 of 6566 (52%), not significant). The use of β blockers remained fairly conservative (4710 of 6593 (71%) v 2657 of 3838 (69%), p = 0.0168). Other antianginal agents were more often prescribed to the lower risk group (nitrates 2228 of 3843 (58%) v 3353 of 6583 (51%), p < 0.0001; calcium channel antagonists 1333 of 3813 (35%) v 1663 of 6542 (25%), p < 0.0001). The use of angiotensin converting enzyme inhibitors increased significantly in both groups at discharge, with 1738 of 3823 (46%) of lower risk and 3326 of 6560 (51%) of high risk patients receiving these drugs (p < 0.001). Figure 3 illustrates medical treatment on admission and discharge in the lower risk group.

Medication on admission and discharge in lower risk patients. ACE, angiotensin converting enzyme.
Hospital and post-discharge events
Figure 2 shows hospital events. Death was uncommon in both groups but was statistically less likely in the lower risk group (41 of 4227 (1%) v 215 of 7586 (2.8%), p < 0.0001). No difference between the groups was noted in the recurrence of ischaemia (1354 of 4231 (32%) v 2313 of 7587 (31%), not significant).
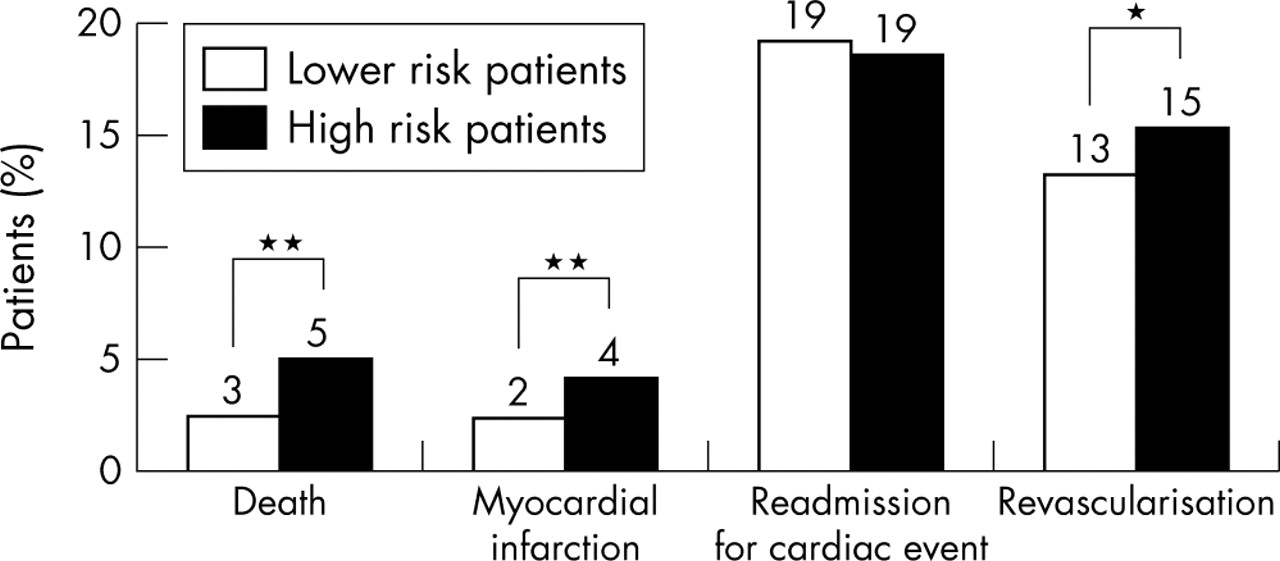
Of the 11 885 patients for whom in-hospital data were available, 10 573 were eligible for follow up and outcome data were available for 8796 (83%). Figure 4 illustrates clinical events up to six months after discharge. Patients in the high risk group were twice as likely to die (302 of 5451 (5.5%) v 79 of 3223 (2.5%), p < 0.0001) as the lower risk group. Rehospitalisation rates with further cardiac related problems were similar in both groups, with one in five patients readmitted. Lower risk patients were less likely to undergo a revascularisation procedure during the six month follow up period (412 of 3128 (13%) v 800 of 5224 (15%), p = 0.007).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Clinical events up to six months after discharge. *p = 0.007; **p ⩽ 0.0001.
Multivariable analysis was performed in the lower risk group to predict outcome at six months. Patients taking aspirin on discharge were less likely to die (hazard ratio 0.4, 95% confidence interval (CI) 0.26 to 0.75) and patients with a history of congestive heart failure (hazard ratio 1.72, 95% CI 1.00 to 2.97) were more likely to die; the likelihood of death rose with increasing age per 10 year increase (hazard ratio 2.37, 95% CI 1.82 to 3.51).
Rehospitalisation for a cardiac related illness within six months was more often noted in patients with a history of smoking (odds ratio (OR) 1.2, 95% CI 1.0 to 1.5), a history of coronary artery disease (OR 1.5, 95% CI 1.0 to 1.5), a history of atrial fibrillation (OR 2.0, 95% CI 1.5 to 2.7), or taking a statin on discharge (OR 1.3, 95% CI 1.0 to 1.6) and if the patient underwent percutaneous coronary intervention during the index admission (OR 1.6, 95% CI 1.3 to 2.0). Readmission was less likely if the patient was taking aspirin on discharge (OR 0.7, 95% CI 0.5 to 0.9) and if surgical revascularisation was performed (OR 0.5, 95% CI 0.3 to 0.9). More men (OR 1.8, 95% CI 1.3 to 2.4) and patients who had a history of hyperlipidaemia (OR 1.4, 95% CI 1.1 to 1.9) were readmitted for revascularisation.
DISCUSSION
ACS remain one of the most common reasons for hospital admission worldwide. Enthusiasm in recent times has centred on identification of the high risk patient, with trial evidence showing a benefit of early interventional based treatment in this population.6,10,11 Troponin status and the presence or absence of dynamic ECG changes remain the most widely used aids for the risk stratification of patients on presentation,6,10,11 and this approach has been widely promulgated in international guidelines.1,2
There are more involved techniques for estimation of risk than those selected for this analysis. One method promoted in the ACC/AHA guidelines involves the TIMI risk score.5 The seven variables in this score are age 65 years or older, at least three risk factors for coronary artery disease, prior coronary stenosis of 50% or greater, ST segment changes on presentation, at least two anginal events in the preceding 24 hours, use of aspirin in the previous seven days, and increased cardiac markers. Risk increases in parallel with TIMI score, with a major adverse cardiac event at 14 days noted in 41% of patients in the TIMI 11B trial with a TIMI risk score of 6 or 7.5 Recently, Granger et al,12 for the GRACE investigators, reported a new risk assessment model based on the spectrum of patients with ACS seen in everyday practice. Eight independent risk factors were assessed and they included, for the first time, two variables not previously identified from clinical trial databases: baseline creatinine concentration and cardiac arrest at presentation. This GRACE model is an excellent tool for assessing the risk for death and can be used as a simple nomogram to estimate risk in individual patients, with the advantage of general applicability across the full spectrum of ACS.12
Both the TIMI and GRACE risk scores are best applied when the clinician has access to a personal digital assistant. This is not commonplace internationally; the TIMI score is not widely applied in clinical practice outside the USA. Furthermore, there is no evidence to date that application of risk scores such as these will result in improved patient outcomes when compared with simple bedside risk stratification based on troponin status and the presence or absence of dynamic ECG changes.
Our study focused on the clinically identified lower risk population. Stubbs et al3 noted a three year rate of major cardiac adverse events of 12% in a low risk population defined as being troponin negative. Lindahl et al,13 for the FRISC (Fragmin and fast revascularisation during instability in coronary artery disease) study group, reported a lower risk of death or myocardial infarction of 4.3% with a shorter follow up period of five months. We found a similar event rate in our study population. In contrast to the FRISC group, however, we have presented additional information on readmission for cardiac related conditions. These were observed in almost 20% of our population, emphasising the burden these patients place on our health care systems.
Enrolment in GRACE requires symptoms consistent with a diagnosis of ischaemia plus one of the following: a history of known coronary artery disease, ECG changes consistent with ACS, or increased cardiac markers. The lower risk group in our study attained a calculated TIMI risk score of 2–4 and thus cannot be regarded as being at low risk. Event rates at 14 days of between 8.3% and 19.9% have been noted in patients with similar TIMI scores.5 Interestingly, patients with this risk profile have not been found to benefit consistently from the use of LMWHs, glycoprotein IIb/IIIa antagonists, and early intervention.4–6 These treatments were offered to high risk patients only slightly more often, confirming reports that there is a deficiency of application of evidence based treatments across the spectrum of patients with ACS.14,15
The use of non-invasive testing for ischaemia and assessment of left ventricular function to further risk stratify the lower risk population is recommended in European Society of Cardiology and ACC/AHA guidelines.1,2 There is little evidence to suggest that this approach aids the further risk stratification of high risk ACS patients, yet, in our cohort, one in five high risk patients underwent stress testing. Presumably this reflects limitations on access to catheterisation laboratories because patients from a number of sites without catheterisation facilities were enrolled in GRACE. Conversely, prognostic assessment with stress testing was undertaken in only 1163 of 4207 (28%) of the lower risk cohort in GRACE, which is the population that is likely to benefit from further risk assessment.16 There was a relatively high incidence of angiography (1930 of 4190 (46%)) in this population, with recurrent angina noted in about half of the lower risk population who underwent angiography. Thus, it appears that a significant proportion of lower risk patients underwent angiography that was not ischaemia driven, suggesting that angiography may be used as an aid to risk stratify the lower risk cohort in some centres. Nonetheless, more than a third of these patients did not undergo any form of risk stratification, either stress testing or coronary angiography, after admission. It is worth noting that these patients had a greater prevalence of known coronary disease than the higher risk population; it is possible, therefore, that coronary ischaemia had been assessed previously and was therefore not required on this occasion. Interestingly, though, a similar proportion of high risk patients did not undergo any further risk stratification or followed a non-invasive management pathway, despite the evidence of the incremental benefit of coronary angiography in this population.
More of the lower risk group were taking antianginal agents on discharge. Of some concern is that β blockers, which should be regarded as the first line antianginal treatment of choice unless contraindicated, were not prescribed to nearly one third of patients in both groups at discharge.
By six months after discharge from hospital, mortality (79 of 3223 (2.5%)) in the lower risk cohort was appreciable, although lower than in high risk patients. Readmission rates were similar in both groups, with one in five patients presenting again with a cardiac related problem, emphasising the burden these patients place on health care systems. The performance of coronary angioplasty was predictive of readmission and was most likely related to restenosis. One would anticipate that the application of drug eluting stents will affect readmission rates in this population. GRACE will be positioned to audit this prospectively.
Factors that were associated with a reduced likelihood of readmission included the prescription of aspirin at discharge and the performance of coronary artery bypass grafting. The protective effect of aspirin has recently been documented in GRACE, with less severe clinical presentation and better outcome in patients presenting with ACS who were previously taking aspirin.17
Study strengths and limitations
GRACE is the largest ongoing multinational registry to include the complete spectrum of ACS patients. In addition, GRACE employs standardised criteria for defining ACS and hospital outcomes and the most rigorous quality control and audit measures of any ongoing or previously published registry dataset. A limitation that can apply to registries of this nature is that the information provided is often extracted from the medical record, requiring second hand interpretation by the study coordinator or physician. However, high risk features of presentation with ACS, which were crucial to the stratification in this analysis, are almost invariably well documented in the medical record and were therefore unlikely to be subject to misinterpretation.
Conclusions
Patients presenting with lower risk features in GRACE have a low incidence of death and myocardial infarction in hospital. However, recurrent ischaemia is just as frequent in this population as in high risk patients. The use of non-invasive testing for further risk stratification is low despite recommendations in current practice guidelines. Angiography is used for risk stratification in a significant proportion of patients, but more than a third do not undergo any form of risk stratification while in hospital. Approaches to further risk stratification and management strategies are similar between lower risk and high risk populations, with revascularisation procedures performed almost as often in the two groups. Patients are often given less than optimal treatment on discharge, and in the six months after discharge lower risk patients are as likely as high risk patients to present again with a cardiac related condition. Our global data show that risk assessment strategies are not applied sufficiently often to patients with ACS regardless of their presenting characteristics. It remains to be seen whether wider application of more accurate risk stratification tools will have an impact on evidence based application of invasive or non-invasive strategies after admission.
GRACE SCIENTIFIC ADVISORY COMMITTEE
Keith AA Fox, UK; Joel M Gore, USA (GRACE Co-chairs); Kim A Eagle, USA; Philippe Gabriel Steg, France (GRACE Publication Committee Co-chairs); Giancarlo Agnelli, Italy; Frederick A Anderson Jr, USA; Álvaro Avezum, Brazil; David Brieger, Australia; Andrzej Budaj, Poland; Marcus D Flather, UK; Robert J Goldberg, USA; Shaun G Goodman, Canada; Christopher B Granger, USA; Dietrich C Gulba, Germany; Enrique P Gurfinkel, Argentina; Brian M Kennelly, USA; Werner Klein, Austria; José López-Sendón, Spain; Gilles Montalescot, France; Frans Van de Werf, Belgium.
Acknowledgments
The authors thank the physicians and nurses participating in GRACE. Further information about the project, along with the complete list of participants, can be found at www.outcomes.org/grace. The authors are grateful to Sophie Rushton-Mellor, PhD, for editorial assistance. The GRACE study is supported by an unrestricted grant from Sanofi-Aventis to the Center for Outcomes Research, University of Massachusetts Medical School.
REFERENCES
Footnotes
-
Ethical approval: Where required, local approval from institutional review boards was obtained.