Article Text

Abstract
Objective Late gadolinium enhancement (LGE) on cardiac MRI that indicates the extent of myocardial fibrosis in hypertrophic cardiomyopathy (HCM) is a potential risk factor of sudden cardiac death (SCD) in non-high-risk patients according to conventional clinical markers.
Methods The present study was designed to systematically review prospective trials and assess the association between LGE and SCD in HCM. We systematically searched the electronic databases, MEDLINE, PubMed, Embase and Cochrane for prospective cohort studies of the effects of LGE on clinical outcomes (SCD/aborted SCD, all-cause mortality, cardiac and heart failure death) in HCM.
Results We identified six clinical studies, examining 1414 patients without LGE and 1653 with LGE and an average follow-up of 3.05 years. The incidence of SCD/aborted SCD in patients with HCM and LGE was significantly increased as compared with patients without LGE (OR 2.52, 95% CI 1.44 to 4.4, p=0.001). The all-cause mortality and cardiac death rates were also significantly increased in patients with LGE. The extent of LGE was not significantly related to the risk of SCD.
Conclusions LGE is significantly associated with SCD risk, cardiac mortality and all-cause mortality in patients with non-high-risk HCM according to conventional risk factors.
Statistics from Altmetric.com
Introduction
Hypertrophic cardiomyopathy (HCM) is the most common cause of sudden cardiac death (SCD) in young individuals, especially trained athletes.1 SCD due to ventricular tachyarrhythmias is often the first presentation, as a large proportion of patients with HCM are asymptomatic.1 Implantable cardioverter defibrillators (ICDs) for primary prevention of SCD are indicated in patients with conventional high-risk clinical markers such as: unexplained syncope, family history of premature SCD secondary to HCM, LV hypertrophy with wall thickness ≥30 millimeter (mm), non-sustained ventricular tachycardia (VT) on ambulatory ECG monitoring, inappropriate blood pressure response to exercise.1 However, current risk stratification tool to identify patients with HCM at risk for SCD remains inadequate as even individuals without these high-risk clinical markers succumb to sudden death at the rate of 0.8% per year.2 Recently, there has been considerable interest in identifying risk markers to recognise patients who may benefit from ICD, but are, otherwise, deemed as low-risk due to absence of conventional risk markers.3 Late gadolinium enhancement (LGE) on cardiac MRI (CMR) that indicates the extent of myocardial fibrosis in HCM is one such novel risk marker.3–9 Myocardial fibrosis acts as an electrophysiological substrate for ventricular tachyarrhythmias.10 Percentage of LGE on CMR is directly proportional to the extent of myocardial fibrosis.4 ,5 A number of studies4–9 have used LGE on CMR as a tool to stratify patients with HCM and determine the need for ICD in individuals who are considered at low risk for SCD. The objective of our meta-analysis is to assess the utility of CMR on LGE as a prognostic factor of SCD in HCM, which could potentially identify at-risk individuals who may benefit from an ICD.
Methods
Search strategy
We systematically searched the electronic databases, MEDLINE, PubMed, Embase and the Cochrane Library for Central Register of Clinical Trials, using the MESH terms ‘hypertrophic cardiomyopathy’, ‘cardiovascular magnetic resonance’, ‘late gadolinium enhancement’ and ‘myocardial fibrosis’. We limited our search to studies in human subjects and English language in peer-reviewed journals published until January 2015. A total of six studies have been identified by two reviewers after the independent electronic search. There were no disagreements in literature search between the reviewers. Subsequently, we manually searched the references listed in the six studies identified by electronic search. Manual search did not reveal any new studies apart from the ones identified by electronic search.
Study selection
We included all observational studies published as original articles in peer-reviewed scientific journals in English. Studies were selected based on inclusion criteria: patient population—group of patients diagnosed with HCM in accordance with standard clinical guidelines and eligible for CMR, use of LGE to quantify the amount of myocardial fibrosis and comparison of outcomes between patients with and without myocardial fibrosis. We excluded those trials that did not report any of the following variables or outcomes: number of events in both the intervention and reference groups, length of study, description of the main relevant features of the study population, including gender and age. We did not restrict eligibility according to outcomes.
Data extraction and quality
The data were independently extracted by two authors (AB and MP) using standardised protocol and reporting form. Disagreements were resolved by discussion with a third reviewer, and consensus was reached after discussion.
We extracted study characteristics such as study design, sample size, baseline demographics and cardiovascular risk factors, inclusion criteria and exclusion criteria, primary and secondary outcomes and follow-up duration, and patient demographic characteristics.
Outcomes assessed
The primary outcome measure was SCD/aborted SCD, defined as unexpected death that occurred within an hour of onset of cardiac symptoms in the absence of progressive cardiac deterioration within last 24 h of being alive. We also examined death or all-cause mortality, heart failure (HF) death, cardiac death and aborted SCD. Only four studies4–6 ,9 included all-cause mortality as part of their outcomes. HF and cardiac death were included in five out of six studies.5–9
Risk of bias
The Newcastle–Ottawa tool was used for the quality assessment of cohort studies. Two authors independently assessed the risk of bias and quality of studies in each eligible trial. This scale appoints a maximum of nine stars to each study: four stars for the adequate selection of the two groups, two stars for comparability of groups on the basis of the design and analysis, and three stars for the adequate ascertainment of the exposure in both groups. High-quality studies received nine stars, and medium-quality studies received seven or eight stars.
Data analysis and synthesis
Data analysis was done in accordance with the Cochrane Collaboration, Meta-analysis Of Observational Studies in Epidemiology (MOOSE) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. Meta-analyses were performed by using the Review Manager (RevMan) 5.2. χ2 test of heterogeneity and I2 statistic of inconsistency were used to assess heterogeneity between studies. I2 values of 25%, 50% and 75% indicate low, moderate and high heterogeneity, respectively. A significant heterogeneity was considered if the p<0.05 or an I2 statistic >75%.
In the absence of heterogeneity, pooled estimates of odd risks (ORs) with their 95% CIs were calculated using the Mantel–Haenszel method. Reported values are two-tailed, and hypothesis-testing results were considered statistically significant at p<0.05. The small-study effect, including publication bias, was tested using funnel plot and the Egger's test.
The interaction of LGE extent (%) with studied outcomes was assessed by univariable random effects meta-regression in order to explore residual heterogeneity between studies. When using binary study-level covariates, the exponentiated coefficient from meta-regression analysis quantifies the relative OR, comparing the subgroups of studies defined by the covariate. The regression was weighted so that the more precise studies have more influence in the analysis. The weight for each trial was equal to the inverse of the sum of the within-trial variance and the residual between-trial variance, in order to correspond to a random-effects analysis. Meta-regression (OpenMeta analyst) was used to assess whether LGE extent (%) was associated with the primary outcomes.
Results
Study selection
Our search strategy is outlined in figure 1. Literature search resulted in a total of 177 studies. Titles and abstracts were reviewed. Studies were selected based on inclusion criteria: patient population—group of patients diagnosed with HCM in accordance with standard clinical guidelines and eligible for CMR, use of LGE to quantify the amount of myocardial fibrosis and comparison of outcomes between patients with and without myocardial fibrosis; finally resulting in six studies. We excluded review articles and case–control studies. We were not able to identify any new studies after hand search. A total of six studies were finally included in the meta-analysis.4–9 All of them were reported between 2008 and 2014.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
Study characteristics
The total number of patients without myocardial fibrosis was 1414, and who demonstrated myocardial fibrosis were 1653. The average follow-up duration was 3.05 years. Mean age of the study population was 60 years. The baseline characteristics of the included studies are represented in table 1.
Interventions and characteristics of individual studies
Quality assessment
On the basis of quality assessment, five studies4–6 ,8 ,9 were deemed as high quality and one study of medium quality.7 No low-quality studies were included.
SCD and aborted SCD
All included studies reported data on SCD. The incidence of SCD/aborted SCD in patients with HCM and myocardial fibrosis was significantly increased as compared with patients without fibrosis (OR 2.52, 95% CI 1.44 to 4.4, p=0.001; figure 2), without significant heterogeneity between trials (I2 0%, p=0.66).

Fixed-effect meta-analysis for sudden cardiac death/aborted sudden cardiac death. The figure presents number of events, number of patients in treatment and control groups, OR and 95% CI for each trial, overall OR estimate with 95% CI and p value for association test, p value for heterogeneity test and between-trial inconsistency (I2) measures. LGE, late gadolinium enhancement.
All-cause mortality
Only four studies reported data on the incidence of all-cause mortality. All-cause mortality rates were significantly increased in patients with LGE enhancement (OR 1.80, 95% CI 1.21 to 2.67, p=0.003; figure 3) without significant heterogeneity between trials (I2 30%, p=0.23).

Fixed-effect meta-analysis for all-cause mortality. LGE, late gadolinium enhancement.
HF death
Five studies reported data on the incidence of HF death. There was a trend towards increased HF death rates in patients with LGE (OR 2.47, 95% CI 0.98 to 6.24, p=0.06; figure 4) without significant heterogeneity between trials (I2 0%, p=0.52).

Fixed-effect meta-analysis for heart failure death. LGE, late gadolinium enhancement.
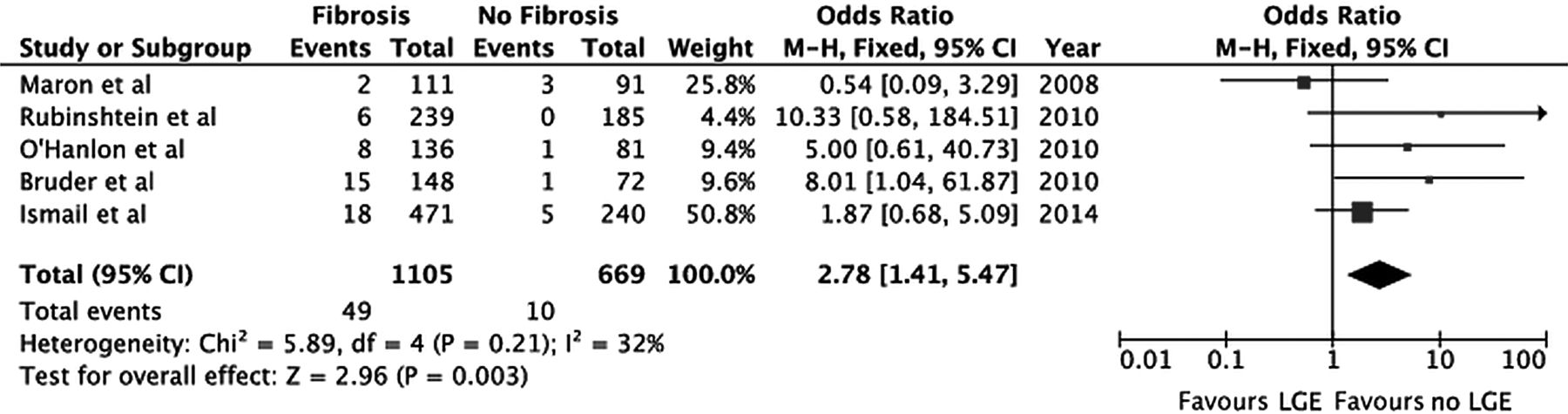
Cardiac death
Five studies reported data on the incidence of cardiac mortality. Cardiac death rates were significantly increased in patients with LGE enhancement (OR 2.78, 95% CI 1.41 to 5.47, p=0.003; figure 5) without significant heterogeneity between trials (I2 32%, p=0.21).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fixed-effect meta-analysis for cardiac death. LGE, late gadolinium enhancement.
Publication bias
The funnel plot did not show asymmetry consistent with publication bias, and the Egger's test was not significant for the outcomes studied.
Meta-regression analysis
We performed a meta-regression analysis, which demonstrated that the extent of LGE (%) was not significantly related to SCD/aborted-SCD risk (p=0.35), all-cause mortality (p=0.084), cardiac death (p=0.59) and HF death (p=0.99) (see online supplementary table).
Discussion
Our study suggested that myocardial fibrosis as suggested by LGE on CMR is significantly associated with SCD, aborted SCD, cardiac mortality and all-cause mortality.
Compared with the previous meta-analysis by Green et al,11 which was conducted on four studies5 ,7–9 comprising a total number of 1063 patients with HCM, our current study re-evaluated the prognostic utility of LGE by including two large recent studies,4 ,6 thus, analysing almost twice the number of patients with HCM. Our results confirmed the association of myocardial fibrosis on CMR with cardiac death and all-cause mortality, and also demonstrated statistically significant association with SCD and aborted SCD.
In patients with HCM, cardiac myocyte disarray and deformation of intramural coronary arteries lead to microvascular ischaemia and myocyte death, which eventually result in myocardial fibrosis.12
SCD is a catastrophic complication of HCM, and can be the first presentation of the disease. Therefore, risk stratification by using multiple factors is necessary in all patients with HCM regardless of the symptomatic status. Patients with no risk factors have 5% risk of SCD, and those with one risk factor have 7% risk of SCD at 6 years.2 The SCD risk increases to 5% per year in patients with two or more risk factors.2 All studies included in our analysis recruited patients at low-to-intermediate SCD risk with the percentage of patients with two or more risk factors ranging from 5.5% to 8.6%. The inclusion of non-high-risk patients in all studies is supported by the SCD rates, which were ≤4% in all studies. According to the recent recommendations of European Society of Cardiology, ICD should be considered for those patients with 5-year SCD risk >6%.1
LGE on contrast-enhanced CMR mostly represents myocardial fibrosis that provides a substrate for ventricular tachyarrhythmias and is associated with a sevenfold increase in the risk of non-sustained VT in patients with HCM.13 However, a significant portion of patients with HCM demonstrate some degree of LGE.3 Five of the studies included in our analysis had >5% extent of LGE on CMR. A prospective cohort study6 suggested LGE as significant predictor of SCD, but on multivariate analysis, only LVEF remained an independent predictor. In contrast, the largest and most recent study4 showed that adjusted SCD risk proportionally increased with respect to the extent of LGE, particularly with LGE% ≥10%. Each 10% increase in LGE was associated with 40% increase in SCD risk. Our meta-regression analysis did not reveal an association between the extent of LGE and outcomes studied. That could be explained by the fact that five studies included patients with a mean LGE extent of <10%.
End-stage HCM is characterised by adverse LV remodelling and systolic dysfunction (EF <50%), which is considered as a poor prognostic indicator.14 A significant portion of patients with HCM and reduced EF have LGE on CMR.5 ,6 Although the studies included in the analysis included a small percentage of patients with LVEF <50%, a trend towards increased HF death was observed (p=0.06).
There are some limitations to the interpretation of our data analysis. First, publication bias may still exist despite our best efforts to conduct a comprehensive search and despite the lack of statistical evidence for the existence of bias. Second, any meta-analysis based on pooling of data from different trials with different inclusion criteria, different designs and populations, variable follow-up duration with differing attrition rates, and not being unified in definition and validation of endpoints in individual trials presents challenges.15 Finally, a small percentage of patients <10% that exhibited higher SCD risk were included in all studies.
Our study confirms that LGE on CMR in patients with HCM LGE has significant prognostic relevance, and is associated with poor outcomes. Extensive LGE is a promising risk-stratification tool as it significantly predicts SCD risk, cardiac mortality and all-cause mortality in patients without conventional risk markers. Hence, LGE should be considered a novel risk marker in predicting SCD in HCM. Currently available data support the consideration for ICD implantation in patients with extensive LGE for primary prevention of SCD, even if they are not at high-risk according to the conventional risk markers. Future studies should focus on the additive predictive value and reclassification of patients with HCM by the addition of CMR findings to currently available risk models.
Key messages
What is already known on this subject?
Late gadolinium enhancement (LGE) on cardiac MRI that indicates the extent of myocardial fibrosis in hypertrophic cardiomyopathy (HCM) is a potential risk factor of sudden cardiac death (SCD) in low-risk patients according to conventional clinical markers.
What might this study add?
LGE significantly predicts SCD risk, cardiac mortality and all-cause mortality in patients without conventional risk markers.
How might this impact on clinical practice?
Current guidelines do not include presence of LGE in the decision model for implantable cardioverter defibrillator implant. The present study, however, demonstrates that presence of LGE is associated with an increased risk of SCD even in patients without traditional clinical risk factors, but the presence of LGE in a large proportion of patients with HCM means it lacks specificity. Further work could look at the extent of LGE as a more specific risk marker.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors AB: analysis, data gathering, manuscript preparation; SM-R: data gathering, review of studies; MP: study analysis; IA: manuscript preparation, supervision; LA: original idea, supervision.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.