Article Text

Abstract
Objective After the arterial switch operation (ASO), disproportional neo-aortic growth during childhood has been reported. Even though it has been suggested neo-aortic dilation will stabilise in adulthood, data are lacking. The aim of this study was to assess the change in neo-aortic dimensions, prevalence of neo-aortic dilation >40 mm and long-term outcome in adults who underwent ASO in childhood.
Methods All 116 ASO patients operated in a tertiary referral centre and born before 1995 were included. Of these, 83 (72%) survived to adulthood (>17 years) and six were lost to follow-up. Neo-aortic measurements performed in adulthood were collected from available echocardiographic, cardiovascular magnetic resonance and CT images. The time trend was analysed using a mixed model, adjusted for imaging modality.
Results Clinical data with at least one measurement of the neo-aortic diameter were available in 77 (93%) adult patients and serial measurements in 65 (78%). At baseline (median age 18.1 years), mean neo-aortic diameter was 36±5 mm. Mean neo-aortic growth was 0.31 mm/year (p<0.001 compared with normal value 0.08 mm/year) and was linear over time. Freedom from neo-aortic dilation beyond a diameter of 40 mm was 23% at 28 years of age. During a mean clinical follow-up in adulthood of 7.2 years (IQR 4.0 to 10.1), 3 (4%) patients underwent neo-aortic replacement. No other neo-aortic complications occurred.
Conclusions In early adulthood, neo-aortic growth was on average linear and did not stabilise over time.
- Cardiac Surgery
- Aorta, Great Vessels and Trauma
Statistics from Altmetric.com
Introduction
Even though initial results were unsatisfactory, the arterial switch operation (ASO) has gradually supplanted the atrial switch operation as the treatment of choice for patients with dextro transposition of the great arteries (D-TGA). The procedure involves translocation of the pulmonary artery and aorta above the level of the sinuses and the coronary ostia are reimplanted in the neo-aorta.1 This causes the original pulmonary valve and proximal main pulmonary artery to become the neo-aortic valve and proximal neo-aorta. Long-term results outperform the atrial switch operation, which leaves the RV supporting the systemic circulation and is associated with progressive systemic right ventricular failure,2–6 decreased exercise capacity,7 ,8 and arrhythmia and premature death.9 ,10 However, long-term complications after ASO have also been recognised as well. They include coronary complications,11–13 right ventricular outflow tract obstruction14–17 and neo-aortic valve regurgitation.18–20 Moreover, neo-aortic dilation is present in the majority of adult patients.21 ,22 However, little data exist concerning the progression of neo-aortic dilation in adulthood, and it has been suggested neo-aortic dilation will stabilise over time.23 The aim of the present study was to assess whether neo-aortic dilation remained progressive in early adulthood in patients who underwent ASO in early childhood. Moreover, we assessed the prevalence of neo-aortic dilation >40 mm and long-term clinical outcome of the neo-aorta after ASO in adults.
Methods
All patients with D-TGA or Taussig–Bing anomaly who had an ASO at the Center for Congenital Heart Disease Amsterdam-Leiden (CAHAL) between January 1977 and December 1994 with a last known permanent contact address in the Netherlands, and were still alive at 18 years of age were included in the present analysis. Surgical techniques in this cohort have been described previously.24 Surgery was performed by a total of three surgeons.
Neo-aortic measurements performed from 17 years of age were collected from all available echocardiographic, cardiovascular magnetic resonance (CMR) and CT images and reports. In addition, hospital and outpatient records were reviewed to obtain demographics, describe preoperative anatomy and collect clinical events. The study was conducted in accordance with all human research regulatory guidelines and the institutional conduct code for health related research.
Echocardiographic measurements
Dimensions of the neo-aorta at midsinus level were measured from parasternal long-axis views. Neo-aortic size was measured in accordance with the European and American guidelines using a leading edge to leading edge measurement of the maximal distance between the anterior aortic wall and the posterior aortic wall at end diastole.25 ,26 The degree of neo-aortic regurgitation was estimated by the width and length of the regurgitant jet using colour flow Doppler and classified as mild, moderate or severe according to the guidelines.27 ,28 All measurements were performed locally by experienced personnel.
CMR and CT
CMR and CT neo-aortic measurements were performed in cine imaging sequences of the long axis of the neo-aorta at midsinus level during diastole. Acquisition protocols differed per location and patient. All measurements were performed locally. Measurements were adjusted for imaging modality using a linear mixed model. CMR and CT imaging was not used for the quantification of neo-aortic regurgitation.
Stable versus dilating neo-aorta
For each patient, individual neo-aortic dilation was defined as the slope of a linear model based on all measurements available for that patient. For the purpose of examining possible determinants of neo-aortic dilation, the patient population was divided into a stable and a dilating group. Taking into consideration the variation caused by measurement error, the neo-aorta in patients with slopes below the 50 percentile was considered stable, whereas the neo-aorta in patients with slopes above the 50 percentile was considered to be dilating. The median was chosen to provide optimal contrast between the two groups, with regard to possible determinants of speed of neo-aortic dilation.
Outcomes and neo-aortic complications
Patients were considered to have a dilated neo-aorta from the moment a midsinus level neo-aortic diameter greater than 40 mm was measured in adulthood (>17 years).
Progression of neo-aortic valve regurgitation was estimated from the first and last available echocardiogram. In addition, the occurrence of death and aortic complications was assessed. Neo-aortic complications were defined as aortic root or valve reoperation, postoperative infective endocarditis of artificial valve or prosthesis, aortic dissection or rupture.
Statistical analysis
Analyses were performed using SPSS V.20 (IBM) and R V.2.14.1 (The R Foundation for Statistical Computing). Data were summarised as number (%) for categorical variables, mean±SD for continuous variables with normal distribution and median (IQR) for continuous data with skewed distribution. A mixed model (R package LME4) adjusted for imaging modality was used to assess neo-aortic dilation over time and determinants of neo-aortic diameter. The imaging modality (echo, CMR or CT) was added as a factor in the mixed model. Subsequently, all individual values were adjusted for imaging modality using the coefficients from the mixed model.
Several models were tested for best fit, among which were multivariable fractional polynomials and splines. The model with the lowest Aikake Information Criterion was considered to have the best fit. Kaplan–Meier analysis was performed to assess freedom from neo-aortic dilation >40 mm, using a method for interval censored data, which takes cases that were considered significantly dilated at baseline (left censoring) into account (package survival, method ‘interval’). χ2 Tests, Student independent t test or Mann–Whitney U was used to evaluate differences at baseline between patients with stable and dilating neo-aorta.
Results
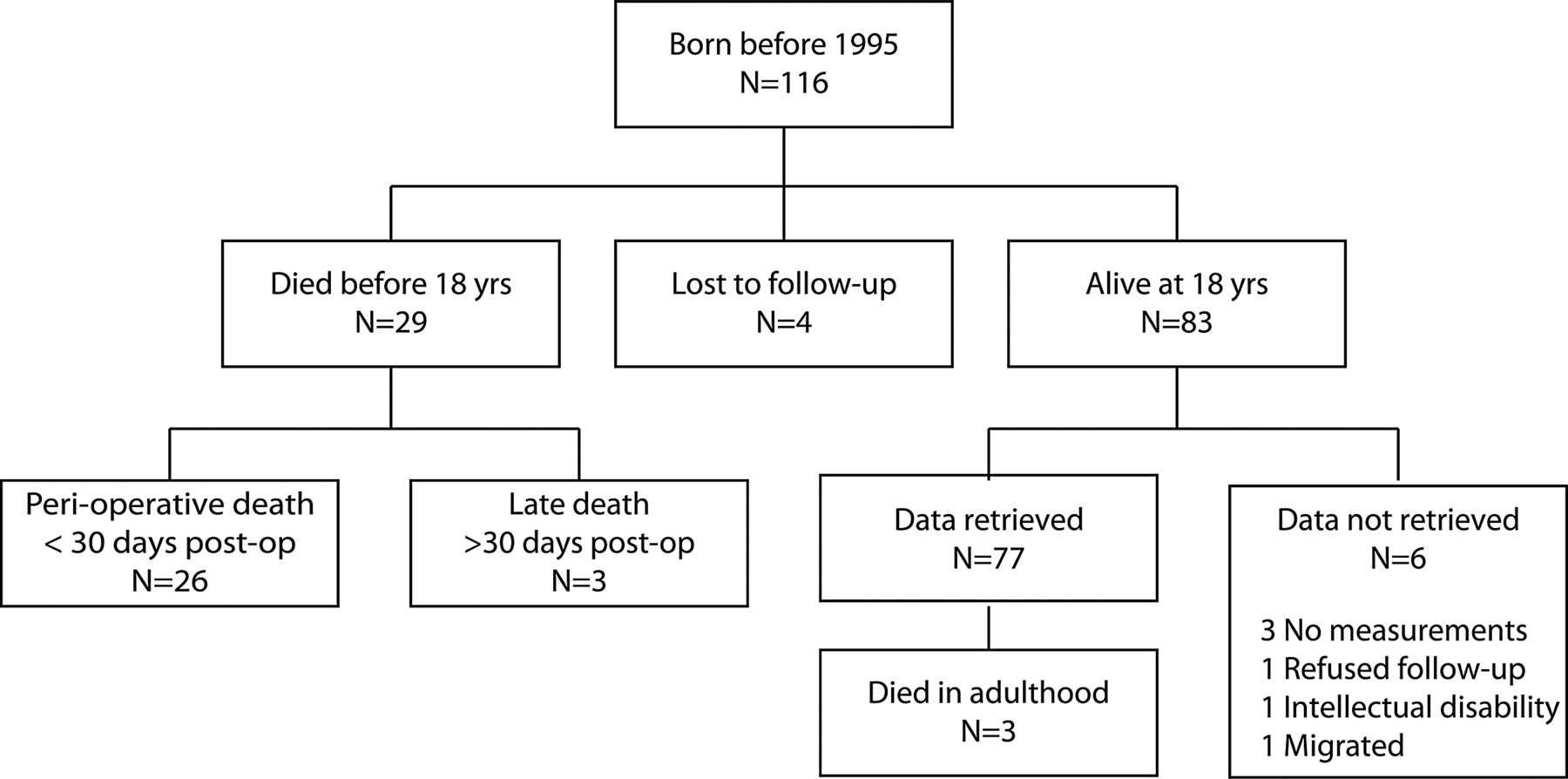
Between January 1977 and December 1994, 116 patients underwent ASO. Of these, 29 died during childhood and four were lost to follow-up, leaving 83 adult survivors (figure 1). Data on the neo-aortic diameter were available in 77 (93%) adult patients with serial measurements available in 65 (78%) of these patients. The analysis included 288 neo-aortic measurements: 194 (67%) from echocardiography, 68 (24%) from CMR and 26 (9%) from CT. Baseline parameters are summarised in table 1.
Baseline characteristics by neo-aortic dilation
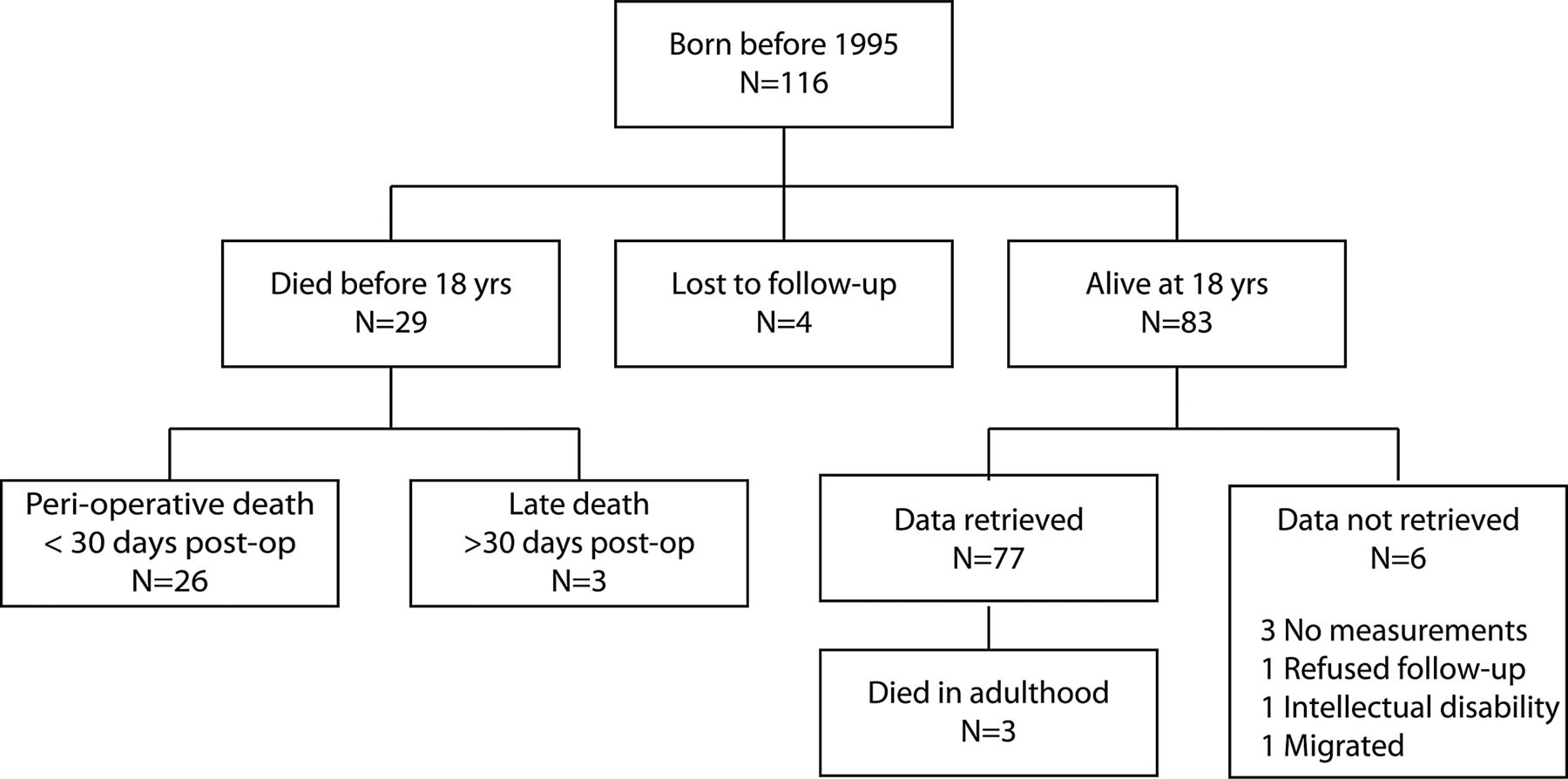
Flow diagram of cohort derivation.
Neo-aortic dilation
At baseline (median age 18.1 years), mean neo-aortic diameter was 36±5 mm. A linear mixed model gave the best fit. Mean neo-aortic growth was 0.31 mm/year (p<0.001 compared with normal value 0.08 mm/year29) (figure 2). In 7 (11%) patients, neo-aortic growth was 1 mm/year or higher. In univariate mixed model analysis, age, sex, age at operation, coexisting ventricular septal defect (VSD), patent ductus arteriosus or Taussig–Bing anomaly, and neo-aortic regurgitation were significantly associated with neo-aortic diameter (table 2).
Determinants of neo-aortic size
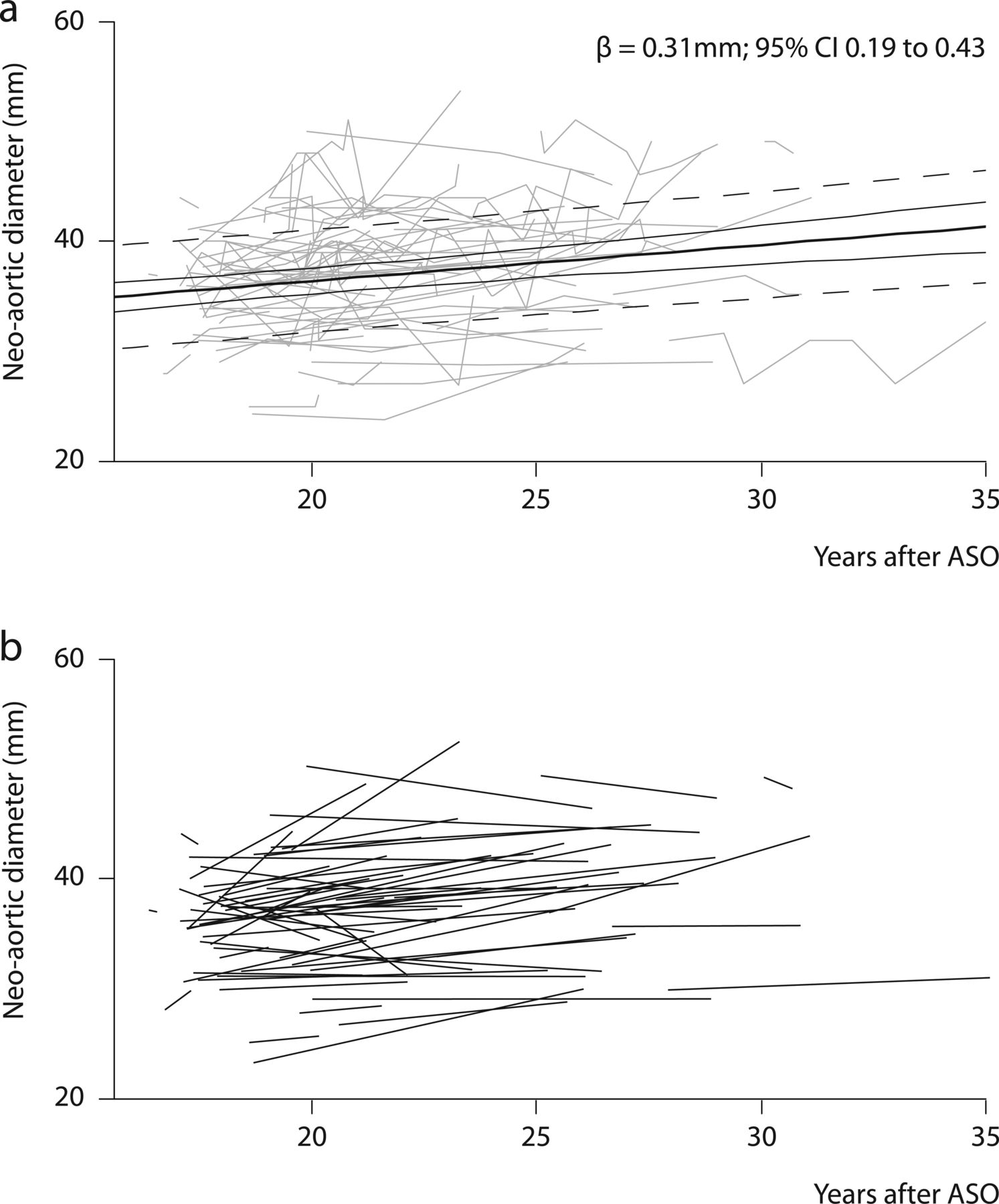
Time trend for neo-aortic diameter in adult patients after arterial switch operation (ASO); (A) each line represents the individual midsinus level neo-aortic measurements of one patient; bold line: mean neo-aortic growth; plain lines: 95% CI of regression line; dashed lines: 95% prediction interval; (B) each line represents the mean slope, based on the individual neo-aortic measurements of one patient.
Using only echocardiographic measurements, mean neo-aortic growth was 0.28 mm/year (p<0.01 vs normal). Using only CMR measurements resulted in mean neo-aortic dilatation of 0.31 mm/year, but this was not significantly different from normal (p=0.08). No serial CT measurements were available.
Stable versus dilating neo-aorta
The 50th percentile of individual change in neo-aortic diameter over time was 0.34 mm/year. Median progression was −0.02 mm/year (IQR −0.53–0.19) in the stable group (growth <0.34 mm/year) and 0.77 mm/year (IQR 0.47–0.97) in the dilating group (growth >0.34 mm/year). Patients in whom the neo-aorta was stable were slightly older at the time of their last measurement and had higher baseline neo-aortic diameter than patients in whom the neo-aorta dilated over time. No other statistical significant differences were found between the two groups (table 1).
Outcomes
In 4 (5%) patients, neo-aortic dilation >40 mm was present before reaching adulthood. Freedom from neo-aortic dilation was 56% at 23 years of age (approximately 5 years follow-up, figure 3) and subsequently remained decreasing with age. During follow-up, a neo-aortic diameter wider than 45 mm was measured in 10 (13%) patients and a neo-aortic diameter wider than 50 mm in 4 (5%) patients. At baseline, 8 (10%) patients had moderate neo-aortic valve regurgitation and 3 (4%) had received an artificial aortic valve during childhood for treatment of haemodynamically significant neo-aortic regurgitation. Only two patients progressed from none or mild to moderate or severe neo-aortic valve regurgitation.

{kind=link}
{kind=link}
{kind=link}
Freedom from neo-aortic dilation—Bold line: first neo-aortic measurement >50 mm; dashed line: first neo-aortic measurement >45 mm; dotted line: first neo-aortic measurement >40 mm; patients with neo-aortic root dilation at baseline were included in the analysis and censored at the age of 17 years.
Neo-aortic complications
Cumulative clinical follow-up in adulthood was 569 years. During a median follow-up of 7.2 years (IQR 4.0 to 10.1), 3 (4%) patients died; one sudden cardiac death with evidence of lymphocytic myocarditis on autopsy, one patient died due to thrombosis of left and right pulmonary arteries after an attempted percutaneous procedure, and in one patient cause and circumstances of death were unknown.
Moreover, 3 (4%) experienced neo-aortic complications. Neo-aortic root replacement (one root sparing, two Bentall procedures) was performed in three patients. Neo-aortic diameters were 53, 51 and 46 mm (the last had severe neo-aortic valve regurgitation). One of these patients had a severely complicated postoperative course, with infective endocarditis of the Bentall prosthesis and multiple reoperations. No dissection or rupture occurred.
Discussion
The present study, for the first time, demonstrates that neo-aortic dilation remained progressive throughout early adulthood in patients who underwent ASO in early childhood. Growth was linear and did not stabilise over time in this period. The majority of patients progressed beyond a diameter of 40 mm during adulthood. Progressive dilation of the neo-aorta did not coincide with progression of neo-aortic regurgitation.
In two recent single centre cross-sectional evaluations of adult patients after ASO, neo-aortic dilation was present in the majority.21 ,22 The present study shows that progressive neo-aortic dilation remains persistent over time with a rate of 0.31 mm/year, significantly increased compared with aortic growth 0.08 mm/year in healthy individuals.29 Growth appeared to be linear. For comparison, yearly aortic growth in patients with Marfan Syndrome has been reported to be 0.41 mm30 and 0.28 mm in patients with aortic coarctation.31 Over a follow-up of approximately 10 years, only 36% of patients remained free of neo-aortic dilation >40 mm. There was large variation between patients in both baseline neo-aortic dimensions and change in neo-aortic diameter over time. We found no difference in baseline characteristics between patients with stable neo-aorta dimension and those in whom neo-aortic dilation was progressive.
Several studies have reported an already disproportional neo-aortic growth during childhood that did not stabilise over time.19 ,32–34 In contrast, Hutter et al23 showed a normalisation of neo-aortic Z-scores after rapid increase during the first year after ASO. In our study, the association between neo-aortic dimensions and time is best described by a linear relation, which seems to support the hypothesis that progressive neo-aortic dilation does not stabilise and persists throughout adulthood.
Despite often substantial neo-aortic dilation, the need for intervention remains unclear. To our knowledge, there have been no reports of neo-aortic rupture or dissection in a dilated neo-aorta after ASO to date. However, dissection has been noted at least four times in patients with pulmonary autograft after the Ross procedure.35 Many centres will empirically proceed to surgical intervention when neo-aortic diameter exceeds a certain limit. In our cohort, three patients received neo-aortic root replacement at neo-aortic diameters over 50 mm or lower when severe neo-aortic valve regurgitation was present. When extrapolating a mean neo-aortic growth of approximately 1 mm per 3 years, as found in the present study, it can be expected that 7 (10%) patients will cross 50 mm in the next 15 years and may need to be considered for replacement surgery.
Moderate neo-aortic valve regurgitation has been reported in up to 15 % of patients after ASO.18 This is comparable with our cohort in whom 10% had moderate neo-aortic valve regurgitation and 4% had aortic valve prosthesis. However, in accordance with several reports,14 ,21 haemodynamically important neo-aortic valve regurgitation was relatively rare in this population. While neo-aortic regurgitation was associated with neo-aortic dimensions, dilation of the neo-aorta did not coincide with progression of neo-aortic regurgitation.
Previous studies have shown relation of neo-aortic dilation and surgical technique or era. The most consistent finding is relation between prior pulmonary artery banding (PAB) and development of neo-aortic dilation.13 ,18 ,19 ,32 ,33 In the present study, PAB was not significantly associated with neo-aortic dimensions. Possibly, the effect of PAB wanes over time. However, there were only three patients with PAB in our cohort, which might have led to an underestimation of the effect of PAB. In contrast to previous work,33 era of operation was not related to aortic dimensions. Anatomic determinants of neo-aortic dilation included the presence of a VSD and Taussig–Bing anomaly, which have both been reported previously.19
Generalisability
This cohort represents the first patients who underwent ASO in the Netherlands. Consequently, as reported previously, initial mortality was high. As surgical techniques and survival have improved over time, our findings might not apply to future cohorts. However, our cohort is representative of patients who are currently seen in adult congenital heart centres.
Limitations
The study was retrospective and included neo-aortic diameters measured using different imaging modalities. Although we adjusted for modality using a mixed model, variation in imaging practice over time might have influenced our findings. However, when only echocardiographic measurements were taken into account, growth was still apparent. This suggests that the influence of image practice was minor. Moreover, the number of adult patients who underwent ASO is comparatively small, and serial measurements were not available in all patients. Data beyond the age of approximately 25 years were limited. Consequently, there may well be a non-linear relationship afterwards, although available data do not imply such a trend. Finally, to avoid the confounding effect of weight gain, we did not adjust neo-aortic diameter for body surface area, which is common practice in paediatric reports when body growth interferes with aortic measurements.
Conclusions
In patients who underwent ASO, neo-aortic dilation was persistent in early adulthood. Growth was linear and did not stabilise over time. Progressive dilation of the neo-AR did not coincide with progression of neo-aortic regurgitation.
Key messages
-
What is known on this subject?
-
In patients who underwent an arterial switch operation, disproportionate growth of the neo-aorta has been reported in early childhood. However, reports on the course of the neo-aorta beyond childhood are contradictory and scarce.
-
What might this study add?
-
The present study shows that disproportionate neo-aortic dilation continues in early adulthood. It is the first study that focuses on neo-aortic dilation in early adulthood. Extrapolation of our data seems to indicate that 10% of patients will dilate beyond 50 mm within 15 years.
-
How might this impact on clinical practice?
-
Follow-up of neo-aortic dimensions during adulthood seems indicated. Moreover, patients with severe neo-aortic dilation may need to be considered for replacement surgery.
Acknowledgments
The work described in this study was carried out in the context of the Parelsnoer Institute (PSI). PSI is part of and funded by the Dutch Federation of University Medical Centers.
References
Footnotes
-
TvdB and RLFvdP contributed equally to this study.
-
Contributors All authors were involved in the preparation of the manuscript, have read the manuscript, agree with the analyses of the data and the conclusions reached in the manuscript and are accountable for all aspects of the work.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.