Article Text

Abstract
Objective: To study whether emergent intracoronary autologous bone marrow cell transplantation (BMT) is applicable for the treatment of acute myocardial infarction (AMI).
Methods: 20 patients admitted within 24 h after the onset of a first AMI were randomly allocated to receive intracoronary autologous BMT (n = 10) or bone marrow supernatant (controls, n = 10) immediately after primary percutaneous coronary intervention. Left ventricular ejection fraction (LVEF), left ventricular end diastolic internal diameter (LVDd) and myocardial perfusion defect scores were examined respectively by echocardiography and single-photon emission computed tomography at one week and six months after AMI.
Results: From one week to six months after AMI, LVEF was enhanced from mean 53.8 (SD 9.2)% to 58.6 (9.9)% (p < 0.05) in the BMT group but was unchanged in the control group (58.2 (7.5)% v 56.3 (3.5)%, p > 0.05); LVDd remained unchanged (52.5 (2.8) v 52.1 (3.2) mm, p > 0.05) in the BMT group but was significantly enlarged in the control group (50.4 (6.0) v 55.2 (7.1) mm, p < 0.05). Additionally, myocardial perfusion defect scores decreased from 21 (11) to 13 (10) (p < 0.01) in the BMT group but were unchanged in the control group (20 (14) v 17 (15), p > 0.05).
Conclusion: Emergent intracoronary transplantation of bone marrow mononuclear cells after AMI is practicable, and it improved cardiac function, prevented myocardial remodelling and increased myocardial perfusion at six months’ follow up.
- AMI, acute myocardial infarction
- BMCs, bond marrow stem cells
- BM-MNCs, bone marrow mononuclear cells
- BMT, bone marrow cell transplantation
- BOOST, Bone Marrow Transfer to Enhance ST Elevation Infarct Regeneration
- FACS, fluorescence-activated cell sorter
- FITC, fluorescein isothiocyanate
- LVDd, left ventricular end diastolic internal diameter
- LVEF, left ventricular ejection fraction
- PCI, percutaneous coronary intervention
- SPECT, single-photon emission computed tomography
- TCT-STAMI, Emergent Transcatheter Transplantation of Stem Cells for Treatment of Acute Myocardial Infarction
- VEGF, vascular endothelial growth factor
Statistics from Altmetric.com
- AMI, acute myocardial infarction
- BMCs, bond marrow stem cells
- BM-MNCs, bone marrow mononuclear cells
- BMT, bone marrow cell transplantation
- BOOST, Bone Marrow Transfer to Enhance ST Elevation Infarct Regeneration
- FACS, fluorescence-activated cell sorter
- FITC, fluorescein isothiocyanate
- LVDd, left ventricular end diastolic internal diameter
- LVEF, left ventricular ejection fraction
- PCI, percutaneous coronary intervention
- SPECT, single-photon emission computed tomography
- TCT-STAMI, Emergent Transcatheter Transplantation of Stem Cells for Treatment of Acute Myocardial Infarction
- VEGF, vascular endothelial growth factor
A growing body of evidence has shown that transplantation of bone marrow stem cells (BMCs) is a useful treatment of experimental acute myocardial infarction (AMI), by which the infarcted heart may be regenerated through increased myogenesis and angiogenesis, leading to improved cardiac function.1–5 Early clinical investigations also indicate that infusion of autologous BMCs into the infarct-related coronary artery can enhance cardiac function in patients with AMI.6–8 However, as Wollert et al8 noted, these studies were not randomised trials,8 and the role of bone marrow cell transplantation (BMT) in the treatment of patients with AMI remains to be clarified. Recently, Wollert et al8 reported a randomised clinical study (BOOST: Bone Marrow Transfer to Enhance ST Elevation Infarct Regeneration) showing the beneficial effects of BMT in patients with AMI.
Most patients with AMI can receive emergent percutaneous coronary intervention (PCI) within 24 h after onset of AMI. However, in early clinical studies such as BOOST, BMT was performed several days after AMI. It is therefore necessary to ask whether intracoronary BMT can be safely and effectively used in patients immediately after primary PCI to avoid a repeat PCI several days later, as this approach would be more cost effective. We therefore designed this double-blind, randomised clinical trial. In our present study, patients received intracoronary BMT or bone marrow supernatant transfer in the infarct-related artery immediately after successful PCI. The primary end point was left ventricular ejection fraction (LVEF), left ventricular end diastolic internal diameter (LVDd) and myocardial perfusion defect score changes from one week to six months after AMI.
METHODS
Patients, randomisation and study protocol
Only patients who were admitted within 24 h after the onset of symptoms of a first ST segment elevation myocardial infarction and had successfully undergone PCI with stent implantation in the infarct-related artery were included in this study. We excluded those with cardiogenic shock, cardioversion, bleeding, leucopenia, thrombocytopenia, hepatic or renal failure, documented terminal illness, HIV, hepatitis or cancer. Eligible patients (n = 20) were randomly allocated at a 1:1 ratio to either the control or BMT group with use of sequentially numbered, sealed envelopes. After successful PCI with stent implantation, bone marrow (∼40 ml) was collected immediately under local anaesthesia from the posterior superior iliac spine of all study patients. Two to three hours after BMC collection, patients received a 15 ml injection of either bone marrow supernatant (control group) or cell suspension containing about 4 × 107 bone marrow mononuclear cells (BM-MNCs) (BMT group) into the infarct-related artery as described previously.6 The appearance of BM-MNCs suspended in cold heparinised saline and of bone marrow supernatant mixed with heparinised saline was similar. After transplantation, coronary angiography was performed to ascertain vessel patency. All patients received standard drugs, including aspirin (100 mg daily), clopidogrel (300 mg loading dose, then 75 mg daily for one month after PCI), an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, a β blocker and a statin, unless these agents were contraindicated.
This TCT-STAMI (Emergent Transcatheter Transplantation of Stem Cells for Treatment of Acute Myocardial Infarction) study was approved by our local ethics committee. Patients provided written informed consent. Clinical data were acquired and analysed in a blinded fashion by clinicians who were blinded to the groups’ identities.
Preparation and characterisation of BMCs
BM-MNCs in the BMT group were prepared by Ficoll-Hypaque gradient centrifugation (Lymphoprep; Axis-Shield PoC, Oslo, Norway).9 BM-MNCs were suspended in 16 ml cold heparinised saline at a density of 2.42 (1.35) × 106 cells/ml and kept on ice before transplantation. An equal volume of bone marrow supernatant mixed with heparinised saline was used for patients in the control group. To ensure that a certain percentage of stem cells were present in the infused mononuclear cells, 1 ml BM-MNCs was analysed by fluorescence-activated cell sorter (FACS) after incubation with anti-human monoclonal antibodies: anti-human CD34 (CALTAG Laboratories, Burlingame, California, USA and Coulter Comp) or CD133 (Miltenyi Biotec) antibodies conjugated with fluorescein isothiocyanate (FITC). An FITC-conjugated isotopic serum was used as the isotype control. FACS analysis showed that BM-MNCs were 4.7% positive for CD34 and 0.79% positive for CD133.
Follow up
At one week and six months after AMI, patients were assessed for clinical status and current drugs and were examined by 24 h Holter recording, echocardiography and single-photon emission computed tomography (SPECT).
Echocardiography
Transthoracic echocardiography was performed on all study patients with a Vivid 7 ultrasound system (GE). Two-dimensional images were obtained at mid-papillary and apical levels. LVDd was measured by the biplane area–length method. LVEF (%) was calculated according to the modified Simpson’s method: LVEF (%) = EDV − ESV/EDV × 100%, where EDV is end diastolic volume and ESV is end systolic volume. All measurements were averaged for three consecutive cardiac cycles and were made by an experienced technician who was blinded to group identity.
SPECT
All patients were evaluated by stress-redistribution thallium-201 SPECT (IRIX SPECT, Philips). We recorded SPECT scans after intravenous injection of 10 × 107 Bq 201Tl-chloride. SPECT images were assessed by quantitative measurements of the activity in the area at risk (Philips Medical Systems, Milpitas, California, USA). SPECT images can be expressed as 17 involved segments with the use of quantitative gated SPECT software as described by Matsumoto et al.10 The extent of myocardial perfusion defect was graded as follows: normal uptake, 0; mildly or equivocally reduced, 1; moderately reduced, 2; severely reduced, 3; or absent uptake, 4. All defect scores were graded by two independent observers. Interobserver variation was < 5%.
Statistical evaluation
Data are presented as mean (SD). To test for differences between the control and BMT groups, an unpaired Student’s t test was used. To test for significant changes of variables from one week to six months after AMI within each study group, a paired Student’s t test was used. Significance was assumed at p < 0.05.
RESULTS
Baseline clinical characteristics
The final cohort in our study comprised 10 controls and 10 patients in the BMT group. Baseline clinical characteristics of the study patients did not differ significantly between the two groups (table 1). Mean time from onset of AMI to BMT was within 12 h. Mean time from PCI to BMT was within 3 h.
Baseline characteristics
Adverse events
No patients had a bleeding complication at the bone marrow puncture site. No angina aggravation, malignant diseases and substantial arrhythmias were found after PCI and intracoronary BMT or bone marrow supernatant transfer either in hospital or during follow up. All study patients are alive now.
Left ventricular function and geometry
LVEF and LVDd did not differ significantly at one week after AMI between the two groups (fig 1). Six months later, however, compared with the marginal changes in the control group (fig 1A), LVEF in the BMT group was significantly increased from 53.8 (9.2)% to 58.6 (9.9)% (p < 0.05; fig 1B). LVDd increased after six months in the control group (50.4 (6.0) mm at one week v 55.2 (7.1) mm at six months, p < 0.01; fig 1C) but was unchanged in the BMT group (fig 1D). These results suggest that BMT in our study improved cardiac function and prevented myocardial remodelling after AMI.

Echocardiographic analysis one week and six months after acute myocardial infarction (AMI) of left ventricular ejection fraction (LVEF) in (A) the control group and (B) the bone marrow cell transplant (BMT) group, and left ventricular end diastolic internal diameter (LVDd) in (C) the control group and (D) the BMT group. *p < 0.05 v one week in the same group.
Myocardial perfusion
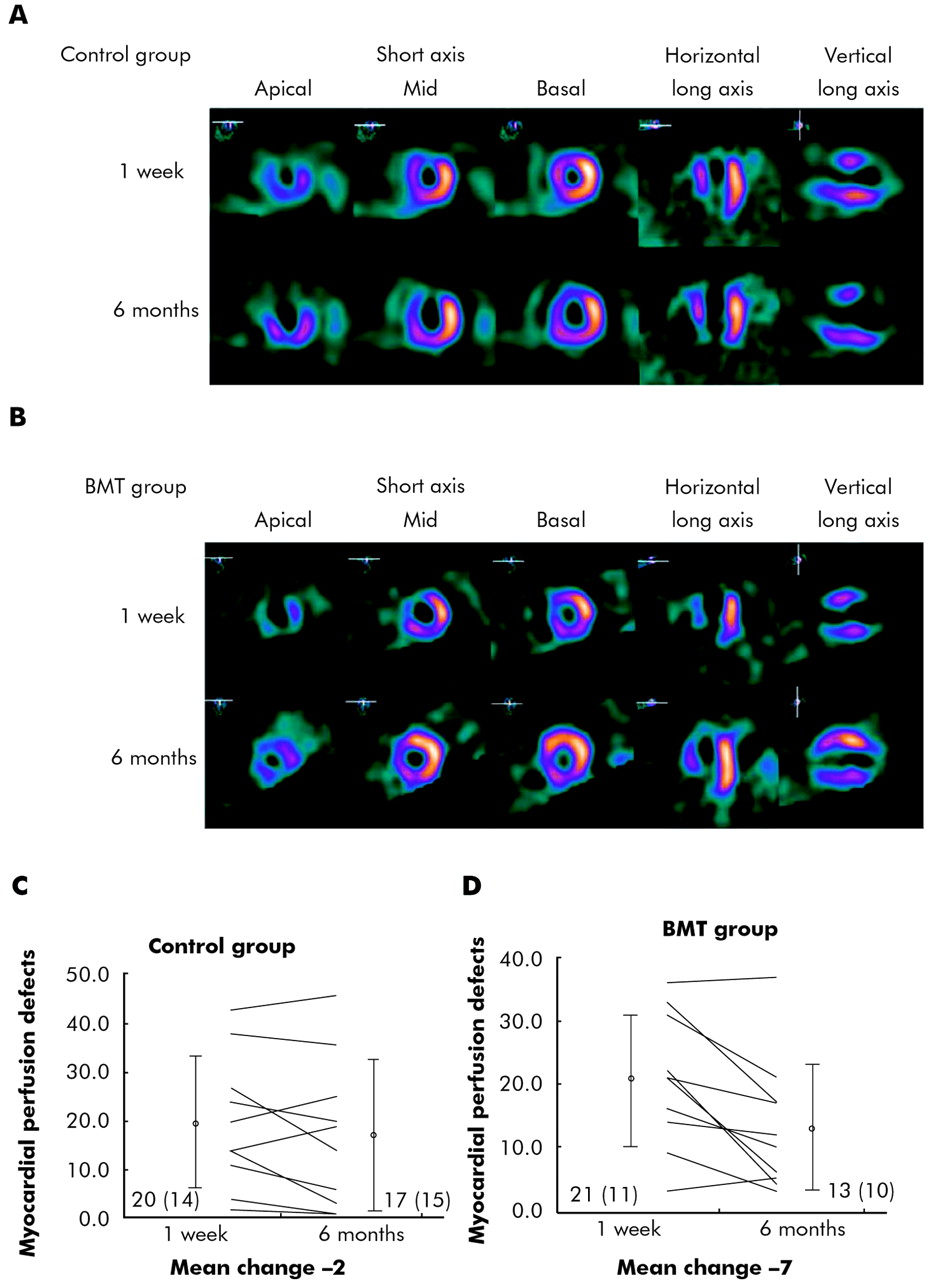
SPECT was used to assess myocardial perfusion. Figure 2A,B shows representative SPECT images of a control and a BMT group patient, respectively, at one week and six months after AMI. The myocardial perfusion defect in the control patient was similar and the left ventricular chamber was enlarged from one week to six months after AMI (fig 2A), whereas myocardial perfusion was improved and the ventricular chamber remained unchanged in the BMT patient from one week to six months (fig 2B). Semiquantitative analysis showed that myocardial perfusion defect scores remained unchanged in the control group (fig 2C) but decreased significantly in the BMT group from one week to six months (fig 2D).
{kind=link}
{kind=link}
Myocardial perfusion defect scores. Representative single-photon emission computed tomograms from (A) a control patient and (B) a bone marrow cell transplant (BMT) patient one week and six months after acute myocardial infraction (AMI). Semiquantitative analysis of myocardial perfusion defect scores in the (C) control and (D) BMT groups at one week and six months after AMI.
DISCUSSION
The present double-blind, randomised clinical trial showed that emergent intracoronary infusion of autologous BM-MNCs into the infarct-related coronary artery after successful PCI is safe and effective for the treatment of AMI.
In a previous randomised study, Wollert et al8 showed that intracoronary transplantation of autologous bone marrow cells during the early postinfarction period (within 4–8 days after symptom onset) improved global LVEF. Our data show that emergent intracoronary infusion of BM-MNCs into the infarct-related coronary artery is also effective for global left ventricular functional improvement in patients with AMI. Moreover, emergent autologous bone marrow cell transfer does not increase the risk of adverse clinical events. Our study was not designed to assess the underlying mechanisms of treatment with autologous bone marrow cells after AMI; however, our previous study in a rat model indicated that BMT immediately after AMI upregulated the expression of cytoprotective proteins, such as heat shock proteins 70 and 32 and blood vascular endothelial growth factor (VEGF).5 Heba et al11 found that the expression of VEGF was upregulated between one and four days after AMI. We speculated that these factors may be responsible for the beneficial effects of BMT on the infarcted hearts.
Global LVEF and myocardial perfusion defect scores remained unchanged and LVDd increased from 50.4 (6.0) mm at one week to 55.2 (7.1) mm at six months after AMI in the control group, indicating that the PCI strategy alone has a limited role in cardiac function recovery in these patients. However, BMT in combination with PCI significantly increased LVEF, decreased myocardial perfusion defect scores and attenuated LVDd enlargement from one week to six months after AMI, showing that addition of BMT to PCI may be a suitable strategy for cardiac functional recovery and for retarding left ventricular remodelling in patients with AMI.
One important limitation of the present study is that only 10 patients were enrolled in each group. The randomising process did not provide ideally matched baseline LVEF: baseline LVEF was slightly higher in the control group than in the BMT group (p > 0.05), which might have limited the capacity for further improvement in the control group. While our manuscript was in preparation, Janssens and colleagues12 published a randomised, double-blind, placebo-controlled study of 67 patients with significant left ventricular dysfunction. Bone marrow was harvested one day after successful PCI for ST elevation myocardial infarction. In their study, intracoronary transfer of autologous bone marrow cells one day after optimum reperfusion therapy did not augment recovery of global left ventricular function (LVEF 46.9% to 49.1% in the control group and 48.5% to 51.8% in the BMC group from baseline to four months) after myocardial infarction; however, a favourable impact on infarct remodelling was observed and patients with larger myocardial infarctions had a greater increase in metabolic activity after cell transfer than after placebo infusion.12 Our and other data indicate that future stem cell transfer studies in a larger patient population and in patients with more profound left ventricular dysfunction are warranted.
In conclusion, our results showed that emergent intracoronary transplantation of BM-MNCs to infarct-related coronary arteries is safe. Global left ventricular function and myocardial perfusion were improved, and the left ventricular remodelling process was attenuated in patients six months after AMI.
REFERENCES
Footnotes
-
Published Online First 14 June 2006
-
This work was supported by the Shanghai Scientific Research Fund (03XD).