Article Text

Abstract
Objectives Mitral regurgitation (MR) is a common entity in patients with aortic stenosis undergoing transcatheter aortic valve replacement (TAVR), but its influence on outcomes remains controversial. The purpose of this meta-analysis was to assess the clinical impact of and changes in significant (moderate–severe) MR in patients undergoing TAVR, overall and according to valve design (self-expandable (SEV) vs balloon-expandable (BEV)).
Methods All national registries and randomised trials were pooled using meta-analytical guidelines to establish the impact of moderate–severe MR on mortality after TAVR. Studies reporting changes in MR after TAVR on an individual level were electronically searched and used for the analysis.
Results Eight studies including 8015 patients (SEV: 3474 patients; BEV: 4492 patients) were included in the analysis. The overall 30-day and 1-year mortality was increased in patients with significant MR (OR 1.49, 95% CI 1.16 to 1.92; HR 1.32, 95% CI 1.12 to 1.55, respectively), but a significant heterogeneity across studies was observed (p<0.05). The impact of MR on mortality was not different between SEV and BEV in meta-regression analysis for 30-day (p=0.360) and 1-year (p=0.388) mortality. Changes in MR over time were evaluated in nine studies including 1278 patients. Moderate–severe MR (SEV: 326 patients; BEV: 192 patients) improved in 50.5% of the patients at a median follow-up of 180 (30–360) days after TAVR, and the degree of improvement was greater in patients who had received a BEV (66.7% vs 40.8% in the SEV group, p=0.001).
Conclusions Concomitant moderate–severe MR was associated with increased early and late mortality following TAVR. A significant improvement in MR severity was detected in half of the patients following TAVR, and the degree of improvement was greater in those patients who had received a BEV.
Statistics from Altmetric.com
Introduction
Mitral regurgitation (MR) is the most frequent valvular heart disease1 and is frequently associated with severe aortic stenosis (AS), ranging from 3% to 74%, in elderly patients undergoing surgical aortic valve replacement (SAVR) or transcatheter aortic valve replacement (TAVR).2 In the presence of both, severe MR and AS, a double valve intervention is generally indicated. Moreover, a recent meta-analysis showed that even moderate MR left untreated during SAVR may be associated with poorer early and late outcomes,3 suggesting that double-valve surgery may be justified in such cases despite the higher perioperative mortality associated with such operations.4
TAVR has been shown to be a non-inferior or even a superior alternative to SAVR in patients with severe AS and a high-risk profile.5–7 However, significant (moderate or severe) MR is present in ∼15% of patients undergoing TAVR and in this setting MR is usually left untreated.2 It is therefore of utmost importance to determine the clinical impact of and changes in MR in patients undergoing TAVR; this may have important implications in the clinical decision-making process for patients with AS eligible for either TAVR or SAVR. The impact of concomitant MR on clinical outcomes has been arbitrarily reported in single-centre and multicentre TAVR series, but no systematic analysis of large series has been performed to date. Moreover, two recent large studies, with different transcatheter valves, reported contradictory results.8 ,9 Thus, it has been hypothesised that self-expandable valves may impair mitral valve function10 and the impact of MR on mortality may vary according to valve type. Also, highly variable results have been reported in the literature with respect to MR changes following TAVR, with an improvement rate ranging from 12% up to 80%.2 We therefore undertook a comprehensive meta-analysis with the objective of (i) assessing the impact of moderate–severe MR on early and late mortality in patients included in TAVR national registries and randomised trials, and (ii) determining the changes in MR severity following TAVR overall and according to valve type (balloon-expandable valve (BEV) vs self-expandable valve (SEV)).
Methods
A systematic review of the published data on baseline MR in patients undergoing TAVR was performed according to the guidelines from the Cochrane Handbook of Systematic Reviews and following the PRISMA11 and MOOSE12 recommendations for meta-analysis interpretation and reporting.
Study search strategy
A computerised search was performed to identify all relevant studies published from January 2002 until December 2013 in the PubMed database. The following search terms were used: “TAVI”, “TAVR”, “transcatheter aortic valve” and “percutaneous aortic valve” and limited by English language subsequently. A secondary search was carried out also including the terms “mortality” or “mitral”. Citations were screened at the title and abstract level and retrieved as a full report if they reported the impact of MR on mortality or changes in MR severity following TAVR. References of the acquired articles were searched manually to identify any further relevant studies for the inclusion.
Study selection: inclusion criteria
All studies fulfilling the following criteria were included: (1) enrolment for TAVR was based on existing and accepted guidelines independently on the approach or the valve design, (2) reported data on mortality outcomes based on MR grading or changes in pre-TAVR and post-TAVR MR severity at a patient level and (3) enrolment of consecutive patients. To avoid publication bias, only data from TAVR national registries or randomised clinical trials were used to assess the impact of MR on short-term and mid-term mortality. Multinational registries that included patients from other national registries were excluded. If the outcome of moderate–severe MR was incomplete or not reported in the original publication, we contacted the main authors from TAVR national registries or randomised trials and invited them to participate in the study. All corresponded authors responded positively. The responding authors analysed and provided the requested data.
Exclusion criteria
Studies were excluded from the review if any of the following criteria applied: (1) duplicate publication, overlap of patients or subgroup studies of a main study; (2) abstracts, case reports, conference presentations and editorials; (3) outcomes of interest were not clearly reported or were impossible to extract or calculate from the published results; and (4) if changes of MR severity were evaluated with <1 month of follow-up.
Data extraction and quality assessment
One investigator abstracted data, which was independently verified by a second investigator. Relevant information collected included first author, year and journal of publication, study design, inclusion/exclusion criteria, enrolment period, definition of MR grading, numbers of centres and subjects included, population baseline characteristics, type of device used and number of patients lost in the follow-up. The quality of studies was scored using a checklist for the assessment of the methodological quality both of randomised and non-randomised studies.13 Discrepancies were resolved by discussion and consensus with a third investigator.
Statistical analysis
The effect, OR and HR for 30-day and 1-year mortality, respectively, were retrieved or calculated with the corresponding 95% CI from each study. Subsequently, natural logarithm of the effect and its SE were calculated. To be conservative, pooled measures were calculated assuming a random effect model using the inverse variance-weighted and used the adjusted OR/HR, when applicable. Fixed effect model and unadjusted OR/HR were also used to detect any discrepancies and included in the sensitivity analysis. Meta-regression analysis was performed to determine whether the impact of MR on mortality was statistically different according to valve type. Q-statistic and Higgins’ and Thompson’s I² test14 were calculated to evaluate heterogeneity among the studies. At least moderate heterogeneity was considered to be present for p<0.10 and an I2>50%. Sensitivity analysis was performed by deleting one study at a time, and a ≥20% modification of the overall effect by exclusion of a given study was considered significant. To assess the potential effect of publication bias, we inspected funnel plots for asymmetry and used the Egger's regression asymmetry test in which p<0.10 was considered significant of publication bias.15 Changes in MR severity pre-TAVR and post-TAVR were evaluated in a patient-level analysis and analysed with the non-parametric Wilcoxon signed-rank test in the whole population and in patients with greater than or equal to moderate MR. A quantile regression analysis was used to determine whether the valve type had differential effect on MR improvement adjusted by baseline characteristics and MR severity. Analyses were conducted using the statistical package STATA, V.12.0 (StataCorp, College Station, Texas, USA).
Results
A total of 3739 reports were identified by using the search keywords. The inclusion of the search term “mortality” or “mitral” narrowed the selection to 1566 publications, which were further reviewed at title and abstract level. Finally, 108 publications were assessed for eligibility, and following the application of the inclusion and exclusion criteria, a total of 85 ,6 ,9 ,16–20 and 99 ,21–28 studies were retained for the assessment of mortality and changes in MR severity outcomes, respectively. The studies for the mortality assessment outcome included two randomised trials and six national registries of TAVR. Three multinational registries were excluded due to the inclusion of the majority of their patients in other national registries,29–31 and two national registries were excluded after contacting the corresponding author because of missing data on MR severity in their original data set.32 ,33 In addition, 15 studies were excluded from the MR changes analysis due to insufficient individual data about the MR severity pre-TAVR and post-TAVR. Figure 1 shows the QUOROM flow chart. Overall, the analysis was performed on 8015 patients to assess the impact of baseline moderate–severe MR on mortality and on 1278 patients to determine the changes in MR severity following TAVR.

Flow chart showing search results and selection of the studies included in the meta-analysis.
Impact of baseline MR on mortality
Patient, study-level characteristics and quality ratings for selected studies are summarised in tables 1 and 2 and online supplementary table S1, respectively. Agreement between reviewers on quality assessment was good for national registries (κ=0.91) and complete in randomised trials (κ=1).
Characteristics of selected studies for the prognostic value of mitral regurgitation in patients undergoing TAVI
Baseline clinical characteristics of the population from selected studies
The overall 30-day mortality was higher in patients with significant MR (OR 1.49, 95% CI 1.16 to 1.92, I2=51.0%, Q=14.29, p=0.046) (figure 2). The OR for 30-day mortality in patients with concomitant significant MR receiving an SEV (n=3474) was 1.94 (95% CI 1.33 to 2.82, I2=0.0%, Q=2.47, p=0.480) and receiving a BEV (n=4492) was 1.31 (95% CI 0.94 to 1.84, I2=50.0%, Q=11.99, p=0.062) (figure 2). The Egger's test was not significant for publication bias (p=0.917).
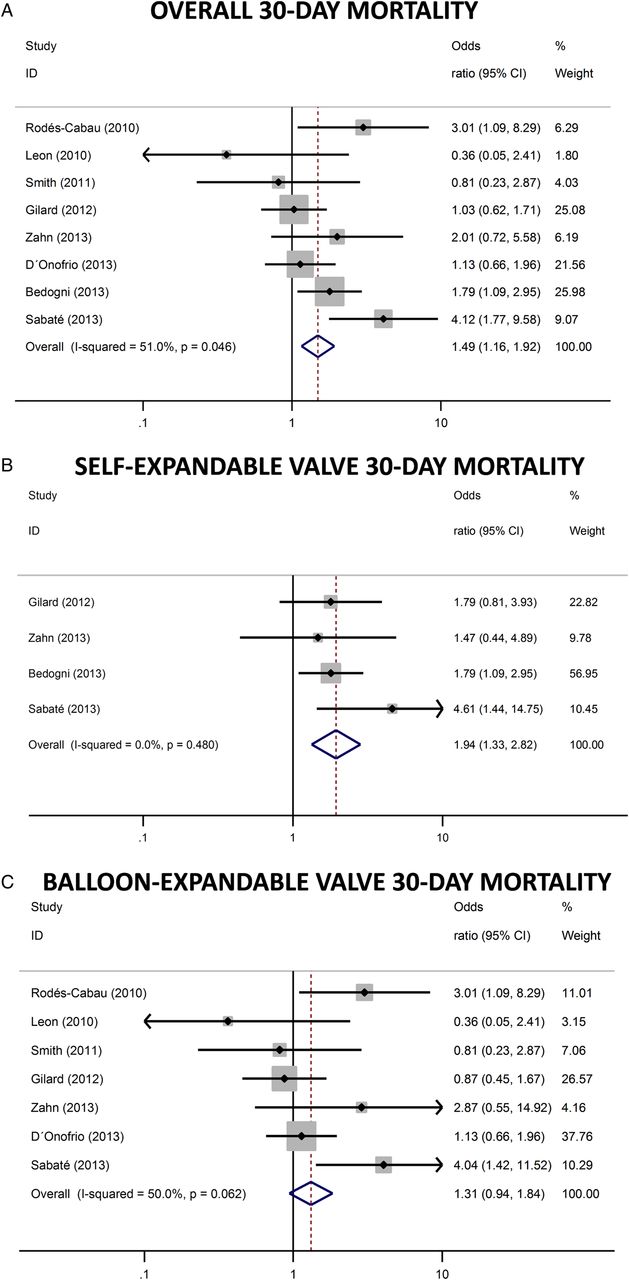
Forest plot showing the individual adjusted and pooled analysis for overall (A), self-expandable valve (B) and balloon-expandable valve (C) groups for the impact of significant mitral regurgitation (MR) on 30-day mortality. The size of the squares represents the percentage of the contribution of each study in the final result and is equivalent to the % weight of each study included in the meta-analysis. The lines represent the CI of the OR or HR (95% CI). The rhombus represents the final effect of the studied factor (significant MR) on mortality.
Baseline significant MR was associated with a higher 1-year mortality overall (HR 1.32, 95% CI 1.12 to 1.55, I2=62.5%, Q=18.69, p=0.009) and in the subgroup of patients who had SEV implantation (HR 1.62, 95% CI 1.23 to 2.14, I2=65.8%, Q=8.77, p=0.032). However, a borderline non-significant effect was found in the BEV group (HR 1.22, 95% CI 0.98 to 1.51, I2=23.3%, Q=7.83, p=0.251) (figure 3). The Egger's test was not significant for publication bias (p=0.409). Meta-regression analysis revealed that the impact of MR on 30-day and 1-year mortality was not different according to valve type—SEV vs BEV—OR of 1.44 (95% CI 0.61 to 3.41), p=0.360 for 30-day mortality, and OR of 1.29 (95% CI 0.68 to 2.46), p=0.388, for 1-year mortality. If unadjusted OR and HR were used, there was no change on the impact of MR on 30-day mortality or 1-year mortality overall and according to valve type (see online supplementary figures S1 and S2). Sensitivity analysis was not significant either for 30-day or 1-year mortality when omitting one study at a time.

{kind=link}
{kind=link}
{kind=link}
Forest plot showing the individual adjusted and pooled analysis for overall (A), self-expandable valve (B) and balloon-expandable valve (C) groups for the impact of mitral regurgitation (MR) on 1-year mortality. The size of the squares represents the percentage of the contribution of each study in the final result and is equivalent to the % weight of each study included in the meta-analysis. The lines represent the CI of the OR or HR (95% CI). The rhombus represents the final effect of the studied factor (significant MR) on mortality.
The results regarding the impact of MR on 30-day and 1-year mortality following TAVI when including only the studies using the two types of transcatheter valves17 ,18 ,20 are presented in online supplementary figures S3 and S4.
Changes in postprocedural MR severity
The characteristics of selected studies are summarised in table 3. Baseline MR was graded as none, mild, moderate or severe in 239 (18.7%), 518 (40.5%), 386 (30.2%) and 135 (10.6%) patients, respectively. At median follow-up of 180 (range 30–365) days, MR was graded as none, mild, moderate or severe in 255 (20.0%), 684 (53.5%), 257 (20.1%) and 82 (6.4%) patients, respectively (p<0,001 vs baseline). Overall MR improved in 287 (22.5%) patients, remained unchanged in 894 (70.0%) and worsened in 97 (7.6%) patients (table 4). Among the 386 patients with moderate MR at baseline, MR improved following TAVR in 186 (48.2%) patients (towards mild and no MR in 37.0% and 11.1%, respectively), remained moderate in 188 (48.7%) patients and worsened to severe MR in 12 (3.1%) patients. Among the 135 patients with severe MR at baseline, MR improved in 77 (57.0%) patients (towards moderate, mild and no MR in 24.4%, 31.1% and 1.5%, respectively) and remained severe in 58 (43.0%) patients. The improvement in moderate–severe MR was greater in patients who had received a BEV (66.7%) compared with those who had received an SEV (40.8%), p=0.001 (table 4). Using quantile regression analysis, patients with a BEV experienced an improvement in MR that was 1° higher than the improvement observed in patients with an SEV (1.0, 95% CI 0.92 to 1.08, p=0.01 after adjusting for baseline MR severity, rate of atrial fibrillation, functional MR, LVEF and pulmonary hypertension). The factors associated with improvement in MR severity are summarised in table 5. These factors could not be pooled because of limited number of studies and variable reporting.
Characteristics of selected studies for mitral regurgitation changes following TAVR
Changes in mitral regurgitation severity following TAVR
Predictors of mitral regurgitation improvement following TAVR
Discussion
This meta-analysis including >8000 patients with AS who underwent TAVR showed that baseline significant MR had a negative impact on early and late mortality. This negative clinical effect was irrespective of the transcatheter valve type, although a more pronounced negative effect was observed in patients with an SEV. Significant MR tended to improve by some degree in about half of the patients, and a higher likelihood of MR improvement was observed among those patients who had received a BEV.
Significant MR and mortality following TAVR
Some studies suggested an increase in acute mortality following TAVR in patients with significant MR,9 ,16 ,18 ,20 ,26 but others failed to demonstrate such association.8 ,17 ,19 This pooled analysis including patients from TAVR national registries and randomised trials showed that moderate–severe MR was associated with increased 30-day mortality. However, significant heterogeneity across studies was found in this meta-analysis. This was mainly driven by differences between BEV and SEV studies, with SEV data being more homogenous in the global effect of significant MR on early mortality. This heterogeneity between studies might partially be explained by higher proportion of severe MR in some studies (∼6–9%)9 ,16 ,20 compared with others (∼2%)6 ,7 ,17 and the incremental risk associated with increasing grades of MR severity.9 ,18
The presence of MR has been associated with poorer long-term outcomes in several cardiac diseases, including SAVR.3 ,34 Similarly, our results showed a significant increase in 1-year mortality following TAVR in patients with greater than or equal to moderate MR compared with those with non-significant pre-procedural MR, although significant heterogeneity was observed between studies. This discrepancy across studies may be related in part to the challenge of MR quantification and the lack of a core laboratory for the assessment of MR severity. Nevertheless, the pooled effect, although modest, clearly showed an increase in 1-year mortality among the patients with significant MR pre-TAVR. While a significant increase in late mortality was observed in patients with significant MR and an SEV, only a tendency towards increased late mortality was observed in those patients who had received a BEV. However, the meta-regression analysis did not reveal a statistical difference according to valve type. Several studies have shown a higher rate of moderate–severe residual aortic regurgitation following SEV implantation,7 ,32 ,35 ,36 and it may be associated with a more negative effect on clinical outcomes in patients with concomitant significant MR. However, these results should be taken with caution and longer-term follow-up results of the CHOICE trial and other randomised trials comparing both valves should help to clarify this issue.
Changes in MR following TAVR
The evolution of MR following TAVR is still controversial and a matter of concern. Our results showed an overall improvement in baseline MR in 23% of patients, no change in 70% and some degree of MR deterioration in the remaining 7%. Subgroup analysis of moderate–severe MR showed improvement in 51%, no change in 47% and worsening in 2%. In accordance with these results, previous studies have reported similar changes in moderate MR left untreated at the time of SAVR.3 ,8 Correction of aortic valve obstruction leads to an immediate drop in LV cavity pressure, and subsequently, in transmitral pressure gradient, resulting in a theoretical improvement in MR severity. The decrease in ventricular afterload contributes to a regression of myocardial hypertrophy, and this is associated with a positive remodelling of LV shape (especially if functional MR), which could contribute to the reduction in MR severity in the late postprocedural period.37 Two prior small studies suggested that BEVs (versus SEVs) were associated with a greater improvement in MR following TAVR.10 ,28 Similarly, this meta-analysis showed that patients with a BEV experienced a higher degree of MR improvement compared with SEV after adjusting for baseline MR severity. Several factors could explain this finding. It has been suggested that the longer frame of the SEV may physically interfere with the anterior leaflet of the mitral apparatus,23 although this was not confirmed in a recent large CoreValve series.9 The CoreValve system is associated with a higher degree of post-TAVR paravalvular aortic regurgitation and may maintain volume overload and contribute to a less MR improvement in such patients.36 ,38 In addition, SEV implantation is associated with a higher rate of both left bundle branch block and the need for pacemaker implantation, which indeed may lead to LV asynchrony and a negative effect on LV remodelling and MR improvement.39
Limitations
The results were derived mainly from observational studies that were not specifically intended to assess the impact of MR on mortality, except in two studies.8 ,9 There was a significant heterogeneity across studies for mortality outcome, except for the impact on 30-day mortality in patients with SEV. However, the results remained similar after removing one by one the studies in the sensitivity analysis or with the use of fixed-effect model. Moreover, the results were significant even with the use of adjusted OR/HR in our analysis, which usually penalises the effect, adding robustness to our findings. Publication bias could always be present when conducting a meta-analysis. To try to minimise this bias, we included all national registries and randomised trials even if the impact of MR was not originally reported. In such cases, contacting authors provided the adjusted prognostic value of MR, ensuring that we included studies with a negative or a neutral impact of MR on mortality. The comparison between the two types of prosthesis should be interpreted with caution due to observational nature of the studies included in the meta-analysis and the lack of randomised data. When evaluating MR changes post-TAVI, the studies used different grading methods to assess MR severity, and no centralised echocardiography core laboratory data were available, highlighting the need for an appropriate echo core lab evaluation of this issue in the future. The timing of MR evaluation at follow-up was not equal across studies; therefore, our postprocedural MR evaluation was performed at different points in the follow-up period. Furthermore, this may have led to selection bias due to the inclusion of survivors only in the echocardiographic analysis. Finally, the aetiology of MR (functional vs organic), which can be relevant in the evolution of MR over time, was not available in the majority of studies and this precluded any adjustment for this variable in the meta-analysis. Despite these limitations, the large sample size and the robustness of our results clearly show the need for ongoing critical evaluation of this problem when evaluating candidates for TAVR.
In conclusion, concomitant significant MR increased early and late mortality in patients with AS undergoing TAVI. This risk factor should therefore be taken into account in the evaluation of the risks associated with a TAVI procedure. Also, the possibility of a double-valve procedure should be considered in such cases, especially in the presence of severe MR in those patients at moderate or high but not prohibitive surgical risk. However, significant heterogeneity was detected across studies, and future research is needed to further determine the impact of baseline MR in such patients. Moderate–severe MR improved in about half of the patients following TAVR, but MR worsening was also detected in some (<10%) patients. There is still limited knowledge of the factors determining MR improvement; however, a higher likelihood of MR improvement was observed among patients who had received a BEV. Future studies will have to elucidate the mechanisms leading to differences in MR changes post-TAVR between BEV and SEV. Meanwhile, the results of the present meta-analysis provide further insight into the effects of and changes in MR in patients undergoing TAVR, and this may help in the clinical decision-making process and procedural planning for such a challenging group of patients.
Key messages
What is already known on this subject?
Significant mitral regurgitation (MR) is a common entity (∼15%) that is usually left untreated in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation (TAVI). The clinical impact and severity improvement of concomitant MR following TAVI has been arbitrarily reported with contradictory results.
What might this study add?
This large meta-analysis showed that baseline significant MR had a negative impact on early and late mortality in patients undergoing TAVI. Moderate–severe MR improved in about half of the patients following TAVI, more likely in patients receiving a balloon-expandable valve.
How might this impact on clinical practice?
The presence of significant MR should be considered when evaluating a patient for a TAVI procedure. The effects of and changes in MR in TAVI candidates should be taken into account in the clinical decision-making, procedural and follow-up process of such a challenging group of patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors LN-F, JR-C: Conception and design, and interpretation of data; drafting and revising of manuscript; final approval of the manuscript submitted. HE, RZ, LT, MBL, RT-N, ADO, CRS, JW, SB, BDC, MG, CT, FB, MB, SS, BGdB, MS, AM, HBR, IA-S, MU, RA, EG, CM, ED, PP: critical review of the manuscript for important intellectual content; final approval of the manuscript submitted. CF: interpretation and analysis of data; critical review of the manuscript for important intellectual content; final approval of the manuscript submitted.
Funding HBR is supported by a research PhD grant from “CNPq, Conselho Nacional de Desenvolvimento Científico e Tecnológico—Brasil”. IA-S is supported by a grant (beca Rio Hortega) from the Instituto de Salud Carlos III, Madrid, Spain. PP holds the Canada Research Chair in Valvular Heart Disease, Canadian Institutes of Health Research, Ottawa, Ontario, Canada.
Competing interests JW and JR-C are consultants for Edwards Lifesciences and St-Jude Medical. MBL, CRS, ED, EG and HE are consultants for Edwards Lifesciences. ADO is proctor for Edwards Lifesciences. FB is medical proctor for Medtronic. SB has financial relationship with Medtronic. CT is consultant for Edwards Lifesciences, CeloNova and Abbott. RZ has received research funding from Medtronic and Edwards Lifesciences. PP has received research funding from Edwards Lifesciences.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction