Article Text

Abstract
Objectives We hypothesised that soluble ST2 (sST2) levels can identify people with elevated risk of subsequent cardiovascular disease (CVD) and add to existing risk prediction algorithms.
Background ST2 is a receptor for the inflammatory cytokine IL33. Increased sST2 levels have been associated with heart failure and death in acute myocardial infarction patients and in the general population.
Methods We measured high-sensitivity sST2 in 8444 men and women (25–74 years) from the FINRISK97 prospective population cohort. Cox proportional hazards modelling evaluated the ability of sST2 to predict fatal and non-fatal heart failure, CVD (coronary heart disease, stroke), diabetes, and death over 15 years follow-up. Discrimination and reclassification statistics for 10-year absolute risks compared the ability of sST2 to improve upon Framingham risk factors (FRF), N-terminal pro-brain natriuretic peptide (NT-proBNP), renal function (eGFR) and prevalent valvular heart disease (VHD).
Results sST2 showed suggestive but non-significant associations with heart failure {(HR per 1 SD of log sST2 1.06; 95% CI 0.96 to 1.17 (562 events))}, and with CVD (1.01 95% CI 0.94 to 1.08) (914 events) after adjustment for FRF, NT-proBNP, eGFR and VHD. sST2 significantly predicted death from all causes following similar adjustment ({HR 1.09 (95% CI 1.01 to 1.19) (974 events))}. No improvement in the c-index was observed for models adding sST2 to the risk factors.
Conclusions In a healthy general population from Finland, sST2 did not improve long-term prediction of cardiovascular events including heart failure or all-cause mortality.
- CORONARY ARTERY DISEASE
- HEART FAILURE
Statistics from Altmetric.com
Introduction
Cardiovascular diseases (CVD) make the greatest contribution to morbidity and mortality in many parts of the world.1 Biomarkers representing inflammation (c-reactive protein (CRP), renal function (Cystatin C), myocyte injury (Troponin), vasoactive and neurohormonal peptides (NT-proBNP, MR-proADM) can improve 10-year CVD risk prediction beyond what is possible with classic risk factors (smoking, cholesterol levels, blood pressure and prevalent diabetes) either individually,2 or in various combinations.3 ,4 In particular, the natriuretic peptides, for example, NT-proBNP, predict outcomes in patients with heart failure, acute myocardial infarction (MI), and in the general population. These biomarkers may be more specific to heart disease because they are released from cardiomyocytes.
ST2 is a biomarker with vasoactive and neurohormonal properties affecting cardiac stress similar to the natriuretic peptides. ST2 is also known as Interleukin 1 receptor-like 1 (IL-1RL-1) and exists in two isoforms: the membrane-bound ST2 ligand (ST2L) and soluble ST2 (sST2). ST2 acts as a receptor for proinflammatory T helper 2 associated cytokine IL33 and is cardioprotective, mitigating the cellular responses to cardiac mechanical stress.5–,8 Loss of intact IL-33/ST2L signalling results in unchecked remodelling of ventricular myocardium characterised by excessive myocyte hypertrophy, fibrosis and worsening of left ventricular function.7 ,9 Soluble ST2 (sST2) may act as a decoy receptor for IL33, and high levels of sST2 in the peripheral circulation may interfere with signalling leading to loss of its cardioprotective effects.6–,8
In patients with heart failure and acute dyspnoea increased sST2 levels predict mortality independently of NT-proBNP and other markers.9 ,10 Elevated sST2 levels in patients with acute MI are associated with increased risk of mortality or heart failure independent of natriuretic peptides.11 ,12 Serial changes in sST2 over time predict outcomes independent of natriuretic peptides, suggesting its potential use in monitoring heart failure,13 or guiding therapy for acute coronary syndromes.14 In the general population, sST2 levels were associated with cardiovascular death and heart failure in the Framingham cohort and mortality in Framingham and Dallas Heart Studies4 ,15 and also with incident diabetes.16 Unlike NT-proBNP, sST2 levels are not related to age, prevalent heart failure, atrial fibrillation, Body Mass Index, or renal function in studies spanning those at high risk, and general populations.4 ,5 ,10 ,15 ,17
sST2 may offer prognostic potential in a broad spectrum of patient settings. Recent development of a highly sensitive sST2 assay allows us to test the clinical utility of sST2 in a large general population of initially healthy participants from Finland, FINRISK97 which have accumulated large numbers of incident cardiovascular events, coronary heart disease, stroke, heart failure and incident diabetes. We evaluate the predictive ability of sST2 to add to and exceed existing risk prediction algorithms for CVD and related endpoints containing classic risk factors, renal function and NT-proBNP; specifically, we test in this situation whether sST2 can improve prediction of incident heart failure compared to the already established natriuretic peptide NT-proBNP.
Methods
The study population
The prospective population-based FINRISK97 study selected 11 500 individuals from the national population register in 1997 and recruited 8444 (67%) men and women aged 25–74 years.18 Individuals were recruited from five districts of Finland, including North Karelia, Northern Savo (former Kuopio), Southwestern Finland, Oulu, Helsinki and Vantaa. Participants received a physical examination, a self-administered questionnaire, and a blood sample was drawn. Smoking status, blood pressure and lipid measurements were collected in a standardised manner. Prevalent diabetes was defined as self-reported doctor-diagnosed diabetes, use of diabetes medication or diabetes history recorded in registry data. All subjects provided written informed consent to study participation, and the study was approved by the Coordinating Ethical Committee of the Helsinki and Uusimaa Hospital District.
Outcome information
During a follow-up of up to 15 years, the National Hospital Discharge Register, the National Causes of Death Register and the National Drug Reimbursement Register were used to identify incident cardiovascular endpoints. Countrywide follow-up coverage of all hospitalisations and deaths in Finland was achieved with loss to follow-up of 0.5% of participants who permanently moved abroad (prior to 31 December 2011). Fatal and non-fatal endpoints during follow-up were first major CVD events which combined first coronary heart disease (defined as MI, coronary death, hospitalised unstable angina pectoris, any coronary revascularisation (percutaneous transluminal coronary angioplasty or coronary bypass surgery), and ischaemic stroke (haemorrhagic strokes were excluded), incident heart failure, first MACE (Major Adverse Cardiovascular Events of CHD, stroke or heart failure), incident diabetes (use of antidiabetic medication during follow-up) and all-cause mortality. CHD, MI and stroke were analysed individually. Definition of endpoints followed MORGAM, and AHA criteria and the high validity of endpoints derived from these registers has been demonstrated.19 ,20
Biomarker measurements
sST2 was measured using the highly sensitive Presage ELISA assay (Critical Diagnostics) which has FDA approval.21 The intra-assay COV was 5%, and interassay COV ∼13%, with the limit of quantification at 2.35 ng/mL. NT-proBNP, cystatin C, creatinine and high sensitivity troponin I ((Abbott Diagnostics, USA, ARCHITECT i2000SR) measurements were previously described.2 ,3 sST2 was measured by Critical Diagnostics, San Francisco, USA, while other biomarkers were measured in the MORGAM/BiomarCaRE laboratory, Hamburg, Germany.
Statistical analysis
Biomarker levels were natural log transformed to account for highly skewed distributions; Spearman's rank order correlation coefficients between variables were calculated. Multiple imputation was used to deal with missing values.22 Complete case analysis was also applied for sensitivity analysis. We excluded participants with prevalent disease at baseline for analysis of those endpoints involving incident disease. For most endpoints, baseline CVD was excluded, while for heart failure and MACE, prevalent MACE was excluded. We assessed the biomarkers as categorical (quartiles) and continuous variables. For continuous variables, log transformed biomarker distributions were standardised to per 1 log transformed unit of sST2. The associations between biomarkers and survival were estimated by a Cox proportional hazards model using age as survival time, and illustrated by age-adjusted survival curves using follow-up years as survival time. We first assessed sST2 in a model containing Framingham cardiovascular risk factors; gender, systolic blood pressure, high-density lipoprotein cholesterol, nonHDL cholesterol (difference between total and HDL cholesterol), prevalent diabetes and smoking status adjusted for the five regions of Finland. Subsequent adjustment considered estimated glomerular filtration rate (eGFR) calculated by CKD-Epi equation,23 other biomarkers (NT-proBNP, hsTnI) and prevalent valvular heart disease (VHD). Gender was also considered by sex-stratified Cox regression.
Analysis of incident diabetes excluded those with prevalent diabetes, and adjusted for HDL cholesterol, smoking, systolic blood pressure, antihypertensive medication, glucose, triglycerides, BMI, prevalent CHD and geographic area. We performed analysis adjusting for use of HRT in women (see online supplementary methods).17
In prediction modelling, 10-year absolute risks were estimated from Cox regression models with and without a biomarker. Tenfold cross-validation was used to avoid overfitting. We calculated the power to detect an effect with 80% power using the variance inflation factor to consider the effect of confounding variables.24
Discrimination criteria used to evaluate the prediction models were the c-index improvement25 integrated discrimination improvement (IDI),26 continuous net reclassification improvement (NRI),26 risk category-based NRI (with risk categories 0–5%, 5–10%, 10–20% and >20%)26 and clinical NRI (those at intermediate risk 10–20%).26 All statistical methods were implemented in R statistical software V.3.0.1 (http://www.R-project.org).
Results
The characteristics of the FINRISK97 participants are described in table 1. The mean age of participants was 48 years, with 50% men. Men had higher sST2 levels (mean 30.4 ng/mL) than women (mean 23.8 ng/mL). sST2 was not significantly correlated with most classic risk factors and novel biomarkers (see online supplementary table 1). There were 890 (10.5%) missing values for sST2, as no plasma remained for measurement. Similar results were observed when using the imputed and complete case analysis. Therefore, we report the main results using the multiple imputed data.
Characteristics of the FINRISK97 study population
Association of sST2 and specific cardiovascular endpoints
Cardiovascular disease
Over a 15-year follow-up, 914 CVD events were observed. We found no significant association between sST2 and CVD (HR per 1 SD of log sST2 1.01 95% CI 0.94 to 1.08) following adjustment for Framingham covariates (FRF) and geographic area (table 2). Prediction metrics were significantly worse for these models; (eg, c-index difference −0.0003, table 3) and remained non-significant upon further adjustment (table 2). sST2 demonstrated a trend of association across quartiles, but was not significant following adjustment for FRF and geographic area with incident myocardial infarction, (325 events), coronary heart disease (CHD) (635 events) and stroke (354 events) (table 2). Discrimination statistics were not significantly different, but IDIs were all significantly worse, that is, to the wrong direction (eg, for stroke (−0.001, p=0.002). Figure 1 presents Cox model results stratified by gender. The results for endpoints other than all-cause mortality (see below) were comparable between the genders, with no interaction between gender and sST2. Minimally adjusted HRs of sST2 for all endpoints are presented in online supplementary table 2 for comparison. The proportional hazards assumptions for sST2 were met in all models and, overall, the Cox assumptions in the models were met reasonably well.
Association of sST2 with cardiovascular and death endpoints
Metrics for improvement in risk prediction of cardiovascular disease with addition of sST2

Association of sST2 and incident events stratified by gender. HRs according to 1 SD unit of log transformed ST2 considering men and women separately for incident events. Model 1 includes adjustment for Framingham risk factors (HDL and non-HDL cholesterol, systolic blood pressure (BP), smoking, prevalent diabetes) and area. Model 2 includes additional adjustment for NT-proBNP, eGFR and prevalent valvular heart disease.
Table 1 hsTroponin indicates high sensitivity Troponin I. Biomarker values given are median and (IQR=75th percentile–25th percentile); *hypertensive as defined by AHA criteria SBP≥140 mmHg, DBP≥90 mmHg or receiving treatment for hypertension. Pregnant women were excluded from all analyses.
Heart failure
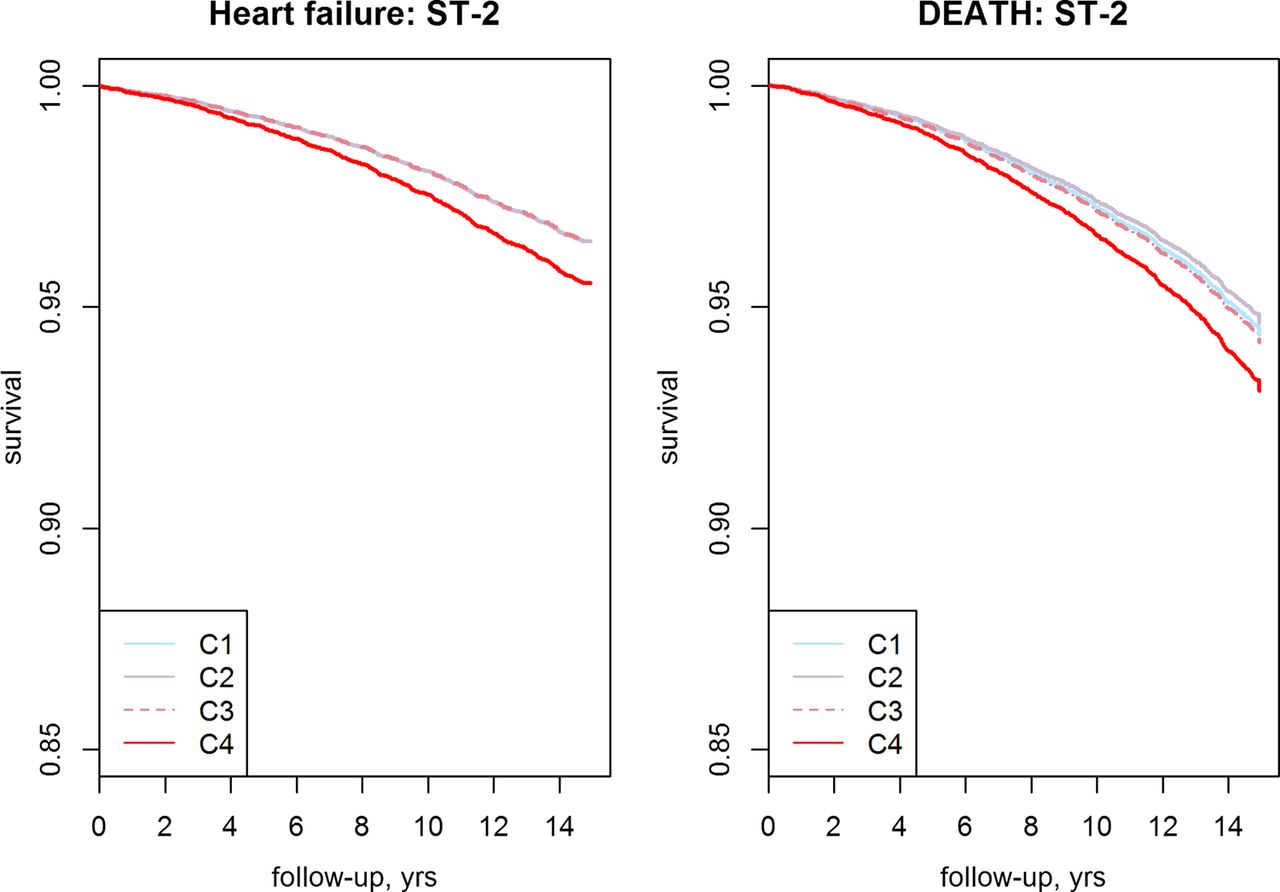
A total of 562 incident heart failure events occured over 15 years. Event-free survival curves adjusted for age and gender, illustrate differences in risk of heart failure across quarters of sST2. The chance of surviving event-free was higher for those in the lowest three-quarters than in the highest (figure 2). sST2 showed a suggestive, but not significant, association following adjustment for FRF and geographic area; HR per 1 SD of log sST2 1.08 (95% CI 0.98 to 1.19) (table 2, figure 2). Clinical NRI was improved for this model 0.04, p=2.05×10−2 with benefit mainly for non-cases and men, but no improvement for other prediction metrics (see online supplementary table 3). sST2 remained non-significant, but only marginally attenuated on further adjustment for eGFR, NT-proBNP, and prevalent VHD (table 2) with non-significant prediction metrics. The addition of hsTnI to these models did not change the estimates (table 2, model 3).
{kind=link}
{kind=link}
Kaplan–Meier survival curves. Kaplan–Meier survival curves adjusted for age and gender, assessing the time to death or heart failure with increasing year of follow-up across sST2 categorised into four quartiles (C1–C4), C1–C4 indicate the sST2 cutpoints used for analysis: C1=3–21.1 ng/mL, C2=21.1–27 ng/mL, C3=27–34.9 ng/mL, C4=34.9–462 ng/mL.
MACE
We analysed 1183 major adverse cardiovascular events. sST2 Showed a suggestive, but not significant association with MACE following adjustment for Framingham covariates and geographic area, risk prediction metrics were non-significant (table 2). Results were slightly attenuated when adjusted for NT-proBNP, eGFR and prevalent VHD (table 2), while the clinical NRI for this model became significant p=0.02, but with only 1% benefit; IDI was significantly worse; that is, to the wrong direction −0.001, p=0.003.
Association of sST2 and incident diabetes
sST2 showed a trend toward elevated but non-significant risk for incident diabetes (682 events), HR per 1 SD of log sST2 0.99 (95% CI 0.95 to 1.15) following adjustment (table 2). Prediction metrics were significantly worse for this model (c-index difference −0.0004 p=0.002, continuous NRI −0.17, p=0.001).
Association of sST2 with mortality
During a mean follow-up of 15 years, there were 974 deaths from any causes. The risk of all-cause mortality increased across sST2 categories in models adjusted for Framingham risk factors (FRF) and geographic area, but did not reach significance for individuals in the highest sST2 category compared to those in the lowest (table 2, model 1, figure 2). However, the HR per 1 SD of log sST2 reached significance HR 1.09 (95% CI 1.01 to 1.19), p=0.023 following adjustment for FRF and area. The clinical NRI (ie, in those at intermediate risk) was significant for this model (7.6×10−5) but not for other metrics (see online supplementary table 3). The relationship between sST2 and all-cause mortality was stronger in men compared to women (figure 1, see online supplementary table 3). This model remained significant upon adjustment for prevalent VHD, eGFR and NT-proBNP HR 1.09 (95% CI 1.01 to 1.19) (table 3, model 2). Clinical NRI was significant in both these models with an 8% benefit in the latter model (p=1.3×10−5). There was no improvement in the c index (p=0.06) or other reclassification metrics. The addition of hsTnI did not change the HRs, and added further improvement to clinical NRI p=4×10−8, (an 11% benefit), with a change in c-index approaching significance (p=0.051).
Discussion
Our objective was to evaluate the usefulness of sST2 for prediction of cardiovascular events, heart failure and death in a general population across a wide age range. Our results show that sST2 adds little predictive information beyond standard risk markers for cardiovascular endpoints, such as MACE, CVD and stroke, and is of marginal benefit to all-cause mortality prediction in a general population of healthy participants. sST2 also fails to improve prediction for heart failure either as an individual marker following adjustment for Framingham risk factors or in addition to the established cardiac marker NT-proBNP and/or eGFR. While sST2 demonstrates benefit in heart failure prognosis after diagnosis,27 it has limited value for predicting long-term risk of heart failure in the general population.
These results are obtained in a large Finnish population with high incidence of cardiovascular disease and a long follow-up. Our results expand upon previous studies4 ,15 in several ways: (1) results are extended to a wider range and larger number of cardiovascular endpoints, in particular, heart failure with a long follow-up; (2) results are not restricted to elderly or high-risk patients, but are extended to men and women across a broad age range; (3) we have adjusted for a range of important risk factors associated with cardiovascular disease and ST2, and adjusted the risk estimates for overoptimism by applying internal 10-fold cross-validation.
Our results for heart failure contrast with those from the Framingham Heart Study (FHS) which found a significant association of sST2 with heart failure based on 152 incident events after 11.3 years follow-up (HR per 1 SD of log sST2 1.45 95% CI 1.23 to 1.70).4 Our findings based on 562 incident cases and 15 years follow-up suggest that sST2 does not significantly improve prediction in addition to the Framingham risk factors alone or also adjusted for NT-proBNP and/or eGFR. Aside from different adjustments, exclusions and endpoint definitions, the Framingham study participants were, on average, older (59±10). Additionally, the phenotypic heterogeneity of heart failure makes it difficult to directly compare results from these studies. Our study had excellent power to detect a modest but clinically meaningful association for heart failure (80% power to detect HR 1.11). A putative role of sST2 is to mitigate the antihypertrophic effect of IL33/ST2 L leading to cardiac hypertrophy.5 Our findings are based on a larger number of events and accord with the Dallas Heart Study (DHS) which found only a weak association between sST2 and left ventricular mass and aortic wall thickness,15 suggesting that a putative hypertrophic effect of sST2 may be weak in younger participants, and that sST2 is not useful for stratifying risk in the early stages of heart failure disease development, or in clinically healthy individuals.
Our findings for MACE are also weaker than observed in FHS with a HR per 1 SD of log sST2 of 1.23 (95% CI 1.10 to 1.39), which may be explained by different adjustments and exclusions.4 Consistent with our findings, the FHS and DHS studies also found no significant association with cardiovascular disease of various types. (FHS: 173 coronary heart disease events with HR per 1 SD of log sST2 1.08 (95% CI 0.92 to 1.27)4; DHS: 185 non-fatal CVD events with HR 4th versus 1st quartile of 1.5 (95% CI 0.9–2.3).15 Indeed, we had sufficient power to detect a modest effect on MACE outcomes (80% power to detect a HR of 1.08 at p<0.05). While a trend of increased HRs is observed with these endpoints, sST2 could still reflect increased systemic inflammation and, to a lesser extent, enhanced fibrosis in damaged myocardium. The sST2 pathway has been associated with early development of atherosclerosis possibly through the promotion of proinflammatory cytokines and vascular leakage injuring the coronary artery endothelium and pancreatic endothelium.28 A combination of atherosclerosis and myocardial fibrosis could increase the risk of fatal endpoints, but the mechanism is not clearly understood.
Our results were strongest for all-cause mortality which is compatible with findings from FHS and DHS. The Framingham Heart Study HR estimate for death was stronger (HR per 1 SD of log 1.32 (95% CI 1.20 to 1.46)) than ours (HR per 1 SD of log sST2 1.09 (95% CI 1.01 to 1.19)), but FHS analysed less than half the number of deaths as were in our study (474 deaths). The Dallas Heart Study found a significant association with all-cause mortality comparing those in the 4th to the 1st quartile, HR 2.1 (95% CI 1.4 to 3.2) based on 164 deaths (aged 18–65 years), which was non-significant on further adjustment for NT-proBNP, cTnT, CRP and GDF-15.15 While this study suffered the complication of having only a fraction (33%) of 3294 participants with detectable sST2 concentrations using a Luminex assay (>0.4 μg/L equivalent to 1.3 μg/L of Presage assay), our study had measureable levels on 99% of participants.
Limitations
While sST2 may remain stable over long periods,29 biomarker measurements were carried out on specimens which had been stored for prolonged periods at −70 °C which could potentially distort the values. sST2 is elevated in a variety of conditions and pathophysiologies, such as inflammatory and respiratory illnesses, which could result in bias if not recorded at baseline. The cardiovascular outcomes in our study were ascertained using nationwide healthcare registers, which have been validated for this purpose.19 ,20 This is particularly relevant for heart failure, where our validation study showed excellent specificity but only modest sensitivity.20 We cannot exclude the possibility that we have missed some cases of heart failure which has weakened our risk estimates. It should be noted, however, that other putative biomarkers of heart failure, for example, NT-proBNP and mid-regional proadrenomedullin,30 provided results that were consistent with expectations in this cohort, and are clearly significant predictors of incident heart failure. Finally, the study was performed in a Finnish population of mainly European ancestry, and results may differ in populations with different levels of absolute risk or ethnicities.
Conclusion
Levels of sST2 in healthy men and women add little predictive information beyond standard risk markers for cardiovascular endpoints such as heart failure, MACE, CVD and all-cause mortality. While sST2 may not be useful for predicting future heart failure events in the general population, it may still be a useful marker for management of heart failure. Our results suggest that sST2 should not be considered for incorporation into risk scores for primary prevention of CVD.
Key messages
What is already known on this subject?
-
sST2 Is a novel biomarker showing predictive benefit in patients with heart failure and myocardial infarction in emergency situations. A smaller prospective study indicated it may have predictive value for cardiovascular death or heart failure in the general population. sST2 may function like natriuretic peptides (eg, NT-proBNP), be released from cardiomyocytes and, therefore, be a more specific biomarker for heart disease
What might this study add?
-
In a large study based on an initially healthy prospective cohort (>8000 participants), we show that sST2 did not improve long-term prediction of cardiovascular events (eg, incident fatal and non-fatal myocardial infarction, stroke, diabetes), heart failure or all-cause mortality beyond standard risk markers (Framingham risk factors, renal function, NT-proBNP).
How might this impact on clinical practice?
-
While sST2 may not be useful for predicting future heart failure or cardiovascular events in the general population, it may still be useful for management of acute heart failure. sST2 Should not be considered for incorporation into risk scores for primary prevention of CVD.
Acknowledgments
MORGAM annexe sites and key personnel: FINRISK collaborators, National Institute for Health and Welfare, Helsinki, V. Salomaa (principal investigator), A. Juolevi, E. Vartiainen, P. Jousilahti. MORGAM Data Centre; National Institute for Health and Welfare, Helsinki, K. Kuulasmaa (head), Z. Cepaitis, A. Haukijärvi, B. Joseph, J. Karvanen, S. Kulathinal, M. Niemelä, O. Saarela. MORGAM Biomarker Laboratory-, Department of General and Interventional Cardiology, Universitäres Herzzentrum Hamburg, Hamburg University Heart Center, Hamburg, Germany formerly located at Johannes Gutenberg-University, Mainz: S. Blankenberg, T. Zeller.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Funding This work has been sustained by the European Commission Seventh Framework Programme FP7/2007–2013 [HEALTH-F2-2011-278913,[BiomarCaRE], the MORGAM Project is additionally funded by European Commission Seventh Framework Programme FP7/2007-2013 [HEALTH-F4-2007-2014113, ENGAGE and HEALTH-F3-2010-242244, CHANCES]. This has supported central coordination, workshops and part of the activities of the MORGAM Data Centre, at THL in Helsinki, Finland. FINRISK97 is mainly funded by budgetary funds of the THL-National Institute for Health and Welfare. VS was supported by the Finnish Foundation for Cardiovascular Research. MH was supported by funding from the Centre of Excellence for Public Health, Northern Ireland and the German Center for Cardiovascular Research (DZHK).
-
Competing interests SB has received research funding from Boehringer Ingelheim, Bayer, Abbott Diagnostics, SIEMENS, Thermo Fisher and Roche Diagnostics and received honoraria for lectures or consulting from Boehringer Ingelheim, Bayer, Roche, Astra Zeneca, SIEMENS, ThermoFisher and Abbott Diagnostics. No other authors have a relationship with Industry or a competing interest.
-
Ethics approval Coordinating Ethical Committee of the Helsinki and Uusimaa Hospital District.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement FINRISK is part of the MORGAM consortium and BiomarCaRE consortium, data can be shared between the consortium members upon committee discussion and approval.