Article Text

Abstract
Objective To test the hypothesis that risk factor pattern, treatment and prognosis differ between men and women with heart failure (HF) with and without diabetes in the Swedish Heart Failure Registry.
Methods Patients with (n=8809) and without (n=27 465) type 2 diabetes (T2DM) included in the Swedish Heart Failure Registry (2003–2011) were followed for mortality during a median follow-up of 1.9 years (range 0–8.7 years). All-cause mortality, differences in background and HF characteristics were analysed in women and men with and without T2DM and with a special regard to different age groups.
Results Of 36 274 patients, 24% had T2DM and 39% were women. In patients with T2DM, women were older than men (78 years vs 73 years), more frequently had hypertension, renal dysfunction and preserved ventricular function. Regardless of T2DM status, women with reduced ventricular function, compared with their male counterparts, were less frequently offered, for example, ACE inhibitors/angiotensin receptor II blockers (ARB). Absolute mortality was 48% in women with T2DM, 40% in women without; corresponding male mortality rates were 43% and 35%, respectively. Kaplan-Meier curves revealed shorter longevity in women with T2DM but female sex did not remain a significant mortality predictor following adjustment (OR 95% CI 0.90; 0.79 to 1.03). In those without T2DM, women compared with men lived longer; this pattern remained after adjustment (OR 0.72; 0.66 to 0.78). T2DM was a stronger predictor of mortality in women (OR 1.72; 1.53 to 1.94) than in men (OR 1.47; 1.34 to 1.61).
Conclusions T2DM is a strong mortality predictor in men and women with HF, somewhat stronger in women. The shorter survival time in women with T2DM and HF related to comorbidities rather than sex per se. Evidence-based management was less prevalent in women. Mechanisms behind these findings remain incompletely understood and need further attention.
Statistics from Altmetric.com
Introduction
In general women are protected from premature cardiovascular disease, but the presence of diabetes attenuates this characteristic.1 ,2 Thus women with diabetes suffer their first myocardial infarction at an age approaching that in men.3 Moreover, women with diabetes have an increased postinfarction mortality, which has been related to a high prevalence of heart failure (HF),4 ,5 in combination with an underuse of evidence-based management.6 The high prevalence of and poor prognosis after myocardial infarction in women with diabetes were first described in 1961 by Sievers et al,7 and in 1974, Kannel et al8 reported increased risk for future HF in women with diabetes based on the Framingham cohort. Since then the management of HF and diabetes has developed. Based on clinical trials it is obvious that, although still impaired, the longevity of patients with HF, including those with diabetes, has improved.9 ,10 However, clinical trials do not mirror everyday clinical practice recruiting proportionately healthier individuals and excluding those at high age causing a lower inclusion of patients with diabetes and of female sex making available information on sex differences in patients with HF contradictory. We hypothesised that sex influences the risk factor pattern, prescribed treatment and the vital prognosis in patients with HF to the disadvantage of women with diabetes and explored this through analyses of a contemporary, large and unselected HF population.
Material and methods
Source of data
The nationwide Swedish Heart Failure Registry (S-HFR) has been presented in detail.11 Registry information, the registration forms and annual reports are available at http://www.rikssvikt.se. Participating centres located at 65 hospitals and 113 outpatient clinics report to the registry, which in 2011 comprised information on 47 000 patients. The main inclusion criterion is a physician-judged diagnosis of HF and 76 variables are recorded via an internet-based case report form at hospital discharge or outpatient visits. Data are entered into a database managed by the Uppsala Clinical Research Center (Uppsala, Sweden) and run against the Swedish Population Registry using the unique ten-digit personal identification number of each Swedish citizen.
Study population
The present study addresses patients registered at hospital-based (68%) and specialised outpatient (32%) HF clinics during January 2003–September 2011 (n=36 595). Sex information was obtained from the Swedish personal identification number. Following exclusion of patients with incomplete information on sex (n=53) or glycaemic state (n=123) and with type 1 diabetes (n=198), the population consisted of 36 274 individuals, of whom 14 297 (39%) were women and 21 977 (61%) men; 8809 (24%; 37% women) had type 2 diabetes (T2DM) (figure 1). The main outcome variable was all-cause mortality, obtained by merging the S-HFR database with the Swedish Population Registry. The last day of follow-up was September 13, 2011.

Flow diagram for the total cohort (left panel) and for the separate cohorts including the age-matched subcohorts (right panel); (1) men and women with T2DM; (2) women±T2DM and (3) men±T2DM. In the right panel, the figure indications refer to the Kaplan-Meier survival curves for each group. T2DM, type 2 diabetes. Included—, Excluded-----.
Definitions
A description of definitions used in the S-HFR is reported in online supplementary appendix A. Heart failure: diagnosed by the attending physician based on guideline recommendations at the time of inclusion. New York Heart Association (NYHA) classes I to IV were used to express HF severity. Presence of ischaemic, valvular or hypertensive heart disease, as well as idiopathic dilated cardiomyopathy, was recorded. Ischaemic heart disease (IHD): was grouped as verified/not verified by coronary angiography, according to the physician-based classification. Type 2 diabetes: defined as a history of this diagnosis combined with treatment (lifestyle advice, oral glucose-lowering drugs and/or insulin). Revascularisation: implied a history of coronary artery bypass surgery and/or a percutaneous coronary intervention. Hypertension: based on case history or ongoing blood pressure-lowering therapy. LVEF: the most recent estimated LVEF (optional method) grouped into four different classes: ≥50%, 40–50%, 30–39% and <30%. Estimated glomerular filtration rate (eGFR): using the Cockcroft-Gault formula: eGFR (mL/min)=((140−age)×weight×1.23×(0.85 if female))/creatine (μmol/L).12
The completeness of reported data for the total cohort including number missing are detailed in online supplementary appendices B and C. Blood samples were analysed at the local chemical laboratories.
Statistical methods and data management
Statistical comparisons of sex differences between independent groups, for example, patients with and without T2DM, were performed using Student's t test for continuous variables. Quantitative, normally distributed variables are presented as the mean (SD) and 95% CIs. Non-normally distributed variables were logarithmically transformed prior to the t test. When appropriate, values are presented as the median, range and 95% CI. Categorical variables are presented as counts and proportions (%) and compared using the χ2 test. Statistical differences for all-cause mortality by T2DM status, sex and age group (≤65 years, 66–80 years and >80 years) were estimated using the logrank test, while survival curves were produced using Kaplan-Meier analyses. Due to low numbers at risk in the last years of follow-up, the Kaplan-Meier curves were truncated at 6 years. A formal test for interaction between mortality, sex and T2DM did not reveal any overall interaction (p=0.74). Still sex aspects were further evaluated for the three defined age groups and additional comparisons performed between the following three groups: (1) men and women with T2DM; (2) women±T2DM; (3) men±T2DM (figure 1). In the total population, multivariate logistic regression models were used to evaluate the importance of sex and T2DM as predictors of all-cause mortality. Variables adjusted for had fewer than 5% missing data reported and a univariate p value of <0.05, apart from LVEF included in the model despite missing information in 20% of the study population. They included age, sex, level of care, duration of HF, LVEF, blood pressure, T2DM, IHD, hypertension, atrial fibrillation, pulmonary disease, revascularisation, valvular surgery, eGFR class, haemoglobin class, weight, ACE inhibitors (ACEi), angiotensin receptor II blockers (ARBs), β-blockers, mineralocorticoid receptor antagonists, diuretics, digitalis, nitrates, statins and antithrombotic agents.
To further explore age as a confounder, three age-matched (±1 year) subcohorts were constructed as detailed in figure 1: (1) men and women with T2DM (n=6452; mean age 76.2 years vs 77.1 years); (2) women by T2DM status (n=6582; mean age 77.5 years vs 76.5 years in those with and without T2DM, respectively); (3) men by T2DM status (n=11 036; 72.6 years vs 71.6 years in those with and without T2DM). Univariable and multivariable OR estimations were calculated in each of the separate groups described above (men and women with T2DM; women±T2DM; and men±T2DM) as well as in the age-matched subgroups applying the same logistic regression model as previously described apart from that sex and diabetes were excluded in the respective groups. Age was excluded in the age-matched subgroups.
All analyses were carried out using the SAS system (version 9.3) and the 5%, 1% and 0.1% levels of significance were considered.
Ethical consideration
The establishment of the S-HFR and registration and data analyses in the S-HFR was approved by the Swedish National Board of Health and Welfare and the Swedish Data Inspection Board. The registry and this study conform to the Declaration of Helsinki. Individual patient consent is not required. Patients are informed on their entry and may opt out. The Regional Ethical Review Board at Linköping University approved the merging of the S-HFR with the Swedish Population Registry.
Results
Comparison of the total cohort
The clinical characteristics of patients by sex and T2DM status are presented in table 1. The mean age of the entire cohort was 75.0 years and 39% were women, who in general were older than men. The female proportion was lower at ages ≤65 years regardless of the presence or absence of T2DM. Figure 1 describes the number of patients by sex and T2DM status. The prevalence of T2DM was similar among women and men (23% vs 24%). Table 2 outlines baseline characteristics and pharmacological HF treatment by age group, sex and T2DM status. The prescription of diuretics was most frequent in women with T2DM (91%) while, compared with men, women received less β-blockade, ACEi/ARBs and statins (table 1). The pattern of less frequently prescribed ACEi/ARBs was only seen in women with T2DM and an LVEF <50%. Women without T2DM were less often given ACEi/ARB irrespective of LVEF.
Baseline characteristics and treatment divided by sex and T2DM status
Baseline characteristics and pharmacological treatment by T2DM and sex in different age groups
Comparison of men and women with T2DM
Among patients with T2DM women were older than men (77.5 years vs 72.6 years) but had a similar duration of HF and did not differ regarding NYHA classes. Hypertension (63% vs 58%), reduced renal function (eGFR 55 mL/min vs 70 mL/min) and a LVEF ≥50% (33% vs 16%) were more frequent in women. IHD was more common in men (62% vs 54%) who more often had been revascularised (38% vs 23%) and more commonly had a severely compromised ventricular function (LVEF <30%; 35% vs 21%). However, in the age group ≤65 years IHD and hypertension were similar in women and men (49% vs 52% and 58% vs 57%, respectively) (table 2). Regarding pharmacological treatment, women more likely received diuretics, while men received ACEi/ARBs and β-blockers to a greater extent (table 1).
Comparison of women with and without T2DM
Women with and without T2DM were of similar age (78.5 years vs 77.5 years). Patients with T2DM were heavier (76 kg vs 67 kg), had a longer duration of HF, were more frequently in NYHA classes III and IV (51% vs 43%) and had a higher mean N-terminal fragment pro brain natriuretic peptide (NT-proBNP) (3.49 pg/mL vs 3.46 pg/mL). Further, IHD (54% vs 40%), hypertension (63% vs 48%) and revascularisation (23% vs 13%) were more frequent among women with T2DM. In the age group ≤65 years, IHD was twice as common in those with T2DM (49% vs 23%) and a similar pattern was seen regarding hypertension (58% vs 31%). eGFR and LVEF were similar except that a larger proportion of patients with T2DM <80 years had an LVEF ≥50% (table 2). Diuretics and ACEi/ARBs were prescribed more frequently to women with T2DM than to those without (table 1).
Comparison of men with and without T2DM
The mean ages in men with and without T2DM were 72.6 years and 72.9 years, respectively. Men with T2DM were heavier (89 kg vs 81 kg), had a longer duration of HF and were more often in NYHA classes III and IV (50% vs 40%). Regardless of age group, IHD (62% vs 49%) and hypertension (58% vs 40%) were more frequent in men with T2DM, as was previous revascularisation (38% vs 28%), while LVEF, eGFR and NT-proBNP did not differ from the levels in men without T2DM. Men with T2DM received somewhat more extensive pharmacological HF treatment than men without this disease (table 1).
Mortality
The median follow-up time was 1.9 years (range 0–8.7 years). Absolute mortality was 48% in women with T2DM, 40% in women without; the corresponding male mortality rates were 43% and 35%, respectively. Survival was significantly lower in patients with T2DM, particularly in women, who had a median survival time of 3.1 years (95% CI 2.9 to 3.3) compared with 3.7 years (3.5 to 3.9) in men with T2DM and 4.0 years (3.8 to 4.1) and 5.0 years (4.8 to 5.3) in women and men without T2DM, respectively (p<0.0001). The Kaplan-Meier curves for the total cohort (figure 2) reveal that women with T2DM have the poorest prognosis, but this pattern was no longer present in survival curves at different age groups (figure 3A–C) and in the age-matched T2DM cohorts (figure 4B, D, F), pointing to a survival disadvantage for patients with T2DM regardless of sex. In univariable and multivariable analyses performed in the total cohort, T2DM independently predicted mortality in patients with HF before and after adjustment: OR 1.37 (1.31 to 1.44; p<0.0001) and 1.59 (1.48 to 1.71; p<0.0001), whereas female sex was not an independent predictor of mortality in patients with HF after adjustment: OR 1.23 (1.19 to 1.29; p<0.0001) and adjusted OR 0.78 (0.73 to 0.84; p<0.0001). This pattern applied regardless of level of care.

Survival in patients with heart failure by sex (Men=M, Women=W) and the presence or not of type 2 diabetes (T2DM) in the total study population.
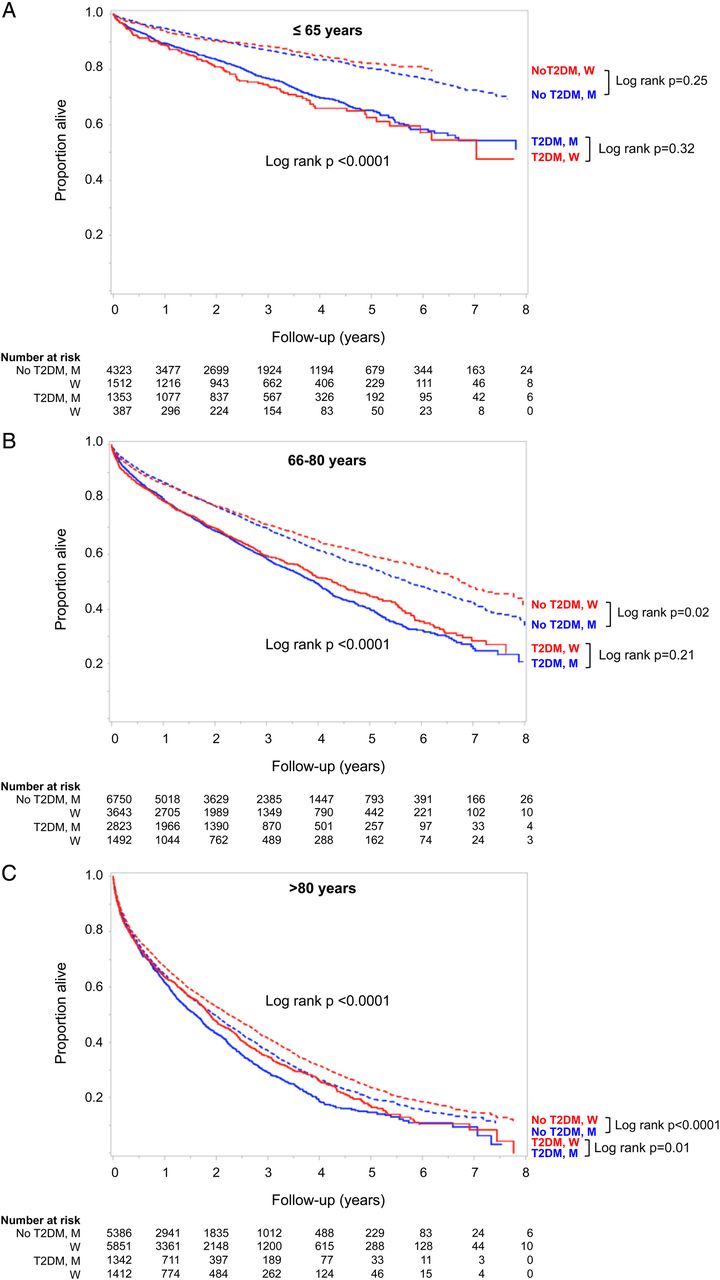
Survival by sex (Men=M, Women=W), type 2 diabetes (T2DM) status and age group in (A) patients below 65 years, log rank (overall p<0.0001, T2DM p=0.32 and no T2DM p=0.25), (B) patients 66–80 years, log rank (overall p<0.0001, T2DM p=0.21 and no T2DM p=0.02) and (C) patients above the age of 80 years, log rank (overall p<0.0001, T2DM 0.01 and no T2DM p<0.0001).

Survival in (A) patients with type 2 diabetes (T2DM) in the total cohort and in (B) the age-matched T2DM cohort. Survival in women (W) by T2DM in (C) all women in the total cohort and (D) in the matched female subcohort and survival in men (M) by T2DM in (E) all men in the total cohort and (F) in the age-matched male subcohort.
The Kaplan-Meier curves in the age-matched cohorts reveal that, within the age-matched T2DM group, there was no difference in survival between men and women (logrank p=0.08; figure 4B). Women with T2DM compared with those without had reduced longevity (figure 4D). A similar pattern, albeit somewhat less pronounced, was seen in men (figure 4F).
The Forest plot in figure 5 presents unadjusted and adjusted associations of sex, T2DM and mortality. In women and men without T2DM the unadjusted and adjusted ORs (95% CI) for mortality were 1.25 (0.19 to 1.32; p<0.0001) and 0.72 (0.66 to 0.78; p<0.0001). In those with T2DM unadjusted and adjusted ORs were 1.23 (1.13 to 1.34; p<0.0001). Following adjustment, female sex did not remain an independent predictor of mortality among all patients with T2DM and HF (OR: 0.90:0.79 to 1.03; p=14) or in the age-matched T2DM group (OR; 0.92; 0.79 to 1.06; p=0.25). T2DM was an independent predictor of mortality in women with HF, increasing from 1.37 (1.27 to 1.48; p<0.0001) to 1.72 (1.53 to 1.94; p<0.0001) after extensive adjustments. Comparing men with and without T2DM, the unadjusted OR was 1.39 (1.31 to 1.48; p<0.0001), increasing to 1.47 (1.34 to 1.61; p<0.0001) after adjustment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Unadjusted and adjusted associations between sex and mortality in (A) the entire population without type 2 diabetes (T2DM) and in (B) in the entire population with T2DM and in an age-matched subcohort, (C) unadjusted and adjusted associations between T2DM and mortality in women and (D) in men in the total cohort and for women and men sex-specific, age-matched subcohorts. *Adjusted for: age, sex, level of care, duration of HF, LVEF, blood pressure, T2DM, IHD, hypertension, atrial fibrillation, pulmonary disease, revascularisation, valvular surgery, eGFR class, Hb class, weight, angiotensin converting enzyme inhibitors (ACEi), angiotensin receptor II blockers (ARB), beta-blockers, mineralocorticoid receptor antagonists, diuretics, digitalis, nitrates, statins and antithrombotic agents. **Adjustments as in * but with T2DM instead of gender. †Age not included in the multivariable model.
Discussion
The main finding in this large unselected HF population is that neither female nor male sex independently predicts mortality in patients with T2DM and HF while T2DM is an independent risk factor of mortality regardless of sex.
Women with HF generally have a survival advantage over men,13–16 supported by the present data when it comes to those without T2DM in whom female sex was protective. The current analysis shows that T2DM attenuates this protection. This matches observations in the meta-analysis by Martinez-Selles et al,17 extending them from populations derived from clinical trials to patients in everyday practice. T2DM was a strong risk factor for adverse prognosis in both sexes, although it imposed a slightly stronger mortality risk on women compared with men. This was further illustrated in the age-matched analyses, and by the risk increase related to T2DM (1.72 in women, 1.47 in men).
The shorter survival time in women with T2DM related to concomitant risk factors, including higher age and more frequently reduced renal function. These data are in line with previous reports on myocardial infarction, indicating no adverse relationship with female sex in itself but rather related to comorbidities, for example, hypertension, HF and renal dysfunction.4 Women with HF and T2DM were older than men and their LVEF more frequently preserved. This is consistent with contemporary population-based HF registries and reasonably reflects the situation for women with HF in general.6 ,18 ,19 One main difference, revealed by comparing women with and without T2DM, was that women with T2DM more frequently had IHD, in fact even more apparent at ages ≤65 years, where IHD was twice as common. In this context women with T2DM had a ‘male-like’ risk factor profile.
Data presented from our group reveal IHD as a common risk factor and important predictor of mortality in patients with T2DM and HF.20 Moreover, our findings indicate an underutilisation of coronary angiography and revascularisation, especially among patients with T2DM. The present analyses confirm that this pattern applies, regardless of sex.
Women with T2DM and reduced LVEF were prescribed fewer ACEi/ARBs and more diuretics and the most comprehensive use of evidence-based treatment was seen in men with T2DM, regardless of age group. This may partially be explained by reduced renal function and precautions taken due to higher age in women, but a subconscious sex-based difference in management cannot be ruled out. This might also explain the lower number of women compared with men undergoing revascularisation. Previous reports of sex-related differences regarding evidence-based treatment are contradictory, some are in line with our findings, that is, women receiving less of modern treatment,6 ,21 ,22 others report no such pattern.19 ,23 ,24
One of the sex differences revealed by this study is that, regardless of T2DM, women more frequently had a preserved LVEF. Women also had higher NT-proBNP, with the highest mean level seen in those with T2DM. Since echocardiography is somewhat blunt when examining LVEF, it would be of interest to use more sophisticated cardiac imaging techniques, such as MRI, to detect myocardial effects caused by, for example, hyperglycaemia.
Strengths and limitations
The main strength is the large, representative patient cohort from everyday practice allowing age-matched and sex-matched analyses and adjustments for many confounders. Individuals were included from specialist care, possibly introducing a selection bias, especially since previous studies have reported that women and patients with preserved LVEF are often managed in primary care.25 We have not adjusted evidence-based treatment for important confounders mainly due to a lack of detailed information on treatment indications. Another limitation is the lack of information on LVEF and treatment after the index event. Unfortunately information on T2DM duration, important for all-cause mortality, was unavailable. Moreover, some pertinent variables were not consistently available. This can explain the widening CIs seen after adjustments, but should reasonably not change the main conclusions. Lastly, the follow-up time may be considered short. It should, however, be noted that the range is 0–8.7 years implicating that the Kaplan-Meier curves express outcome during a fairly long period (truncated at 6 years). The short median survival time is reasonably influenced by a poor life expectancy in patients with HF and a larger proportion of the patients being included during the latter years of the studied period as an effect of a registry in constant growth.
Conclusion
T2DM is a strong risk factor of mortality in patients with HF of similar magnitude in men and women. The present data indicate that the impaired survival in women with T2DM and HF relates to comorbidities such as hypertension and IHD and potentially less than optimal management rather than sex in itself. Especially in the age group ≤65 years, the risk factor pattern differs between women with and without T2DM, with the latter presenting with a more ‘male-like profile’.
Key messages
What is already known on this subject?
Patients with diabetes, especially women, run an increased risk of developing heart failure (HF) but whether they also have a poorer life expectancy than their male counterparts is not clearly established. Previous reports are often dated and based on selected populations with a low proportion of women and patients with diabetes.
What might this study add?
The Swedish Heart Failure Registry enables a detailed analysis of the vital prognosis in less selected patients with HF. Type 2 diabetes (T2DM) is a strong and independent risk factor of mortality in women and men increasing the mortality risk by 70% and 50%, respectively. The more dismal prognosis seen in women relates to associated risk factors rather than female sex itself.
How might this impact on clinical practice?
This report should increase the awareness that T2DM compromises the vital prognosis in women with HF, seemingly related to a ‘male-like’ cardiovascular risk factor profile already at younger ages (<65 years). This should increase the efforts to improve investigation and treatment of this vulnerable group.
References
Supplementary materials
Footnotes
Contributors All authors have made substantial contribution to this paper. IJ and AN developed the study concept and design and all authors (IJ, LR, ME, UD, PN and AN) took part in the analysis and interpretation of the results. ME obtained the database from Uppsala Clinical Research Centre. IJ managed and analysed the data, performed the statistical analyses and took main responsibility for putting the report together. PN provided supervision and support within the frames of statistical analyses performed by IJ. IJ and AN finalised the manuscript after adjustments from all the authors. All authors have read and approved the final version of the manuscript.
Funding Unrestricted grants from The Swedish Heart-Lung Foundation. The regional agreement on medical training and clinical research (ALF) between Stockholm County Council and the Karolinska Institute, the Swedish Heart Failure Registry steering group, the Swedish Diabetes Foundation supported this work.
Competing interests None declared.
Ethics approval The Regional Ethical Review Board at Linköping University.
Provenance and peer review Not commissioned; externally peer reviewed.