Article Text

Abstract
Objective: To determine the safety and diagnostic accuracy of adenosine-stress cardiac magnetic resonance (CMR) perfusion imaging early after acute ST elevation myocardial infarction (STEMI) compared with standard exercise tolerance testing (ETT).
Design and setting: Cross sectional observational study in a university teaching hospital.
Patients: 35 patients admitted with first acute STEMI.
Interventions: All patients underwent a CMR imaging protocol which included rest and adenosine-stress perfusion, viability, and cardiac functional assessment. All patients also had an ETT (modified Bruce protocol) and x ray coronary angiography.
Main outcome measures: Safety and diagnostic accuracy of adenosine-stress perfusion CMR vs ETT early after STEMI in identifying patients with significant coronary stenosis (⩾70%) and the need for coronary revascularisation. Also, to determine if CMR can distinguish between ischaemia in the peri-infarct zone and ischaemia in remote myocardium.
Results: CMR imaging was well tolerated (all patients completed the protocol) and no complications occurred. CMR was more sensitive (86% vs 48%, p = 0.0074) and more specific than ETT (100% vs 50%, p<0.0001) for detecting significant coronary stenosis, and more sensitive for predicting revascularisation (94% vs 56%, p = 0.039). Inducible ischaemia in the infarct related artery territory was seen in 21 of 35 patients and was associated with smaller infarct size and less transmurality of infarction.
Conclusions: Adenosine-stress CMR imaging is safe early after acute STEMI and identifies patients with significant coronary stenosis more accurately than ETT.
- magnetic resonance imaging
- myocardial infarction
- coronary heart disease
- myocardial perfusion
- myocardial ischaemia
Statistics from Altmetric.com
- magnetic resonance imaging
- myocardial infarction
- coronary heart disease
- myocardial perfusion
- myocardial ischaemia
Despite the evidence in favour of primary percutaneous coronary intervention, the majority of patients presenting with acute ST segment elevation myocardial infarction (STEMI) are still treated with intravenous thrombolysis.1 2 Because of the relatively high incidence of failed reperfusion and the occurrence of reocclusion, guidelines recommend that following intravenous thrombolysis for STEMI patients with high risk features (such as an ejection fraction less than 0.40, recurrent ischaemia, presence of shock or severe pulmonary congestion) should undergo in-hospital cardiac catheterisation.3–7 Other patients should have an exercise tolerance test (ETT) in the hospital or early after discharge to assess the presence and extent of inducible ischaemia (class 1 evidence), or a stress imaging study if baseline ECG abnormalities compromise interpretation of the ETT.7 However, although widely available and cost-effective, ETT has important and well known limitations in terms of diagnostic accuracy.8–10
Cardiac magnetic resonance (CMR) imaging is becoming increasingly available for the assessment of patients with coronary artery disease. CMR allows a simultaneous assessment of myocardial perfusion, function, and scar at high spatial resolution.11–13 In patients with recent STEMI, late gadolinium enhanced CMR imaging already provides detailed information about the extent of the myocardial scar as a guide to revascularisation, and has been shown to predict future cardiovascular events.14 15 Adding a stress perfusion study to the CMR assessment of the scar may provide an accurate tool for detecting patients with significant coronary stenosis and predict the need for revascularisation after STEMI. In addition, the high spatial resolution of CMR should allow the localisation of ischaemia to the infarct related artery (IRA) or to other coronary arteries. However, the use of stress CMR imaging early after STEMI has not been reported previously.
The main aim of this study was to evaluate whether CMR stress perfusion imaging is safe early after STEMI. As secondary objectives we aimed to determine the diagnostic accuracy of CMR vs ETT for identifying significant coronary stenosis, the diagnostic accuracy of CMR vs ETT for identifying the need for revascularisation, and whether CMR can distinguish between ischaemia in the peri-infarct zone and ischaemia in remote myocardium.
METHODS
Subjects
We studied 35 patients (31 male, 4 female; mean 55 years, range 36 to 74 years). They presented with a first acute STEMI and met the traditional World Health Organisation (WHO) criteria for acute myocardial infarction, which include chest pain lasting more than 20 minutes, ST segment elevation >1 mm in two or more contiguous leads, or new left bundle branch block on a 12-lead ECG. Table 1 summarises the demographic information on the patients.
All patients had a CMR study during the index admission and an ETT while in hospital or in the early post-discharge period. They were eligible for inclusion in the study if they also underwent clinically indicated cardiac catheterisation after CMR and ETT. Exclusion criteria were a previous history of acute coronary syndrome, coronary revascularisation, New York Heart Association class IV congestive heart failure, haemodynamic instability, contraindication to CMR imaging (claustrophobia, non-compatible metallic implants), or adenosine infusion (second or third degree atrioventricular block, history of asthma or bronchospasm). A TIMI risk score and Killip class were calculated for all patients.17 The study complied with the Declaration of Helsinki, was approved by the local ethics committee, and all subjects gave their informed written consent.
CMR imaging
CMR imaging was carried out during the index admission two to eight days (mean (SD), 3.7 (1.4)) after presentation and before x ray coronary angiography. A 1.5 Tesla clinical CMR system was used for all studies (Philips Medical Systems, Best, Netherlands), which was equipped with ‘Master’ gradients (30 mT/m amplitude, 150 mT/s slew rate) and a five element cardiac phased array receiver coil. Any substances containing caffeine were withheld for 12 hours before the study.
A previously reported CMR protocol was used.13 All data were acquired in identical parallel imaging planes aligned in the left ventricular short axis.
Perfusion imaging
First pass myocardial perfusion imaging was carried out in four parallel short axis slices at rest and during a five minute adenosine infusion (140 μg/kg/min). A bolus of 0.05 mmol/kg dimeglumine gadopentetate was given at 6 ml/s by power injector (Spectris, Medrad, Pittsburgh, PA, USA) for each perfusion study and a T1 weighted saturation recovery segmented k-space gradient echo pulse sequence combined with sensitivity encoding (SENSE) was used for data acquisition (echo time 1.6 ms; repetition time 3.3 ms; flip angle 15°, SENSE factor 2, matrix 160×112 reconstructed to 256×256, in plane spatial resolution 3×3 mm). Data were acquired for 40 seconds and at every heart beat.
Cine imaging
Cine images in 10 to 12 slices were acquired with a steady state free precession pulse sequence (echo time 1.4 ms; repetition time 2.8 ms; flip angle 55°, in-plane spatial resolution 2×2 mm).
Late gadolinium enhanced imaging
An additional bolus of 0.1 mmol/kg of contrast agent was given immediately after the second perfusion study to achieve a total of dose 0.2 mmol/kg for optimal late gadolinium enhanced imaging. Acquisition in 10 to 12 slices used an inversion recovery segmented k-space gradient echo pulse sequence (echo time 3.8 ms; repetition time 7.5 ms; flip angle 15°, inversion time set to null signal from normal myocardium, spatial resolution 1.2×1.2 mm).
Safety
To maximise patient safety, a physician was present in the CMR department throughout the scan. Heart rate and a vector cardiogram were monitored continuously. Blood pressure was monitored at the beginning of the study and every two minutes during the perfusion measurements. Patients were removed from the magnet bore for the first three to four minutes of the adenosine infusion to improve ECG monitoring and patient access. The physician remained in the magnet room for the duration of the stress infusion.
CMR analysis
Visual analysis of the CMR perfusion and viability images was done off-line by consensus of two experienced observers using commercial software (Mass 5.0, Medis, Netherlands). Rest and stress perfusion and the late gadolinium enhancement images were viewed side by side. If the signal intensity on stress perfusion appeared lower in an area of myocardium for at least three dynamic images compared with remote myocardium, it was considered to be ischaemic.18 If non-transmural infarction was seen on scar images with a stress perfusion defect extending transmurally or outside of the scar, ischaemia in the IRA territory was reported. Ischaemia in myocardium remote from the infarct was recorded separately. If the same signal intensity abnormality was seen in the rest and stress perfusion images and there was no evidence of scar on late contrast enhanced images, the defect was considered an artefact.19
Left ventricular mass and volumes were calculated by drawing the endocardial and epicardial contours on the end diastolic and end systolic images of the cine data sets and applying the modified Simpson’s rule. On late gadolinium enhanced images regions of interest were drawn around the hyperenhanced tissue in each of the left ventricular short axis slices and the volume of infarcted tissue calculated. Infarct volume was multiplied by 1.05 (myocardial density) so as to calculate the mass of infarcted tissue in grams. The transmurality of scar was graded as 0%, 1–25%, 26–50%, 51–75%, and 76–100% for 17 myocardial segments according to American Heart Association segmentation criteria.20
Exercise tolerance tests
Exercise tolerance tests were carried out either during the index admission (n = 25) or in the early post-discharge period (n = 10). A standard modified Bruce protocol was used and the test reported by a cardiologist. The test was considered positive if any one of the following occurred: symptomatic ST segment depression (or additional elevation) of ⩾1 mm, fall in systolic blood pressure during exercise, <5 METS workload.
x Ray angiography
Cardiac catheterisation was carried out during the index admission (n = 19) or after discharge from hospital (n = 16). All x ray angiograms were undertaken after the CMR and ETT using a standard technique21 and were reported by a single, blinded interventional cardiologist. The presence of one or more coronary stenoses of ⩾70% luminal narrowing in a main coronary vessel or major side branch of >2 mm diameter was reported as representing significant coronary artery disease. Any requirement for revascularisation was determined as per routine clinical practice by the interventional cardiologist, without knowledge of the CMR study.
Statistics
Results are presented as mean (SD). The diagnostic accuracy in terms of sensitivity, specificity, and positive and negative predictive values of CMR and ETT for detecting a significant coronary stenosis (⩾70%) on x ray angiography and for predicting the need for revascularisation was determined. Comparisons between ETT and CMR for predicting the presence of coronary stenosis were made using a McNemar’s test. Comparisons between continuous variables were made using t tests. Ordinal parameters were compared with a Mann–Whitney U test. All tests were two sided. A probability (p) value <0.05 was considered significant.
RESULTS
Safety
All 35 patients completed the CMR study, which was undertaken at a mean of 3.7 (1.4) days post-infarction. During adenosine stress CMR perfusion, 22 patients (63%) reported mild symptoms of flushing, breathlessness, or chest discomfort. Thirty three of the patients were on β blockers at the time of the CMR study, but heart block or other significant complications were not observed. Mean resting heart rate was 61.7 (10.2) beats/min at rest and increased to 72.3 (11.4) beats/min during the adenosine stress. Mean systolic blood pressure was 110.2 (15.9) mm Hg at rest and increased to 114.6 (16.9) mm Hg on stress. No clinical events occurred in any patient between the three investigations of CMR, ETT, and x ray angiography, and all patients completed all three tests.
Clinical markers
Twenty eight patients were treated with intravenous thrombolysis (17 with an accelerated alteplase regime, 11 with streptokinase). The reasons for not using thrombolysis in the remaining seven patients were: presentation more than 12 hours after pain onset (n = 3), and clinical judgment against thrombolysis for other medical reasons (n = 4). Infarct location was inferior/posterior in 18 patients, anterior/septal in 12, and lateral in five. All patients had a significant creatine kinase (CK) rise to more than twice the upper limit of the normal range in our institution. The mean peak CK rise in all patients was 1677 (1214) IU (range 262 to 5288). The mean Killip class was 1.1 (0.4), with 31 patients in Killip class 1, three in Killip class 2, and one in Killip class 3. The mean TIMI risk score was 2.3 (1.6), with eight patients having a TIMI score of greater than 3.
x Ray angiography
Twenty nine of 35 patients had evidence of coronary stenosis of ⩾70% on x ray coronary angiography. In seven patients, significant coronary stenosis in more than one first order coronary artery was seen. Eighteen patients underwent percutaneous coronary intervention. Reasons for not carrying out percutaneous intervention in the remaining 11 patients with significant coronary stenosis were: angiographic appearance of total occlusion with presumed completed infarction (n = 4), distal lesions unsuitable for percutaneous intervention (n = 3), and diffuse coronary disease requiring bypass surgery (n = 4).
CMR imaging
Mean ejection fraction as measured by CMR was 45.6 (7.4)%, and eight patients had a value less than 40%. All 35 patients had evidence of infarction from the late gadolinium enhanced CMR images, and the mean infarct size measured was 23.0 (16.5) g or 18.9 (12.4)% of the left ventricle when normalised to left ventricular mass. Infarct size was greater in patients with evidence of transmural infarction (>75%) in any myocardial segment than in those whose infarct transmurality was less than 75% in all segments (30.8 (15.0) vs 8.8 (6.8) g, p<0.0001).
On the perfusion CMR images, inducible ischaemia in the IRA territory was seen in 21 of 35 patients. In all seven patients with multivessel coronary disease, ischaemia in remote myocardium was demonstrated on CMR. In all six patients without significant coronary disease on x ray angiography, no inducible ischaemia was demonstrated on CMR perfusion imaging.
In patients in whom CMR showed inducible ischaemia in the IRA territory, the infarct size was smaller than in those with no ischaemia in the IRA territory (16.8 (12.7) vs 31.3 (16.8) g, p = 0.008). Patients with inducible ischaemia in the IRA territory also had less transmural infarction, with a mean of 1.0 (1.2) segments showing transmural infarction compared with 2.6 (2.0) segments in patients with no ischaemia in the IRA territory (p = 0.0047). Conversely, 18 of 25 patients with two or fewer segments showing transmural infarction had inducible ischaemia in the IRA territory, while only three of 10 patients with transmural infarction in more than two segments showed evidence of inducible ischaemia in the IRA territory.
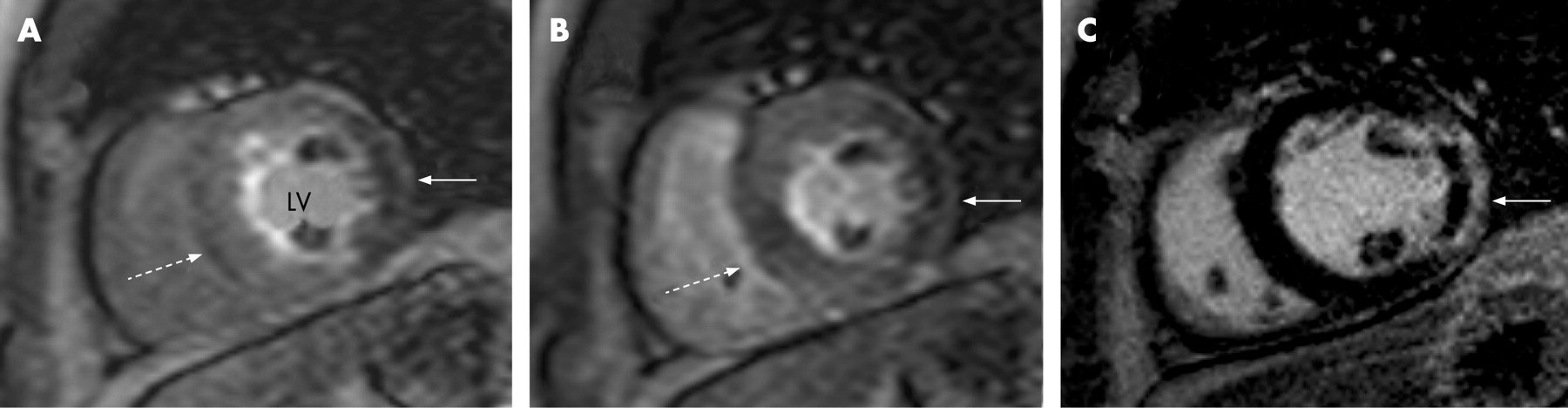
Two case examples are shown in figs 1 and 2. In fig 1, CMR scar imaging was normal and stress perfusion imaging identified a very large anterior perfusion defect. Subsequent x ray angiography demonstrated a high grade lesion in the proximal left anterior descending coronary artery (LAD). In fig 2, a transmural infarct in the lateral wall can be seen with inducible ischaemia in the septum. x Ray angiography showed significant disease in the LAD and circumflex arteries.


{kind=link}
{kind=link}
Diagnostic accuracy
Table 2 highlights the main results for diagnostic accuracy of CMR perfusion analysis and ETT. CMR was significantly more sensitive (86%) than ETT (48%) in predicting coronary stenosis of ⩾70% on x ray coronary angiography (p = 0.0074). The specificity of CMR was 100% and for ETT 50% (p<0.0001), but only six patients had no angiographic evidence of significant coronary stenosis. CMR was also more sensitive in predicting the need for revascularisation (94% vs 56%, p = 0.039), while specificities for this end point were similar for CMR and ETT (59% vs 53%, NS).
DISCUSSION
This study showed that stress myocardial perfusion CMR imaging can be undertaken safely early after STEMI. Furthermore, the sensitivity of CMR perfusion analysis for detecting significant coronary stenosis and predicting revascularisation was superior to ETT in this study.
Previous studies have shown the feasibility of adenosine stress CMR imaging in patients with chest pain where acute myocardial infarction was excluded, as well as in patients with non-ST-elevation acute coronary syndromes.18 19 The present study is the first to report vasodilator stress CMR imaging early after STEMI. Serious complications from adenosine are rare, and nuclear scintigraphy studies have shown that vasodilator stress imaging is safe two to four days after STEMI.22–25 However, in the magnetic resonance environment the limited patient access and electromagnetic interference with the ECG pose additional challenges for pharmacological stress imaging. For this study we therefore defined clear safety procedures. Patients were supervised by a physician in the magnet room and haemodynamic indices were monitored regularly. Removing patients from the magnet bore during the adenosine infusion proved an effective method of improving interaction with the patient during this critical part of the scan. This approach would also have allowed a more rapid response to any complications. With these procedures in place, adenosine was well tolerated by the majority of patients in our study with recent STEMI, and no complications occurred. Therefore this study adds to the growing evidence that stress CMR imaging can be safely undertaken in all forms of acute coronary syndromes.
Current guidelines recommend that following medically treated STEMI, patients at high risk of future cardiovascular events should undergo early cardiac catheterisation. For prognostic assessment of low risk patients, ETT is still recommended (class I evidence).7 Either nuclear scintigraphy or stress echocardiography are recommended to look for inducible ischaemia in patients judged to be unable to exercise (class I evidence) or to assess myocardial viability when required to define the potential efficacy of revascularisation (class IIa evidence).7 Furthermore, the measurement of infarct size by nuclear scintigraphy has been shown to be significantly associated with subsequent patient mortality after fibrinolytic therapy.26
CMR, as an emerging imaging technique for coronary artery disease, is poised to play an important future role in both risk stratification and clinical management after STEMI. CMR has the potential to provide a more accurate assessment than currently available tests because of its superior spatial resolution. Late gadolinium enhanced CMR imaging already allows the most precise estimate of infarct size of any imaging method currently available. In particular it has been shown to be more accurate than nuclear scintigraphy in detecting subendocardial infarction.27 Importantly, several recent studies have also shown that abnormalities on CMR, such as the transmurality of late contrast enhancement or the presence of microvascular obstruction, can predict adverse clinical events following STEMI.14 15 The present study adds to these existing data by showing that CMR can also be used for accurate detection of the presence of significant coronary stenosis after STEMI, and to predict the need for revascularisation. Compared with the currently recommended and widely used ETT for ischaemia detection, CMR was significantly more sensitive for both of these end points. In addition, CMR was able to differentiate between myocardial ischaemia in the IRA territory and in remote myocardium. In all patients with multivessel coronary disease CMR demonstrated remote ischaemia outside the IRA. Because it is often difficult to localise ischaemia to coronary vessels on ETT, such information provided by CMR should be useful for patient management following STEMI. In addition, CMR data on myocardial scarring could become an important investigation to guide revascularisation decisions.
In this study we found that the majority of patients with recent STEMI had evidence of ischaemia in the IRA territory. However, IRA territory ischaemia was more likely if infarcts on CMR were smaller and predominantly non-transmural. Conversely, if more than two myocardial segments showed transmural infarction, IRA territory ischaemia was unlikely. These observations are biologically plausible because myocardium that has been reperfused before the infarction has become transmural remains at risk of further events and ischaemia. On the other hand, in a large transmural infarct the vast majority of myocardium supplied by the IRA is likely to be infarcted so that there is less potential for further ischaemia in this territory. These findings underline the potential clinical value of a combined assessment of perfusion and scar after STEMI with high resolution CMR imaging. However, future studies need to determine the prognostic implications of our initial observations and also the key issue whether a CMR study would justify the additional cost for risk stratification and guidance of revascularisation.
Limitations
Some x ray angiograms were carried out after discharge from hospital. This reflected clinical practice at our institution at the time, but should have little impact on our results as no clinical events occurred between the study investigations of CMR, ETT, and x ray angiography.
We did not compare CMR with SPECT or stress echocardiography. Those tests may provide better diagnostic accuracy than ETT alone and in addition provide viability information. However, all patients in this study were able to exercise and none had a baseline ECG that could have compromised the interpretation of an ETT. Our study was thus within the ACC/AHA guidelines for the management of patients after STEMI. Because of the small number of patients without significant coronary artery disease on x ray angiography, the specificity data obtained in this study are less robust.
Finally, the severity of coronary stenosis was estimated visually and we assumed that a stenosis of 70% produced a significant impairment of coronary flow, in line with routine clinical practice. Intracoronary pressure wire or intravascular ultrasound studies were not carried out.
CONCLUSIONS
Adenosine stress CMR perfusion is safe early after STEMI and is more sensitive than ETT for detecting significant coronary stenosis and predicting revascularisation. In a single imaging study CMR can provide data for both risk stratification and guidance on the potential efficacy of revascularisation. Larger studies in this patient group appear justified.
REFERENCES
Footnotes
Competing interests: None declared.
- Abbreviations:
- CMR
- cardiac magnetic resonance
- ETT
- exercise tolerance test
- IRA
- infarct related artery
- STEMI
- ST elevation myocardial infarction
- TIMI
- Thrombolysis in Myocardial Infarction trial