Article Text

Abstract
Aims Previous cohort studies of patients with coarctation of the aorta (CoA) demonstrate reduced long-term survival. Improved surgical outcomes in children and evolution of adult congenital heart disease (ACHD) services have resulted in improved survival in patients with other CHDs. We hypothesise that for young adult patients with CoA long-term outcomes have improved in the contemporary era.
Methods 151 patients (58% men) with simple CoA followed up at a tertiary ACHD service in Sydney, Australia, from 1993 to 2013 were included. We documented mortality and major morbidity such as the need for re-intervention for re-coarctation or aneurysms.
Results 140 patients (mean age 35±15 years) underwent CoA repair at median age of 5 (IQR 0–10) years. Initial surgical strategy included end-to-end repair in 43, subclavian flap aortoplasty in 28 and patch aortoplasty in 31 patients (and was not documented in 28 cases). 6 patients had endovascular repair, 4 had interposition tube grafts and 11 were unrepaired. There were a total of seven deaths at a median age of 60 years. Actuarial survival was 98% at 40, 98% at 50 and 89% at 60 years of age. Re-coarctation occurred in 34% and descending aortic aneurysms were noted in 18%. Patients with end-to-end repair had lower rates of significant re-coarctation or descending aortic aneurysms (p=0.026 and <0.001, respectively). 66% had bicuspid aortic valve and 44% were hypertensive.
Conclusions Patients with CoA who reach adolescence demonstrate very good long-term survival up to age 60 years. Long-term morbidity is common, however, related largely to aortic complications and late hypertension.
Statistics from Altmetric.com
Introduction
Since the first coarctation repair in 1944,1 surgical techniques have evolved, aiming to reduce early and late mortality as well as minimise long-term sequelae such as re-coarctation and late aneurysms. Recognition of complications from specific surgical repair types (eg, local aneurysm formation following Dacron patch aortoplasty (PA)2–5) has led to increased surveillance that has been incorporated into recommended clinical practice.6
Although coarctation of the aorta (CoA) appears to be a conceptually simple lesion, long-term management is complex, related to associated valvulopathy, vasculopathy,7 ventricular dysfunction, long-term hypertension,8 ,9 cerebrovascular disease10 and operative site complications. Studies from the 1980s describing long-term survival in adults with CoA reported a median age at death of 38 years.11
In developed countries, there are now more adults than children with congenital heart disease (CHD).12 Accordingly, specialist adult congenital heart disease (ACHD) centres have been established. CoA, with a prevalence of 5–8% of all CHD,6 comprises one of the commonest patient groups referred for evaluation. We thus sought to determine long-term survival patterns of adults with CoA in the contemporary era, who are followed up at a tertiary-level ACHD centre. We also aimed to describe the patterns of ongoing morbidity including aortic re-coarctation or aneurysms and hypertension to improve understanding of the outlook for patients with CoA who survive beyond adolescence.
Methods
A single-centre study was performed involving a specialised ACHD referral centre in Sydney, Australia. Established in the early 1990s, this is the only centre state-wide with a referral ‘catchment area’ of 6–7 million people. Patients presenting to this service above age 16 years, seen at least once between 1993 and 2013 with ‘simple’ CoA (defined as having no associated CHD except bicuspid aortic valve (BAV), persistent ductus arteriosus or small atrial or ventricular septal defects (VSDs) not requiring repair) were included. Forty-one patients with CoA in conjunction with other complex CHD were excluded (figure 1). These included double-inlet LV in 2, double-outlet RV in 2, Eisenmenger's syndrome due to unrepaired VSD in 1, subaortic stenosis in 8, atrioventricular canal defect in 1, VSD requiring surgery in 15, Shone's complex in 2 and mitral valve abnormalities requiring repair in 5 patients. One patient had anomalous pulmonary venous drainage and a coronary to pulmonary artery fistula was present in one patient, requiring repair. Patients with significant non-cardiac disease were excluded, as were those with hypoplasia of the transverse aortic arch (defined as having a diameter of <50% that of the ascending aorta13). Three excluded patients had a hypoplastic aortic arch, one with Shone's syndrome and two with repaired VSDs. Two patients had significant intellectual impairment, which influenced the management of their CHD and were therefore excluded.

Flow chart showing patient recruitment process including numbers of patients excluded due to more complex congenital heart disease. CHD, congenital heart disease; CoA, coarctation of the aorta.
Clinical data were retrospectively obtained, including details of initial surgical repair (age, type, perioperative complications and details regarding associated CHD). Of the 140 repaired CoA patients in this study, initial surgical repair was known in 112 patients. In 28 patients, old operation reports could not be obtained from patient records.
The National Death Index (NDI) registry was accessed to document the vital status of all patients. Thus, survival data were calculated from knowledge of vital status of all subjects at the time of accessing the NDI. Further details regarding cause of death were obtained by consulting medical records, death certificates or autopsy reports. Late morbidities including repeat cardiac surgery, re-coarctation, aortic aneurysms and hypertension were also noted. Mortality was the primary outcome measure, and incidence of re-coarctation, aneurysm, hypertension and need for intervention for re-coarctation and/or aneurysm formation were pre-specified secondary outcome measures. Long-term morbidity referred to the presence of secondary outcome measures or aortic valve disease.
Our centre follows standard ACHD protocols. Patients with CoA are reviewed every 1–2 years based on symptoms and complexity. Aortic screening by echocardiography is performed at each visit in addition to clinical examination and ECG. Asymptomatic patients are not screened for intracranial aneurysms. Descending aortic complications are further assessed at regular intervals using MRI or CT scanning depending on clinical and echocardiographic findings, repair type and evidence of interval change.
Hypertension was defined as a blood pressure of >140/90 mm Hg on two separate occasions14 at rest, a systolic blood pressure of >220 mm Hg at peak exercise during a standardised exercise stress test15 or the need for antihypertensive medications. Re-coarctation was defined as having hypertension and a resting blood pressure gradient ≥20 mm Hg between right arm and leg,6 transverse aortic arch/diaphragmatic aorta ratio <0.7 or site of repair/diaphragmatic aorta ratio <0.7 at MRI.16 Re-coarctation was considered significant if it required percutaneous or surgical repair. Aneurysm formation was defined by a ratio of the aortic dimension at the repair site to the aortic dimension at the diaphragmatic aorta of >1.517 on cardiac MRI, requiring surgery, or on an autopsy report.
Statistical analysis
Statistical analysis was performed using SPSS V.20 (IBM, Armonk, New York, USA). Actuarial survival was assessed using Kaplan–Meier survival methods. The Mantel–Cox log-rank test was used to compare multiple survival curves. Differences between two continuous variables were assessed using independent t tests, and categorical variables were assessed using Fisher's exact tests. Analysis of variance tests were used to assess differences between more than two groups. Correlations were assessed using bivariate models by Pearson's method. A two-tailed value of p<0.05 was considered statistically significant.
Results
Patient characteristics
A total of 151 patients with simple CoA were identified. All patients (58% men) attended our ACHD centre at least once over the age of 16 years in the past 20 years (1993–2013), with mean age at last follow-up of 35±15 years. The median age at surgery was 60 months (IQR 2–120 months). The median year at surgery was 1989 (IQR 1980–1996). Patients were followed up for a mean total period of 26±13 years after surgical repair.
The initial repair strategy was end-to-end anastomosis (EEA) in 43, subclavian flap aortoplasty (SFA) in 28, PA in 31, interposition tube graft in 4 and percutaneous repair in 6 patients (table 1). Surgical repair strategy was unknown in 28 patients, and 11 patients were unrepaired. There was no significant difference in age at repair comparing the surgical strategies (p=0.09). Associated CHD included atrial septal defects in 2%, dysplastic tri-leaflet aortic valves in 2%, VSDs in 4% and persistent ductus arteriosus in 5%.
Initial surgical repair strategy and long-term complications
Long-term survival
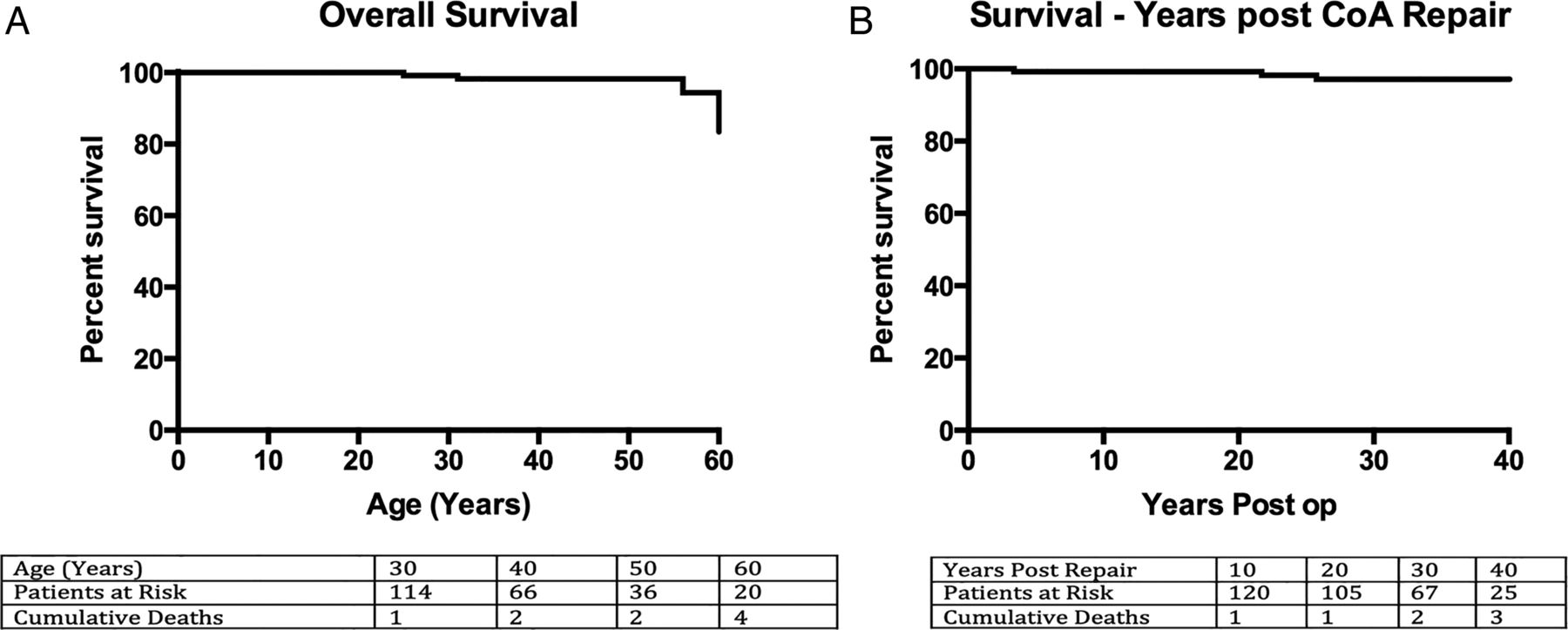
Overall survival in our cohort (ie, patients over age 16) was 98% to age 40, 98% to age 50 and 89% to age 60 years (figure 2).

Kaplan–Meier curve showing long-term survival in patients with coarctation of the aorta (CoA) repair. (A) Overall survival; (B) survival in years post-repair.
There were a total of seven deaths, at a median age of 59 (IQR 29–72) years. Two female patients had fatal intracranial haemorrhages, one aged 24 years and the second aged 67 years. The latter had mild re-coarctation. Neither of these patients had had prior cerebral vessel imaging as both were asymptomatic and normotensive. The third death was in a 30-year-old woman with prior SFA and Turner syndrome with an ascending aorta measuring 38 mm on cardiac MRI who suffered an acute type A aortic dissection. She was prescribed angiotensin receptor antagonists and calcium channel antagonists for hypertension, with good control. She had not been referred for surgical management as the aortic diameter did not warrant this and was therefore under surveillance with serial MRIs. There were three sudden cardiac deaths, one in a 56-year-old man with EEA aged 15 years who chose not to attend regular follow-up, with ascending aortic dilatation and hypertension. Non-occlusive atherosclerotic coronary disease was found on autopsy. The second was a 61-year-old woman with prior CoA repair of unknown type and mechanical aortic valve replacement who did not have an autopsy and the cause of death was undetermined. The third patient was a 60-year-old man who underwent a tissue aortic valve replacement for severe aortic stenosis 4 months prior to death. He had a prolonged postoperative course complicated by pericardial tamponade and sternal wound dehiscence requiring surgical repair. Infective endocarditis was the presumed cause of death. One patient died due to myocardial infarction aged 85 years with comorbidities including chronic renal failure and dementia. He had undergone percutaneous CoA repair 3 years prior to death.
Initial surgical repair strategy and long-term survival
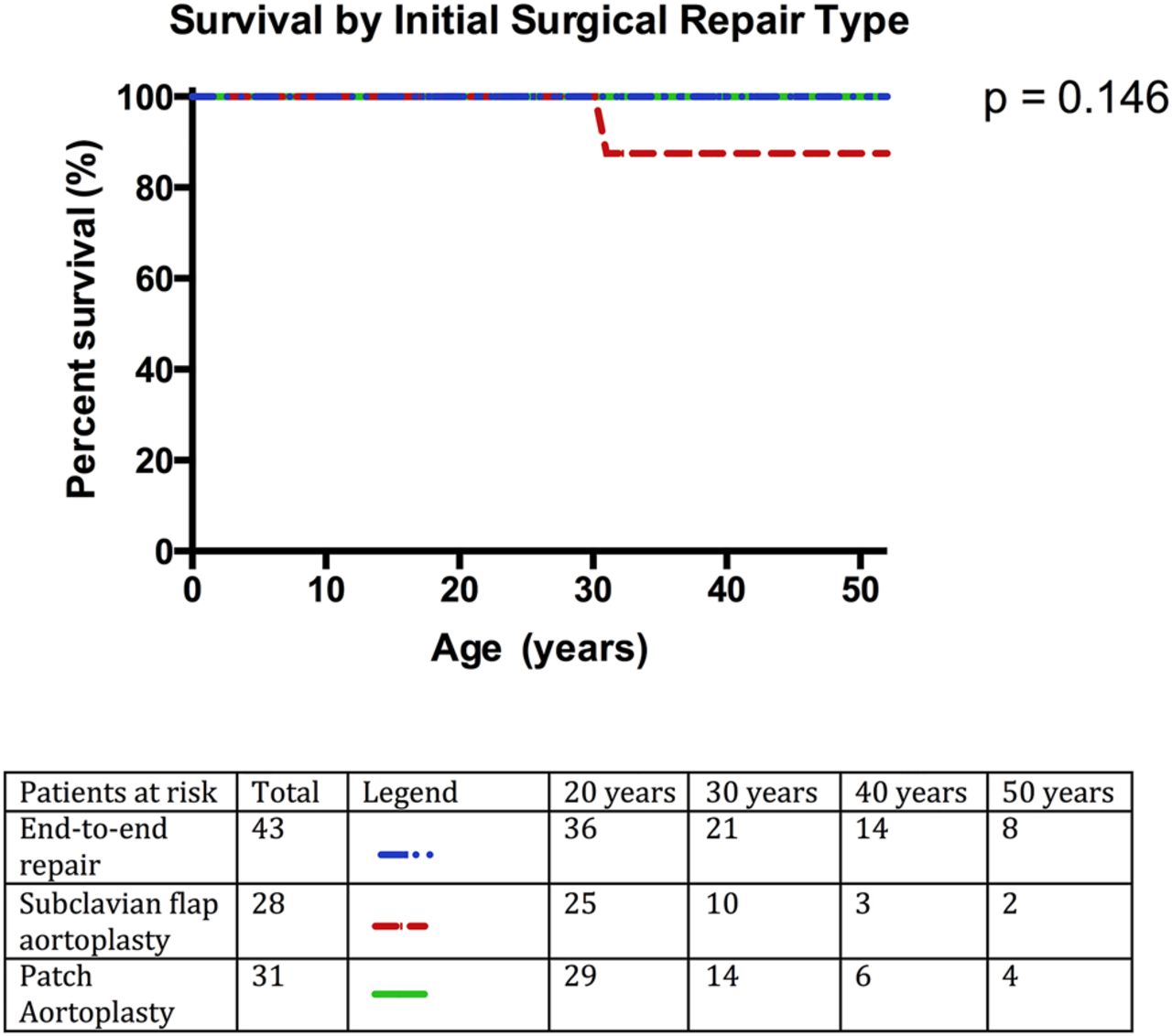
There was no significant difference in survival (p=0.146) or age at last follow-up comparing EEA, SFA and PA (p=0.33) (figure 3).
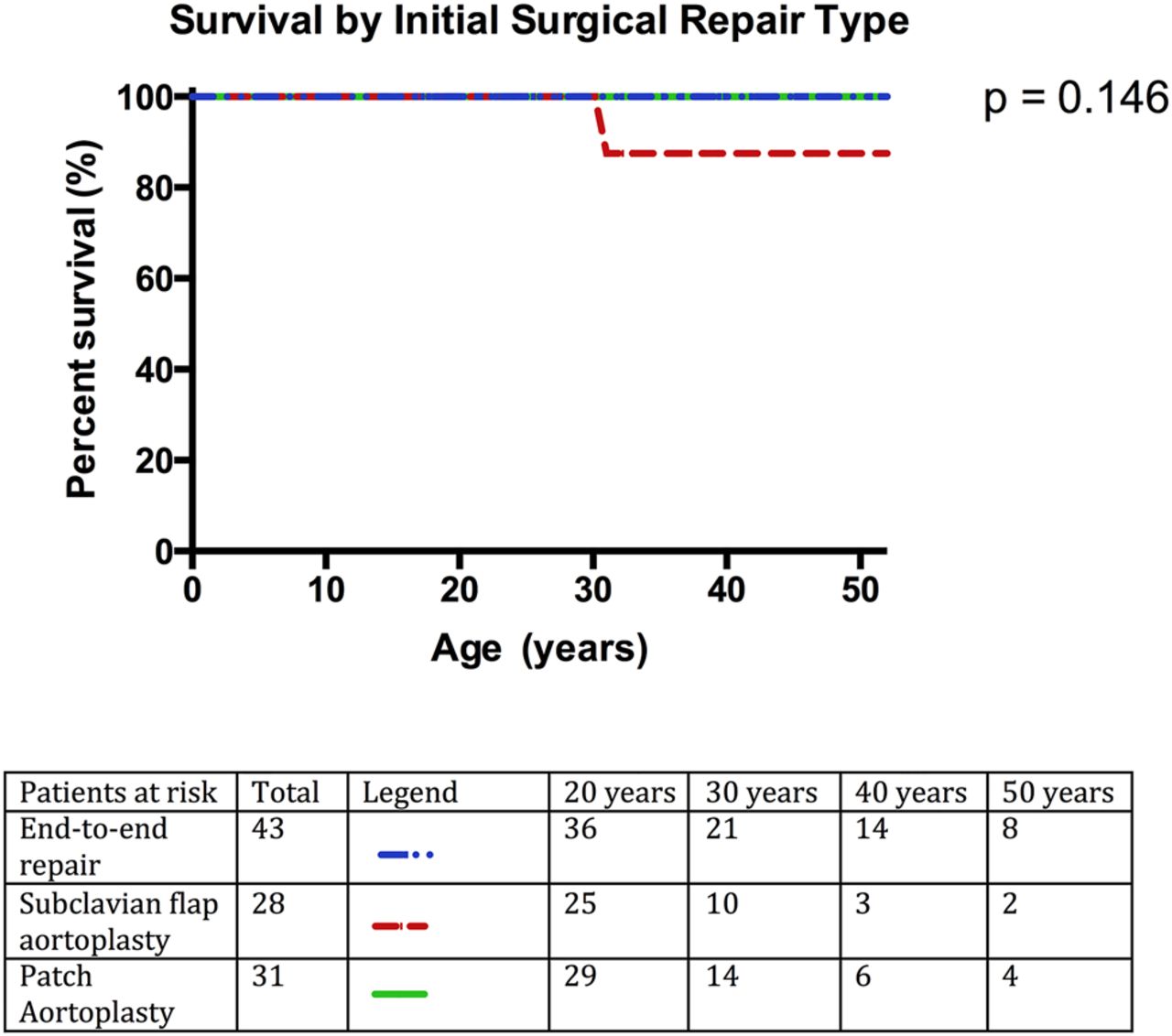
Kaplan–Meier curve showing long-term survival by type of initial surgical repair strategy.
Re-coarctation post-repair
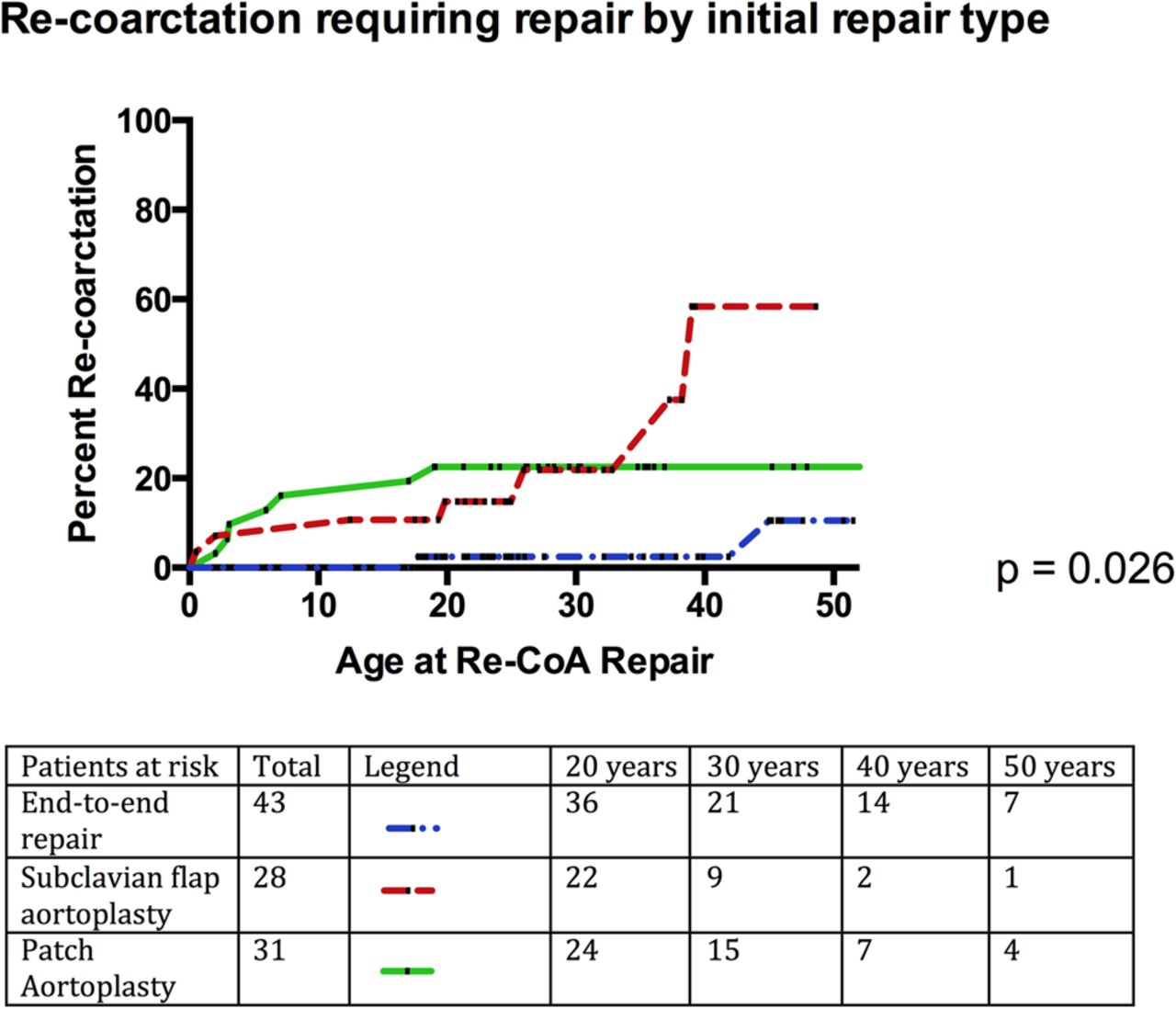
Re-coarctation occurred in 43 (31%) patients following CoA repair, requiring either surgical or percutaneous intervention in 18 patients. The prevalence of re-coarctation was 30% following EEA, 36% following SFA and in 42% after PA. Re-coarctation repair was required in 7%, 25% and 23%, respectively. Patients with EEA had a lower prevalence of significant re-coarctation compared with those undergoing SFA or PA (p=0.026) (figure 4). Patients with significant re-coarctation requiring repair were younger at their initial CoA surgery (age 2±4 years vs 6±6 years; p=0.029) compared with those without re-coarctation.

Incidence of significant re-coarctation following surgical repair of coarctation of the aorta (CoA) by initial surgical repair strategy.
Descending aortic aneurysm
Descending aortic aneurysms were noted in 23 patients with a prevalence of 2% in patients with EEA, 18% in patients with SFA, 42% in patients with PA and in none of those with interposition grafts or percutaneous repair. Surgical repair was necessary in 1 patient with EEA, 3 with prior SFA repair and 12 patients with prior PA repair. Patients with initial EEA repair had markedly lower rates of descending aortic aneurysms requiring intervention compared with those with initial SFA or PA (p<0.001). Indeed, the highest prevalence of descending aortic aneurysms was noted in patients with PA (figure 5).

Incidence of descending aortic aneurysms following surgical repair of coarctation of the aorta by initial surgical repair strategy.
Hypertension
A total of 63 patients (42%) were hypertensive. Hypertension was associated with later age at initial repair (median age 7 (IQR 0–17) years vs 4 (IQR 0–6) years, p=0.025). This was particularly noted in patients with prior EEA; median age 7 (IQR 0–17) years in hypertensive vs 4 (IQR 0–6) years in normotensive patients (p<0.001). Hypertension only modestly correlated with ascending aortic aneurysms (Pearson's r=0.206, p=0.02). Initial surgical repair strategy was not associated with late hypertension (44% EEA, 54% SFA and 42% of patients with PA, p=0.68).
Bicuspid aortic valve
BAV was present in 66% of patients with 5% requiring intervention on their aortic valve (aortic valve replacement in four patients, valvotomy in two and repair involving leaflet resuspension in one patient). The presence of BAV did not correlate with the presence of ascending aortic aneurysms (r=0.160, p=0.06). 6.1% of patients with BAV had ascending aortic aneurysms, three of whom required ascending aortic repair during aortic valve surgery. The presence of BAV did not correlate with death or future re-coarctation (p=0.77 and 0.57). There was also no correlation with need for repeat cardiac surgical procedures (r=0.15, p=0.08).
Event-free survival
A composite end-point of death or intervention for aortic aneurysms, re-coarctation or aortic valves was considered and time to death or re-intervention was determined. Event-free survival at age 30 was 83%, at age 40 was 77% and at age 50 was 63% with a median event-free survival of 60 years (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier curve showing the composite end-point of time to death or re-intervention for aneurysms or re-coarctation.
Discussion
In this contemporary series of 151 adults with CoA, we report long-term actuarial survival rates of 98% to age 40, 98% to age 50 and 89% to age 60 years with event-free survival up to 50 years in 63% of patients. However, our data also highlight a high incidence of late complications requiring careful surveillance and often needing intervention. Neither type of surgical strategy nor age at repair affected long-term survival. Earlier age at surgery, however, was associated with a lower prevalence of hypertension and a higher incidence of re-coarctation. Hypertension was prevalent in our cohort, and repeat procedures were frequently required for aortic valve and thoracic aortic complications.
Cohort studies of patients with CoA from three decades ago demonstrated a median age at death of 38 years, primarily related to premature cardiovascular disease.11 ,18–22 Subsequent studies highlight improved survival, but few studies report contemporary era survival from ACHD centres. Recent data by Brown et al21 showed an improved long-term survival (but still only 86% remained alive at 20 years post-repair). These data include patients from 1946 to 2005—an era with marked evolution of treatment, surgical strategy, postoperative care and long-term surveillance programmes. Infants and young children are also included, who have a significantly higher mortality related to perioperative events.22 Our study addresses those followed up into the contemporary era (1993–2013) and those who have successfully survived to age 16 years and have been evaluated at a specialised ACHD centre. Previous data have suggested improved long-term outcomes from specialised ACHD management in the setting of other lesions, such as tetralogy of Fallot.23
There are a number of possible contributors towards recent improvements in survival. Management of CHD has evolved considerably, particularly since the 1970s with marked changes in practice including prenatal diagnoses, early prostaglandin administration and early definitive repair. Improved perioperative care has resulted in reduced early postoperative mortality.22 It is important to note that our survival data only include patients who have survived to age 16 years and have transitioned to ACHD services. We therefore excluded patients with early postoperative mortality in childhood. We included patients repaired prior to 1980 as the main aim of the study was to assess long-term survival and cardiac morbidity in adulthood. Furthermore, recognition of cardiovascular morbidity in hypertensive patients has led to closer monitoring and institution of preventative strategies for vascular disease. Finally, adult congenital services have evolved in order to meet the long-term surveillance requirements of this group including earlier intervention where indicated for aortic complications, related to re-coarctation and descending aortic aneurysms.
Our data highlight the complexity of the patterns of morbidity in these subjects. Ongoing issues related to aortic aneurysms and re-coarctation underscore the importance of serial aortic imaging to ensure earlier management of potentially life-threatening complications. Canadian guidelines24 advocate periodic surveillance for aortic complications using cardiac MRI, substituted by CT if cardiac MRI is unavailable. Hypertension management is also critical, given the high prevalence of hypertension in our cohort and thus the predisposition towards premature coronary and cerebrovascular disease. Associated CHD such as BAV also contribute towards need for repeat cardiac surgery25 as well as the incidence of aortopathy, particularly involving the ascending aorta. The correlation between BAV and ascending aortic aneurysms was not statistically significant in our CoA cohort. This is possibly due to insufficient sample size due to the low incidence of ascending aortic aneurysms, with a high background prevalence of BAV.
The prevalence of intracranial aneurysms was low, although no specific screening was performed in our cohort. Curtis et al26 have reported a prevalence of intracerebral aneurysms of 10% with routine magnetic resonance angiography screening; however, only 0.3% of that population required intervention.
It is well recognised that coarctation repair does not signify ‘cure’27 and late cardiac morbidity due to occlusive coronary artery disease, redo coarctation procedures, aortic disease including aneurysms and/or dissection, cerebrovascular accidents, hypertension and aortic valve procedures can occur in up to 40% of patients, 30 years post-repair.9 ,11 ,19 ,25 ,28 Maintaining adequate long-term follow-up, although challenging, is important to ensure adequate surveillance for repair site aortic complications, cardiovascular risk reduction measures, management of associated CHD and assessment of intracranial vascular disease. We report improved overall as well as event-free survival rates (compared with previous publications), underscoring the importance of recognising and treating long-term sequelae, in a specialised ACHD tertiary referral setting.
Limitations
The main limitation of this study was the absence of detailed operation reports in 18% of our patients, most of whom had had operations in a remote location, due to the segregation of adult and paediatric services. Movement of patients across geographical areas, loss to long-term follow-up and management of patients outside the specialty centres add to this difficulty. However, we obtained comprehensive mortality data from the Australia-wide National Death Registry, ensuring that apart from deaths that may have happened outside the country we would have captured all the deaths in our cohort. Ideally, documenting the initial denominator of repaired coarctation and serial follow-up of patients nationwide would be beneficial, specifically to assess outcomes of those lost to follow-up. However, this is currently not available within the health service and our data thus reflect the current clinical setting with real-world limitations. Thus, our findings cannot be generalised to survivors of coarctation repair who do not attend regular specialist follow-up, into adult life.
Conclusions
In the contemporary era, patients with repaired CoA who reach adulthood and are managed by a specialist ACHD centre have very good long-term survival, even up to 40 years following initial repair. This occurs despite significant cardiovascular morbidity related to re-coarctation, descending aortic aneurysms, hypertension and need for repeat procedures related to associated CHD, most commonly, BAV. Such favourable outcomes prompt a cautious optimism regarding long-term prognosis in this cohort; however, close surveillance for the recognised morbidities suggests the need for maintaining lifelong follow-up of these patients at a specialised ACHD centre.
Key messages
What is already known on this subject?
Coarctation of the aorta (CoA) is one of the commonest congenital lesions presenting to adult cardiologists. Previous data demonstrate reduced long-term survival for patients with CoA repair. Improved paediatric surgical outcomes and evolution of adult congenital heart disease (ACHD) services have resulted in improved survival in patients with other CHD such as tetralogy of Fallot.
What might this study add?
Our data demonstrate very good medium-term to long-term survival in patients with repaired CoA who maintain follow-up with a specialised ACHD service. Actuarial survival was 98% at 40, 98% at 50 and 89% at 60 years of age. Re-coarctation requiring re-intervention occurred in 34% and descending aortic aneurysms occurred in 18%. Patients with initial end-to-end repair had significantly lower rates of re-intervention for re-coarctation or descending aortic aneurysms compared with other surgical strategies. Older age at initial repair was significantly associated with hypertension, particularly in patients undergoing end-to-end repair.
How might this impact on clinical practice?
Clinicians managing patients with CoA need to maintain long-term surveillance for aortic complications, particularly for re-coarctation or descending aortic aneurysms. Management of hypertension and associated aortic valve disease is also important, considering the pattern of long-term morbidity.
References
Footnotes
Contributors All the authors fulfil relevant criteria for authorship regarding design, analysis, interpretation, drafting, revision and approval of the study and the manuscript.
Funding PC was supported by the National Health and Medical Research Committee & National Heart Foundation Postgraduate Scholarship no. 1055773.
Competing interests None.
Ethics approval Royal Prince Alfred Hospital Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.