Article Text

Abstract
Objective To estimate the size and characteristics of the UK population with single-ventricle physiology, and predict future population growth.
Methods The surviving population with single-ventricle physiology in Northern England (resident population 2.9 million) was identified from our clinical database and the Northern Congenital Abnormality Survey (NorCAS). Conditions included double inlet ventricle, tricuspid atresia, mitral atresia, hypoplastic left heart syndrome and other unbalanced defects. Fetal diagnoses, terminations of pregnancy and surgical interventions were reviewed. Childhood and adult prevalence of single-ventricle physiology were calculated. Current and future National population figures were estimated using expected mortality derived from literature.
Results 80 children and 48 adults with single-ventricle physiology were identified in the NorCAS region. The most frequent underlying condition in childhood was hypoplastic left heart, and among adults was double inlet ventricle. All children over 5 years of age had completed a Fontan repair (89%) or had a Glenn anastomosis. Seven adults had not undergone a Glenn shunt or Fontan procedure. Of those patients over 30 years of age (n=12), 50% were New York Heart Association (NYHA) functional class 3, compared to 3% of those under 30 years (p=0.001). Regional childhood and adult prevalence of single-ventricle physiology was 16 and 2 per 100 000, respectively.
Conclusions The current UK single-ventricle population is composed of around 1040 adults and 1700 children. Adult numbers will increase by over 60% in the next decade with the proportion in NHYA functional class 3 set to double.
- CONGENITAL HEART DISEASE
Statistics from Altmetric.com
Introduction
Outcomes for patients born prior to 1990 with single-ventricle physiology have been relatively poor.1 ,2 However, remarkable advances in surgical technique and perioperative care for those undergoing Fontan surgery, mean that many patients now expect to survive and graduate to the adult clinics.2 ,3 The provision of care in adult life is challenging with most clinicians regarding deterioration in ventricular function and shortened life expectancy as inevitable.4 It is unclear whether standard antifailure therapies influence outcome and expectations with respect to transplantation and mechanical assist devices may be unrealistic. The clinical needs and service requirements of this growing population must be addressed, but this is difficult when the size and status of the population is unknown.5
The purpose of the present study is to determine the scale of the problem posed by the adult single-ventricle population currently and in the next decade.
Methods
We ascertained our current population of surviving patients with single-ventricle physiology, in a defined catchment area of North East England and North Cumbria served by a single congenital surgical referral centre. Those born before 1 January 1998, will all be 16 years old, or over, by the end of 2013 and, therefore, comprise our current regional adult population. Those born after 1 January 1998 comprise our current regional paediatric population. Those born between 1 January 1998 and 31 December 2007, in addition to the existing adult population, will be 16 years old, or over, by the end of 2023 and, therefore, will contribute to the adult population in a decade's time. Demographic and clinical data were determined from last clinical contact and collected in March 2013.
Sources of information
Individuals with single-ventricle physiology were identified from two sources.
-
The Northern Congenital Abnormality Survey (NorCAS) database has collected details of all infants born with structural congenital heart disease in North Cumbria, Northumberland, Newcastle upon Tyne, North Tyneside, Gateshead, South Tyneside, County Durham, Darlington and Tees (formerly known as the Northern Health Region) since January 1985.6 Additionally, the survey records fetal diagnoses and terminations of pregnancy for these conditions. Population statistics for this defined region are collected annually.
-
Our centre is, and has been, historically, the sole referral centre for babies born with single-ventricle physiology in the NorCAS region. The geographical location of the centre was different prior to 1978, but referral patterns have not changed and the patient population has moved on all occasions with the centre. The departmental database contains information, including birth location, of all individuals with congenital heart disease currently and previously followed at our centre, and was initiated at the same time point as NorCAS commenced. The database is maintained by a dedicated secretary and updated following each patient contact with healthcare services in our unit, and when information is received from elsewhere. All individuals with single-ventricle physiology followed at our centre were identified from this source, and from 1985 were cross-checked with the NorCAS data. If they had died or were born outside the NorCAS region they were excluded from the subsequent analysis. For subjects born prior to 1985, a cross-check was performed with current clinic attendance lists. It is accepted that of these older individuals, some may have moved away from the region prior to commencement of the departmental database and might still be alive. While this number is likely to be tiny, if existent, these individuals cannot be accounted for. Thus, absolute adult population numbers for the region and the UK, as well as the adult prevalence calculation, represent a minimum estimate.
The annual rate of Fontan surgery at our centre and nationally is available from the Central Cardiac Audit Database (CCAD) database maintained by National Institute for Cardiovascular Outcomes Research (NICOR).7
Definition of single ventricle in this study
The single-ventricle population was defined as those with the following diagnoses: double inlet ventricle (DIV); mitral atresia (MA); tricuspid atresia (TA) and hypoplastic left heart syndrome (HLHS). Unbalanced defects (such as atrioventricular septal defect or pulmonary atresia with intact septum) were included if the patient had undergone Glenn anastomosis or Fontan palliation.
Calculation of prevalence and national population
Livebirth prevalence of single-ventricle physiology was determined from the NorCAS registry using data available between 2003 and 2012. The number of cases of single-ventricle physiology, as described above, was divided by the total livebirths in the region during these years.
Paediatric prevalence of single-ventricle physiology was estimated by dividing the number of childhood cases, identified from the departmental database, by the resident paediatric population of the NorCAS region. The resident paediatric population was calculated by summing the livebirth rate over the period 1997–2012, and adjusting for infant and childhood mortality using nationally available statistics.8
Adult prevalence of single-ventricle physiology was estimated by dividing the number of adult cases, identified from the departmental database, by the resident adult population of the NorCAS region. The resident adult population was approximated by subtracting the calculated paediatric population from the resident population statistic in order to eliminate those under 16 years of age.
Knowing the relationship between the regional resident population and that of the UK, we were able to predict the national population of patients with single-ventricle physiology. Patients who migrated in or out of the region during the timeframe of the study were excluded from the analysis. The national population estimate is, therefore, designed to represent a figure that is at the low end of what may be expected.
Prediction of 10-year survival
Using assumptions based on literature, we estimated the likely growth in the adult single-ventricle population over the next decade. We assumed an annual mortality of 4.8% for the minority of adults with unrepaired or palliated single-ventricle physiology.9 We assumed a 10-year mortality of 10% for adults with Fontan repair based on data from the Boston cohort (n=261, operated between 1973 and 1991, mean age 7.9 years),3 and a 10-year mortality of 6% for children with Fontan repair based on data from the Wisconsin cohort (n=256, operated between 1994 and 2007, mean age 36.2 months).10
It was assumed that those with a Glenn shunt only would progress to Fontan surgery, which in the current era has low perioperative mortality, and would thus have comparable 10-year mortality.3
Statistical analysis
For simplification, local and national resident population and live birth statistics have been presented to the nearest 100 000 and nearest 1000, respectively. Prevalence has been reported per 100 000 cases. Age is expressed as median and range. Fisher's exact test was used for comparison of New York Heart Association (NYHA) functional class. Statistical analysis was performed using SPSS (V.19.0).
Results
The NorCAS region has a resident population of around 2.9 million (2012), approximately 4.6% of that of the UK (63.7 million, 2012). The mean annual live birth rate of the region is approximately 33 000 (data from 2003–2012) accounting for 4.3% of the live birth rate in the UK over the same period.11
Regional paediatric population
There are 80 children currently alive with single-ventricle physiology, who were born and remain resident in the NorCAS region (table 1 and figure 1). The predominant diagnoses are HLHS (n=20) and TA (n=19) with 53% (n=42) having undergone total cavo-pulmonary connection.
Current single-ventricle population demographics in the northern region

Current paediatric (n=80) and adult (n=48) population with single-ventricle physiology, born and resident in the Northern Congenital Abnormality Survey region, by diagnosis and age. DIV, double inlet ventricle, TA, tricuspid atresia, MA, mitral atresia, HLHS, hypoplastic left heart syndrome, Other, other unbalanced conditions with Glenn or Fontan repair.
Of those aged over 5 years (n=37), who in a decade's time will be adults, 89% (n=33) have undergone total cavo-pulmonary connection with the remainder having a Glenn shunt. Median age of total cavo-pulmonary connection in this group was 4 years (range 1–8).
Regional adult population
There are 48 adults currently alive with single-ventricle physiology that were born and remain resident in the NorCAS region (table 1 and figure 1). The predominant diagnoses are double inlet ventricle (n=17) and TA (n=16) with the majority (n=35) having undergone total cavo-pulmonary connection as the definitive repair strategy. Two patients who underwent total cavopulmonary connection, were converted from atriopulmonary Fontan. Median age of total cavopulmonary connection was 7 years (range 1–38) including those converted from atriopulmonary Fontan (n=2). Heart failure therapy was prescribed in 17 patients (diuretics: n=6; ACE inhibitors/ARBs: n=14). Six patients were prescribed β-blockers; of whom five had a history of arrhythmia, predominantly atrial. Three patients were treated with sildenafil. Five patients had pacemakers.
Twelve adults (25%) were older than 30 years of age. NYHA functional class was greater in those adults over the age of 30 years (p<0.001) despite no significant difference in heart failure treatment (p=0.3) or prevalence of arrhythmia (p=0.094). Of those in NYHA functional class 3 (n=7), five had TA, three had undergone total cavopulmonary connection, one had undergone atriopulmonary Fontan and five had either had or were awaiting transplant assessment. NYHA status could not be assessed in two patients due to non-cardiac limitations to mobility.
Rates of Fontan and Glenn surgery
Over the last decade, our centre has performed 4.5% and 5.0%, respectively, of the National caseload of Fontan and Glenn Surgery, which corresponds with the proportion of the population we serve (figure 2). There has been a slight increase in Fontan operations performed over time at our centre: it is difficult to identify a single reason, however, transplantation practise may have some influence. Nationally, mean 30-day mortality and 1-year mortality were 2.2% and 3.8% for Fontan surgery, and 1.8% and 4.0% for Glenn surgery, over this period of time. Approximately 5% of Fontan surgery and 1% of Glenn surgery were performed in adults (>16 years).

Rates of Fontan and Glenn Surgery in the UK and at the Freeman Hospital, Newcastle upon Tyne.
Transplantation
Between 1988 and 2013, 25 children (6 total cavopulmonary connection, 4 Glenn anastomosis) and 11 adults (2 total cavopulmonary connection, 2 atriopulmonary Fontan) from our region underwent transplantation at our centre for single-ventricle physiology. These patients are not included in current population statistics or future population modelling.
Fetal diagnoses and terminations of pregnancy
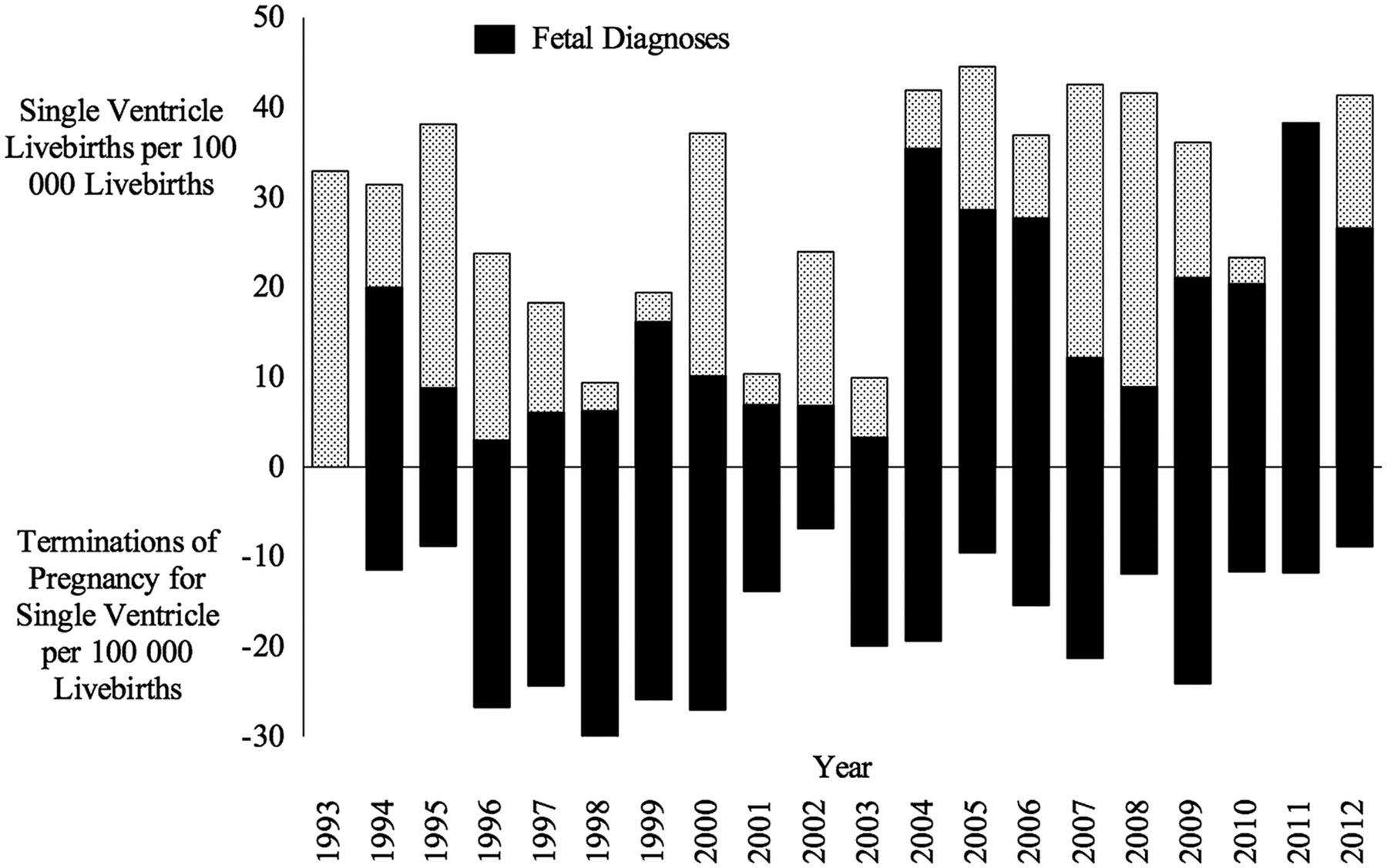
Fetal diagnoses of single-ventricle physiology increased in the NorCAS region in the mid-90s; this was mirrored by an increase in terminations of pregnancy (figure 3). Over the last decade, while the detection rate has been maintained, the relative proportion of terminations has fallen.
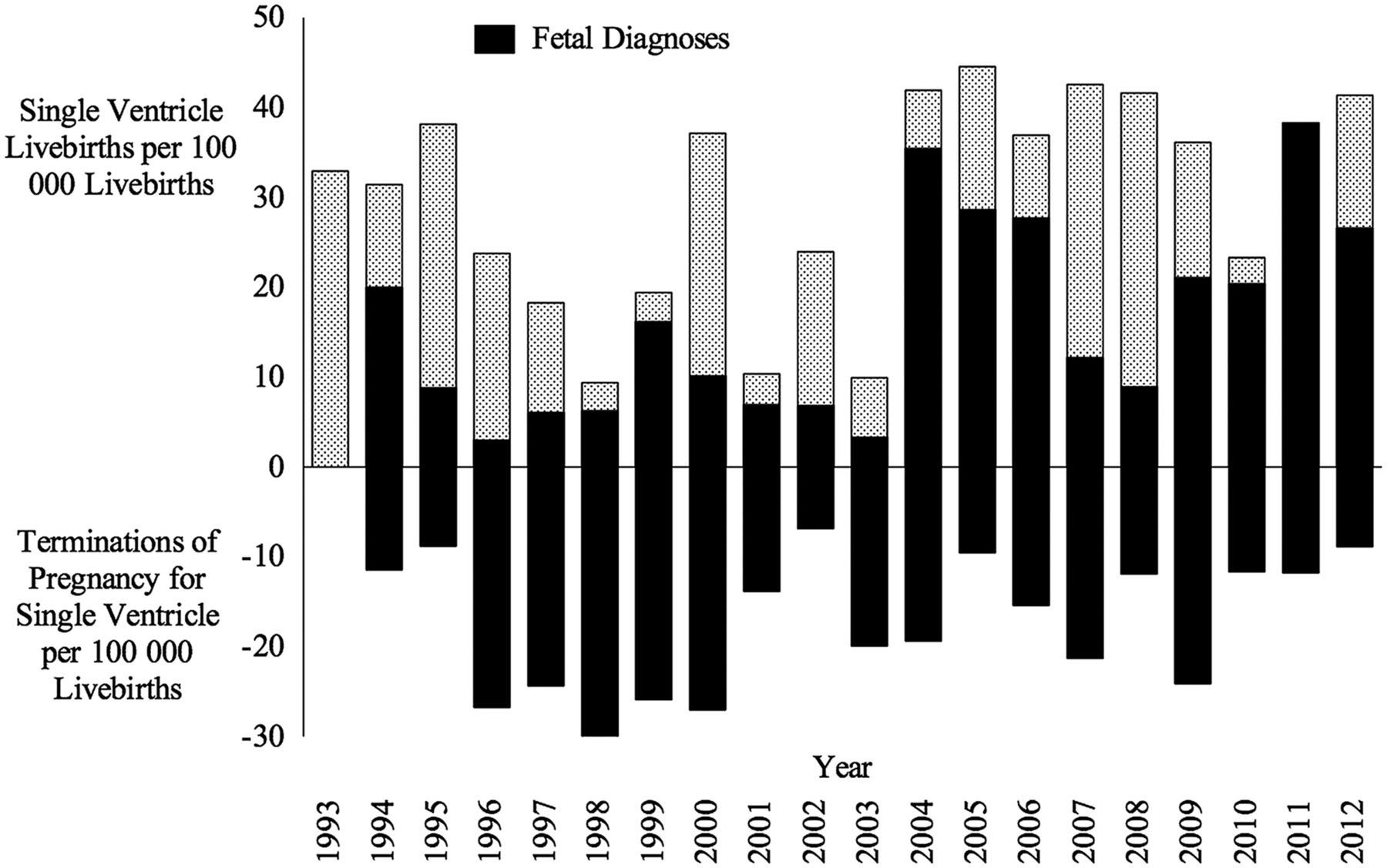
Annual livebirths and terminations of pregnancy for single-ventricle physiology in the Northern Congenital Abnormality Survey region standardised to annual regional livebirth rate.
Prevalence and estimated national population
The regional live birth prevalence of single-ventricle physiology was 31 per 100 000 live births, based on 101 babies born between 2003 and 2012 within the defined area. This comprised: HLHS (45%), DIV (12%), TA (19%), MA (6%) and other unbalanced defects (18%). This figure is likely to be a slight underestimation, as unbalanced defects were only included if the patient had undergone a Glenn anastomosis or Fontan repair.
The regional prevalence of single-ventricle physiology among the paediatric population was 16 per 100 000 children, and among the adult population was 2 per 100 000 adults. We estimate that there are currently just over 1700 children and 1040 similar adult patients with single-ventricle physiology in the UK.
Predicted growth in adult population over the next decade
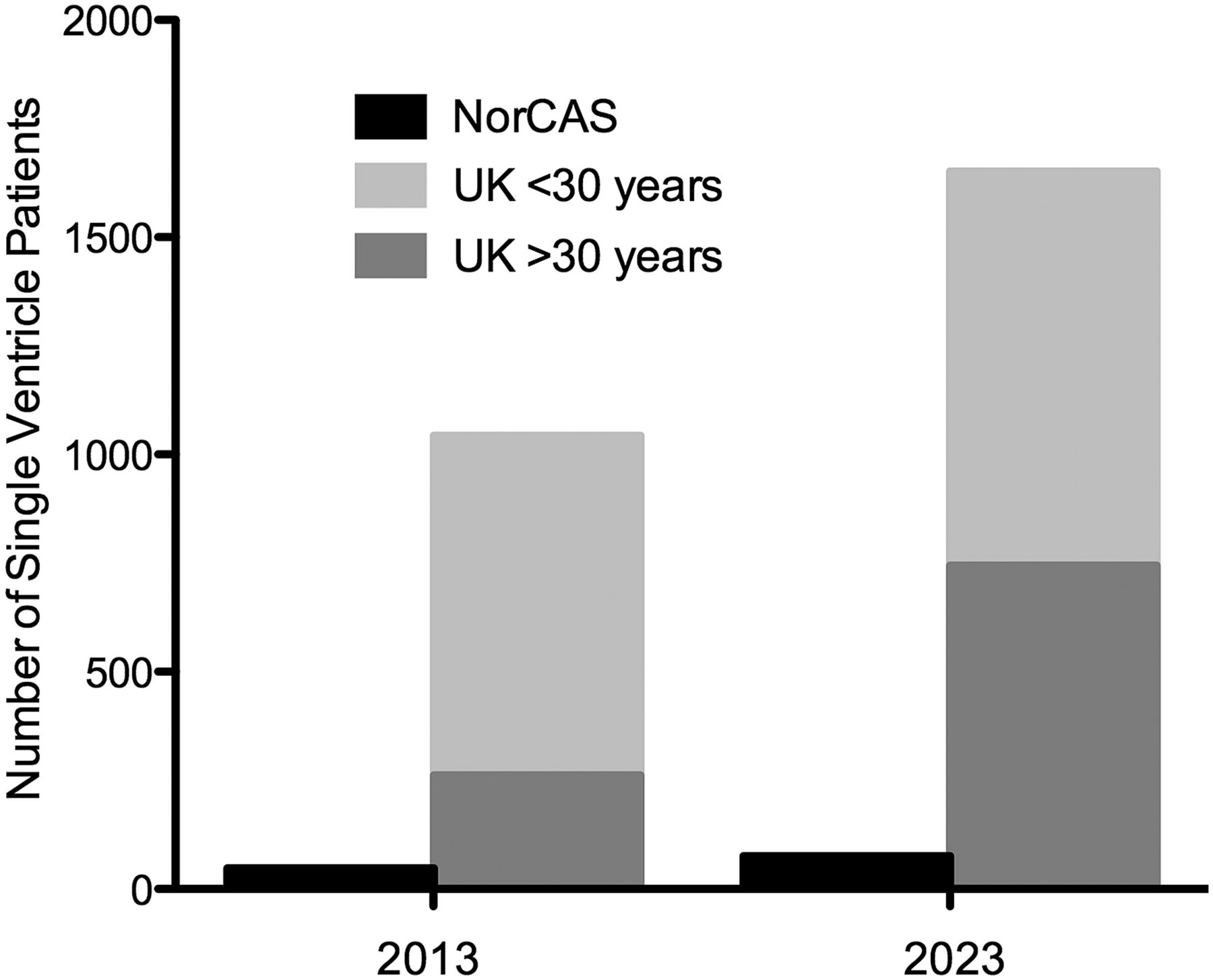
There are 37 paediatric patients currently aged between 6 years and 15 years, all with Fontan or Glenn repair, who in the next decade may add to the existing adult population. The current adult population of 48 patients includes seven who are unrepaired or have only palliative intervention. Applying the mortality assumptions outlined in Methods, we estimate the expected regional adult single-ventricle population in 2023 will be 76, of whom 45% will be over the age of 30 years. This would equate to an overall UK population of adults with single-ventricle physiology of just over 1650. Figure 4 depicts the growth in the overall population and in the proportion of those over 30 years of age.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Current and predicted Northern Congenital Abnormality Survey and UK adult single-ventricle population with the proportion expected to be over 30 years of age.
Discussion
The present study reports, for the first time, a population-based prevalence of single-ventricle physiology among children and adults and, based on simple modelling, a prediction of the size and composition of the adult single-ventricle population in the next decade. We estimate that there are currently just over 1000 adults with single-ventricle physiology in the UK and predict that this number will rise to around 1650 over the next decade.
Few other contemporary studies report frequency of single-ventricle physiology in the adult population. A recent Canadian study, where healthcare access is universal, reported a prevalence of 3 per 100 000 adults for the year 2000.11 These findings however were determined from an administrative database, and the possibility of miscoding was highlighted. While it could be argued that our sample may not be representative, our live birth prevalence of single-ventricle physiology is broadly comparable with other cohorts, and our rate of surgical repair proportionate.2 ,12 ,13 The birth incidence of congenital heart disease in our region is 962 per 100 000, which is towards the upper end of the range (437–1140 per 100 000) reported by other regions of the UK that hold registry data and is compatible with contemporary European data.14 ,15
While, the most common diagnoses in those over 5 years of age are DIV and TA, in those less than 5 years of age, HLHS is more prevalent and, significantly, we are now beginning to see the first adult survivors with this condition. It is also worth noting that all paediatric single-ventricle patients over the age of 5 years have either a Glenn or Fontan completion. These facts reflect the remarkable developments that have occurred in cardiac surgery over the last half-century, and indicate that we should expect continued growth and greater complexity in the adult population beyond the next decade.16 ,17
It is possible that termination of pregnancy will impact on the single-ventricle population, and this study also addresses this. Over the last decade (2003–2012), in our region, 50 terminations of pregnancies were performed for 127 fetal diagnoses. In the preceding decade (1993–2002), 58 terminations of pregnancies were performed for 88 fetal diagnoses. Our data indicate, that latterly fetal detection has improved, but that proportionately more parents are electing to continue the pregnancy. This, alongside improved surgical outcome, has resulted in an observed increase in the current paediatric population who will progress to adulthood in the next decades. This contrasts with the previously expected impact of termination of pregnancy rates on the prevalence of congenital heart disease.18 However, overall detection rates outside specialist tertiary centres remain low, and considerable inconsistency in counselling strategies for these diagnoses remain among tertiary centres, therefore, it may be difficult to generalise these results.19 ,20
We also report on functional status of the current population of adults with single-ventricle physiology. It is interesting to note that those in NYHA functional class 3 are almost all over 30 years of age. This may reflect the expected gradual age related decline in function first identified by Fontan.21 However symptoms in this group may also reflect the fact that some have not had Fontan completion, or the era in which the surgery was carried out. Better outcomes and later onset of symptom may therefore be expected in patients who have been operated upon in the modern era, as compared to those who have had less efficient Fontan procedures. It is of note that our population is composed primarily of patients who have undergone total cavopulmonary connection, which was instigated at our unit in 1991, in comparison with the historical reference group we have used to model mortality in our adult patients.3 However, it is also possible that certain diagnoses, such as those with classical HLHS, will do less well in the long term despite these surgical advances. Sixteen percent of our current population are NYHA Class 3, which corresponds to 165 patients nationally. If we assume a similar rate in a decade, then we will have 264 such patients. This is, however, a conservative estimate, as with a greater proportion of the population over 30 years of age, we may hypothesise symptoms are likely to be more frequent.
There would appear to be broad agreement that when patients develop symptomatic heart failure, the only realistic hope for prolongation of life in patients with single ventricle is successful transplantation. Currently, as is widely publicised, there is a shortage of donors with many patients on the waiting list dying; this is not likely to change in the foreseeable future.22 Single-ventricle patients, as with other congenital heart disease patients, may have high levels of preformed human leucocyte antibodies, complicated reconstructed anatomy and elevated pulmonary vascular resistance, and are at high risk for transplantation.23 Furthermore, while those with Fontan palliation are more likely to be considered for transplant during their lifetime, worryingly, they also perform worse following treatment.24 The growing problem of very sick patients on the transplant list dying, has stimulated development and use of ventricular assist devices, but their ability to support the failing single-ventricle circulation in the medium term is unknown. The numbers provided in the present study will help inform discussion for strategic planning of heart transplantation and assist devices in this group.
The prognosis for children with single-ventricle physiology, who are currently well, is unknown, but expected to be significantly worse than for those with two-ventricle repair. The process of transition is critical and likely to be difficult. Information on future uncertainties, and the possibility of limited medical treatment options, may be difficult to accept at any age, but particularly in the teenage years.4 The important issues of family planning, life insurance, recreation and career planning may all need to be addressed. In the longer term, preconceptual counselling and focused maternity and postnatal care will be essential to ensure patient expectations are appropriate and outcomes are optimal. It is clear from our data that the single-ventricle population is already of significant size and that, as the size and complexity of the population increases, deficits in providing and managing transition and the availability of specialist services will be exposed. The data provided here should inform this planning process.
Limitations
Classification of conditions is made according to a recognised schema, however, conditions are not always distinct, and there is a subjective element to classifying patients with multiple abnormalities. We have not attempted to find patients born before 1985 in the region who are resident elsewhere, so national population estimates represent a minimum. Only those with unbalanced defects who have actually undergone Fontan or Glenn surgery were included; this may contribute to underestimation of the live birth rate in particular, and less so, current population size. Survival assumptions for current adult patients are based on a cohort with a higher proportion of atriopulmonary Fontan repairs.3 Mortality may, therefore, be overestimated for this group and predicted population numbers thus represent a bare minimum. Finally, our cohort may not truly reflect other regions, as the diagnosis and management of patients with unbalanced ventricles is not uniform, and other units may adopt a more or less aggressive strategy to Fontan palliation as opposed to biventricular repair.
Summary
The present study shows that the single-ventricle population in the UK will consist of approximately 1650 adults at the end of the next decade. Data presented on functional status supports symptomatic decline over time. Detailed study of this growing population requires cooperation between units if issues, such as transplant assessment, impact of assist devices and use of medical therapies, which are critical to the care of these patients, are to be addressed.
Key messages
What is already known on this subject?
-
Patients with complex congenital cardiac conditions resulting in single-ventricle physiology are rare but high consumers of health service resources, and a growing group of young adults meeting criteria for cardiac transplantation, a scarce resource. Little evidence is available on the prevalence of this condition or, indeed, the current population size.
What this study adds?
-
Live birth, paediatric and adult prevalence rates for single-ventricle physiology. An estimate of the current and future UK population of adults with single-ventricle physiology who will likely become transplant candidates. An assessment of the effects of antenatal diagnosis and termination of pregnancy on live birth prevalence of single-ventricle physiology.
How might this impact on clinical practice?
-
Our study indicates there are currently around 1040 adults with single-ventricle physiology in the UK, and that this number is set to rise by over 60% in the next decade. This information is critical to initiate debate as to what service provision can and should be made available.
References
Footnotes
-
Acknowledgments We are grateful to the Link Clinicians in the Northern region for their continued collaboration and support of the Northern Congenital Abnormality Survey (NorCAS).
-
Contributors LC and JOS conceived, conducted and reported this study and were involved at all stages of data acquisition, analysis and interpretation. SOC contributed to data analysis and helped develop the first draft of the manuscript. CW contributed to data collection, provided epidemiological advice and revised the manuscript.
-
Funding The Children's Heart Unit Fund supports the Regional Paediatric Cardiac Database. We are indebted to Mary Bythell of the Regional Maternity Survey Office and to Valerie Sutherland of the Regional Paediatric Cardiology Database for help with the data. NorCAS is funded by the Healthcare Quality Improvement Partnership.
-
Competing interests LC and JOS have received research grants from the Academy of Medical Sciences and the Newcastle Hospital Charities for unrelated research.
-
Ethics approval NorCAS is one of seven linked surveys of maternal and infant health housed at the Regional Maternity Survey Office in Newcastle upon Tyne. The Patient Information Advisory Group has granted exemption from a requirement for consent for inclusion on the NorCAS register under section 60 of the Health and Social Care Act (2001). NorCAS, as part of the British Isles Network of Congenital Anomaly Registers, has ethical approval (04/MRE04/25) to undertake studies involving the use of the data. The departmental database has Caldicott approval for clinical and research purposes.
-
Provenance and peer review Not commissioned; externally peer reviewed.