Article Text

Abstract
Objective Patients with repaired tetralogy of Fallot (TOF) are followed serially by cardiac magnetic resonance (CMR) for surveillance of RV dilation and dysfunction. We sought to define the prevalence of progressive RV disease and the optimal time interval between CMR evaluations.
Methods Candidates were selected from a multicentre TOF registry and were included if ≥2 CMR studies performed ≥6 months apart were available without interval cardiovascular interventions. Patients with ‘disease progression’ (defined as increase in RV end-diastolic volume index (RVEDVi) ≥30 mL/m2, decrease in RVEF ≥10% or decrease in LVEF ≥10%) were compared with those with ‘disease non-progression’ (defined as RVEDVi increase ≤5 mL/m2, RVEF decrease ≤3% and LVEF decrease ≤3%).
Results A total of 849 CMR studies in 339 patients (median age at first CMR 23.6 years) were analysed. Over a median interval of 2.2 years between CMR pairs, RVEDVi increased 4±18 mL/m2 (p<0.001), RV end-systolic volume index increased 3±13 mL/m2 (p<0.001), RVEF decreased 1%±6% (p=0.02) and LVEF decreased 1%±6% (p=0.001). Disease progression was observed in 15% (n=76) and non-progression in 26% (n=133). There were no significant differences between those with and without progression in baseline demographic, anatomic, ECG, exercise or baseline CMR characteristics. The optimal time interval between CMR studies for detection of progression was a 3-year interval (63% sensitivity, 65% specificity, area under the receiver operating characteristic curve 0.65).
Conclusions Although progressive RV dilation and decline in biventricular systolic function occur at a slow pace in the majority of adults with repaired TOF, 15% of patients experience rapid disease progression. The results of this study support the practice of serial CMR examinations to identify progressive disease at a time interval of up to 3 years.
Statistics from Altmetric.com
Introduction
The majority of patients with repaired tetralogy of Fallot (TOF) are exposed to chronic pulmonary regurgitation (PR) as a result of reconstructive surgery to relieve the obstruction in the RV outflow tract. The ensuing RV remodelling has been associated with biventricular systolic dysfunction, exercise intolerance, arrhythmia and premature death.1 ,2 In light of the growing awareness of the clinical importance of timely identification of deteriorating ventricular size and function and reliance on ventricular parameters for deciding when to recommend pulmonary valve replacement (PVR), guidelines for care of the adult with congenital heart disease recommend serial cardiac MRI (CMR) studies in patients with repaired TOF.3–6 Although a 2- or 3-year interval between CMR studies has been proposed,4 ,6 no published evidence is available to support this recommendation.
While several investigators have demonstrated that ventricular parameters worsen over time in patients with repaired TOF, others have suggested that, at least in the short-term, RV parameters remain stable in the overall population.7–9 Nevertheless, clinical experience suggests that in some patients RV dilatation and dysfunction can worsen precipitously. These inconsistent observations highlight current gaps in knowledge, including: (1) uncertainty about the prevalence of rapidly progressive disease, (2) absence of markers that may identify patients at risk for worsening ventricular parameters and (3) paucity of information regarding the optimal strategy for CMR surveillance. Published studies to date have been hampered by modest patient numbers, relatively short time intervals between CMR examinations and a limited number of CMR studies per patient.7 ,9 ,10
Therefore, this study was undertaken to: (1) characterise the rate of change in ventricular parameters over time in a large contemporary cohort of patients with repaired TOF, (2) determine the prevalence of clinically important progressive disease and (3) identify markers of progressive versus non-progressive disease from baseline demographic, clinical, ECG and CMR characteristics.
Methods
Patients
Subjects were selected from the International Multicenter TOF Registry (INDICATOR), representing patients with repaired TOF followed at four large congenital heart disease centres in North America (Boston Children's Hospital and Toronto General Hospital) and Europe (Royal Brompton Hospital in London and Academic Medical Center in Amsterdam). Each patient in the INDICATOR cohort had ≥1 CMR study completed between 1997 and 2010. Demographic (eg, age and gender) and clinical (eg, anatomic type of TOF, surgical history and clinical status at last follow-up) data, ECG (eg, QRS duration), and, when available, 24 h Holter monitor and exercise test results were recorded. The details of the INDICATOR study population, study methodology and clinical outcomes have been published.2 ,11 Each participating centre received Institutional Review Board or Research Ethics Board approval. Eligible patients from the INDICATOR registry were included if: (1) ≥1 CMR study was available for analysis at an interval of at least 6 months between them, (2) no interval cardiovascular intervention (eg, PVR, other valve repair or replacement, pulmonary artery (PA) dilation or stent implantation) had occurred between studies and (3) CMR studies had appropriate image data for evaluation of ventricular volumes and function by steady-state free precession cine imaging. Subjects were excluded from the analysis if the diagnosis of TOF was complicated by additional structural lesions such as common atrioventricular canal or heterotaxy syndrome.
Study endpoints
Clinically important ‘disease progression’ was defined as fulfilling any one of the following criteria between consecutive CMR studies: (1) increase in indexed RV end-diastolic volume (RVEDVi) ≥30 mL/m2, (2) decrease in RVEF ≥10% (eg, from 40% to 30%) or (3) decrease in LVEF ≥10%. These threshold values were selected based on published data from the core CMR laboratory on reproducibility of ventricular measurements in repaired TOF.12 ,13 Specifically, the selected cut-off values exceed two SDs of the interobserver and interstudy variability for each parameter. In addition, we defined an endpoint termed ‘marked disease progression’, defined as having any one of the following criteria: (1) increase in RVEDVi ≥40 mL/m2, (2) decrease in RVEF ≥15% or (3) decrease in LVEF ≥15%. Conversely, ‘disease non-progression’ was defined as fulfilling all of the following criteria: (1) increase RVEDVi ≤5 mL/m2, (2) decrease in RVEF ≤3% or (3) decrease in LVEF ≤3%. An intermediate group included those who did not meet the aforementioned definitions or those in whom data were missing, precluding assignment to either a category of disease progression or non-progression.
CMR analysis
All CMR analyses took place at a core laboratory at Boston Children's Hospital. Details of the CMR imaging protocol, data transfer to the core laboratory and the methodology used for ventricular measurements in the INDICATOR cohort have been published.2 ,11 ,14 Ventricular volumes and mass were indexed to body surface area calculated using the formula of Haycock et al and z-scores were computed based on normative data published by Alfakih et al.15 ,16
Statistical analysis
Continuous variables were described as means and SDs or as medians and ranges, as appropriate. Categorical variables were summarised using frequencies and percentages. Continuous CMR parameters were compared between consecutive studies using generalised estimating equations (GEE) models, which account for the correlation among multiple pairs of studies contributed by the same patient. GEE models were also used to compare demographic, CMR, ECG and exercise characteristics for study intervals demonstrating progression versus those with non-progression; these models were adjusted for length of time from first to second CMR. For patients with two consecutive CMR intervals (ie, first to second and second to third CMR examinations), Pearson correlation coefficients were used to evaluate the relationship between changes in these time intervals. Linear mixed models were used to estimate the mean change per year in ventricular size and EF. Area under the receiver operating characteristic (ROC) curve was used to identify the optimal time interval between CMR studies that maximised sensitivity and specificity for identifying progression. A p value ≤0.05 was considered statistically significant. All analyses were performed using SAS V.9.2 (SAS Institute, Cary, North Carolina, USA).
Results
Patient characteristics
A total of 849 CMR studies in 339 patients (55% male) were included in this study. The median age at TOF repair was 3.2 years (range 2 days to 45.3 years) and the median age at the baseline CMR was 23.6 years (range 1.8 to 62.9 years); 243 patients (72%) were ≥18 years, 49 patients (14%) were 12–17 years and 47 patients (14%) were <12 years. The number of CMR studies per patient was 2 in 223 patients (66%), 3 in 79 (23%), 4 in 26 (8%) and 5 or higher in 11 patients (4%); the maximum number of CMR studies per patient was 7. There were 507 distinct CMR pairs (in patients with several CMR studies, a single CMR could be counted in more than one pair). The median time interval between CMR studies was 2.2 years (range, 6.3 months to 7.7 years). Of the 339 patients, 97 (29%) underwent PVR following ≥2 CMR studies. Compared with patients who did not have PVR during the study period (n=242), those who did were younger at the time of TOF repair (median 0.8 years [range 2 days to 19 years] vs 3.9 years [range 2 days to 45.3 years], p<0.001), were younger at the time of first CMR (20.1 years [range 3.1–59.5 years] vs 26.4 years [range 3.3–63.4 years), p<0.001], and were more likely to have underlying pulmonary atresia (17.5% vs 8.7%, p=0.02).
Changes in ventricular parameters
Comparisons of CMR parameters between the first and second studies of the 507 pairs are summarised in table 1. Small but statistically significant changes in RV parameters were observed in the overall cohort, including increases in RVEDVi and RV end-systolic volumes (RVESVi) and their respective z-scores, and a decrease in RVEF. RV mass z-score did not change significantly, and RV mass-to-volume ratio decreased as RVEDVi increased with no commensurate change in RV mass index. RV stroke volume index and PR fraction did not change. Among LV parameters, small increases in indexed LV end-diastolic (LVEDVi) and end-systolic volumes (LVESVi) and their z-scores, and a decrease in LVEF were noted. Similar to the RV, the increase in LVEDVi was not accompanied by a commensurate change in LV mass index, resulting in a decrease in LV mass-to-volume ratio. The RV/LV end-diastolic volume ratio increased significantly between CMR studies, indicating that, on average, the increase in RV volume exceeded that of LV volume.
Changes in CMR parameters from baseline to second study in 507 CMR pairs
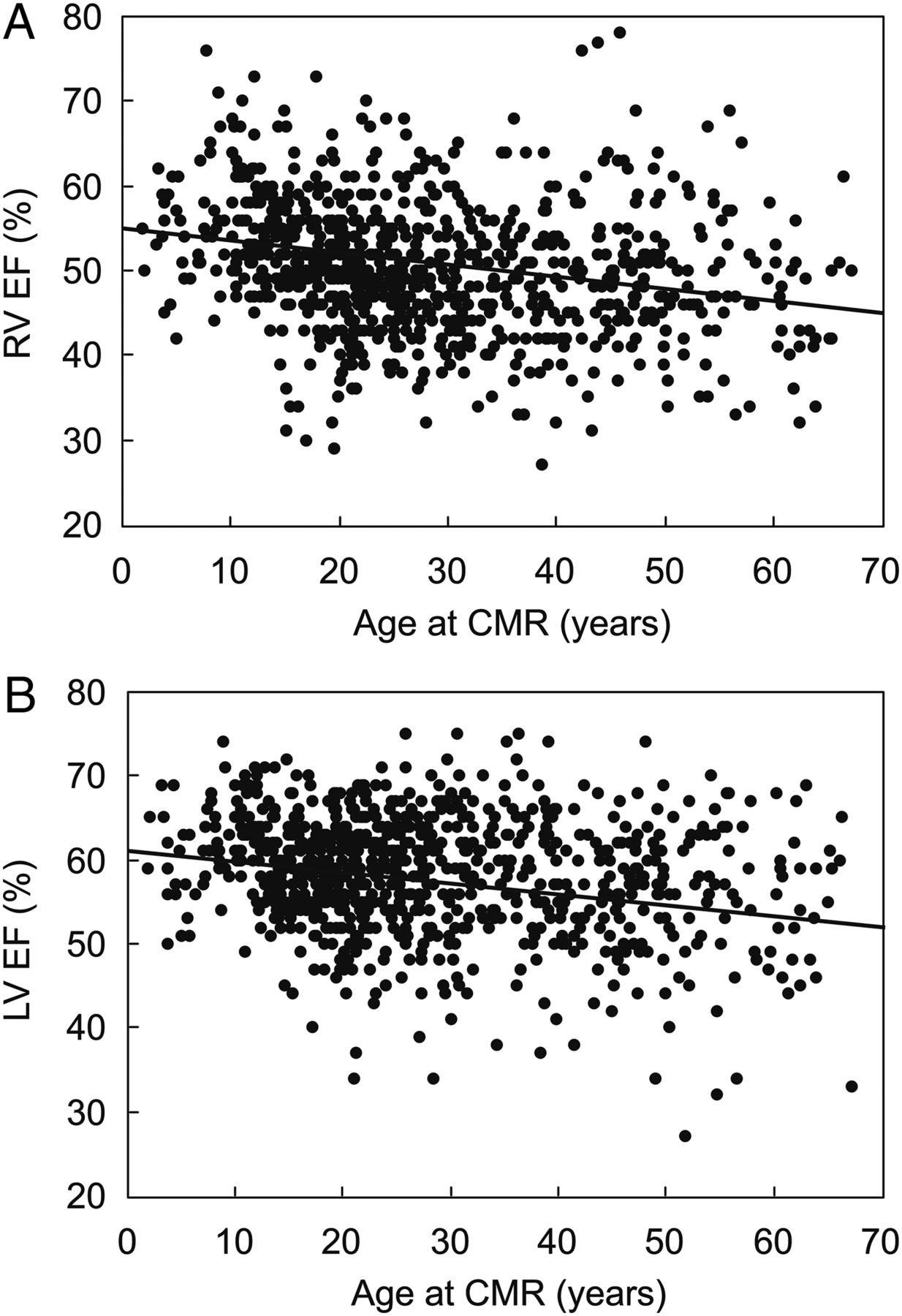
Using linear mixed models to estimate the mean change in ventricular volumes and EFs as a function of age in the entire study population, we found that RVEDVi did not change significantly (mean increase of 1.5 mL/m2 for each 10-year increase in age (p=not significant (NS))). On the other hand, RVESVi increased by 3.4 mL/m2 and RVEF decreased by 1.4% for each 10-year increase in age (p<0.001, respectively) (figure 1A). Rates of change in the LV over time were also minimal; LVEDVi increased 1.2 mL/m2 (p=0.03), LVESVi increased 1.6 mL/m2 (p<0.001) and LVEF decreased 1.2% (p<0.001) for each 10-year increase in age (figure 1B).

Plots of right (A) and left (B) ventricular EF versus age in 849 CMR studies in 339 patients. RVEF decreases by 1.4% for each 10-year increase in age (p<0.001) (A). LVEF decreases by 1.2% for each 10-year increase in age (p<0.001) (B). CMR, cardiac magnetic resonance.
To evaluate whether changes in ventricular size and function over time differed between those who typically would not be considered candidates for PVR based on most current CMR criteria and those who may be candidates, we stratified the patients into the following subgroups: (1) patients without important ventricular dilation and normal ventricular function defined as RVEDVi <120 mL/m2, RVEF >48% and LVEF >55%; and (2) patients with ventricular dilation and/or dysfunction, defined as RVEDVi 120–170 mL/m2, RVEF 40%–48% and LVEF 50%–55%. The rate of change in ventricular volumes and EFs did not significantly differ between these two subgroups.
Factors associated with disease progression
Based on our prespecified criteria, disease progression was observed in 76 patients (15%) and non-progression in 133 (26%). Of the remaining patients, 225 (44%) did not fulfil criteria for either group as defined above and 73 patients (14%) could not be classified due to incomplete data for ventricular size and/or function. Among the 76 patients with disease progression, the classification was based on increase in RVEDVi ≥30 mL/m2 alone in 23 patients (30%), decrease in RVEF ≥10% alone in 18 patients (24%), decrease in LVEF ≥10% alone in 25 patients (33%), having 2 of the 3 criteria in 7 patients (9%) and having all 3 criteria in 3 patients (4%). Of the 76 patients with disease progression, 45 (59%) met published CMR criteria for PVR defined as any two of the following: RVEDVi >150 mL/m2, RVESVi >80 mL/m2, RVEF <47%, LVEF <55% or QRS duration >160 ms on ECG.17 During follow-up, 30 patients from the disease progression group (40%) underwent PVR. Figure 2 depicts changes in RVEDVi, RVEF and LVEF in patients with and without disease progression as a function of the time interval between sequential CMR studies.

Box and whiskers plots comparing changes in indexed RV end-diastolic volume (RVEDVi) (A), RVEF (B) and LVEF (C) between those with disease progression (pink bars, right) and those with non-progression (blue bars, left) at different time interval between CMR examinations. CMR, cardiac magnetic resonance.
Table 2 summarises the comparison of baseline demographic, anatomic, ECG and exercise parameters between patients with progression versus non-progression. None of the parameters examined differed significantly between the groups. Similarly, a comparison between those with disease progression with all others (the non-progression and intermediate groups) found no significant difference between the groups. Notably, the prevalence of an RV-to-PA conduit tended to be higher in those with progression as compared with the remaining patients (9/76 (12%) vs 29/431 (7%), p=0.07). Among the 190 patients with contemporaneous echocardiographic data (57 with disease progression and 133 without), the degree of tricuspid regurgitation and/or RV outflow tract obstruction did not differ between the outcome groups.
Comparison of demographic, anatomic, electrocardiographic, and exercise characteristics between patients with and without disease progression
Table 3 compares the baseline CMR characteristics between patients with disease progression and those with non-progression. Compared with those who did not progress, those who did had higher RVEF, RV stroke volume index, LVEF, LV stroke volume index and lower LVESVi at baseline CMR. None of the other parameters examined differed significantly between the groups. Restricting the analysis to those with CMR pairs at least 2 years apart and matching patients with disease progression with those who did not progress for length of follow-up (n=71 in each group) did not identify new variables that differentiated between the groups. Similarly, those with marked disease progression (n=30; 6%) did not have any identifiable features that distinguish them from non-progression at the time of baseline evaluation.
Comparison of CMR parameters between patients with and without disease progression
Comparison between patients who received an RV-to-PA conduit as part of their primary TOF repair (n=36) and those with other types of RV outflow tract reconstruction (n=450) demonstrated that the frequency of disease progression was similar in both groups (16% in patients with conduit vs 15% in those without). However, among patients with a conduit, comparison of baseline CMR parameters between patients who experienced progression (n=9) versus those who did not (n=18) found that those who progressed had significantly higher RVEDVi (135±54 vs 116±23 mL/m2, p=0.04), RVESVi (88±65 vs 55±19 mL/m2, p=0.007), RV mass index (50±17 vs 35±17 g/m2, p=0.05) and lower RVEF (48±9 vs 53%±9%, p=0.02).
To determine whether changes in RV size and function at a given time interval between two CMR examinations are predictive of the rate of change on subsequent assessments, we analysed all patients with three or more studies (n=116). As seen in table 4, changes in ventricular parameters during the first interval correlated modestly with changes on subsequent intervals. The most closely correlated parameters were RVEF, LV volumes and LV stroke volume index.
Correlations between changes in ventricular parameters in patients with two or more pairs of CMR studies (n=116)
Frequency of CMR studies for detection of disease progression
The proportion of patients with disease progression detected at various time intervals between CMR studies is depicted in figure 3. Of the 76 patients with progressive disease, 11% were detected when the time between CMR studies was 1–2 years. The frequency of detection increased to 28% when the interval was three or more years (p<0.001). Similarly, the frequency of detecting marked disease progression was only 3% when the interval between CMR studies was 1–2 years, increasing to 14% when the time between CMR studies was 3 years or longer (p<0.001). ROC analysis identified an interval between CMR examinations of 3 years as having the best balance of sensitivity and specificity (63% and 65%, respectively; area under the ROC curve 0.65) for detection of disease progression. Shorter intervals (1–2 years) resulted in a higher sensitivity but lower specificity, whereas longer intervals (4 years or longer) resulted in a higher specificity but lower sensitivity.

{kind=link}
{kind=link}
{kind=link}
Per cent of patients with disease progression detected by sequential CMR studies according to time interval between examinations. Depicted are changes in indexed RVEDVi in blue, RVEF in pink and LVEF in green. CMR, cardiac magnetic resonance; RVEDVi, RV end-diastolic volume index.
Discussion
During the past 15 years, CMR has assumed a key role in the longitudinal follow-up of adolescent and adult patients with repaired TOF. The rationale for this clinical practice, which has been advocated by individual researchers and endorsed by professional societies,3–6 ,14 ,18 ,19 is that CMR is ideally suited for monitoring changes in RV size and function.20 However, despite its broad incorporation into routine clinical practice, little information exists regarding the frequency and rate of change in CMR measurements in this patient population over time and what is the optimal interval between serial studies.
In this large multicentre study, we found that in the cohort as a whole, RV and LV volumes, mass, and systolic function changed slowly over time whereas PR fraction remained stable. However, 15% of the patients experienced substantial deterioration in RV volumes and/or either RV or LV systolic function and 6% experienced marked disease progression. Of those with disease progression, nearly two of three patients met published criteria for PVR17 and 40% underwent the procedure during the study period. Disappointingly, we were unable to identify robust baseline clinical, ECG, exercise or CMR predictors of significant deterioration on a subsequent study. The exception to this was the group of patients with RV-to-PA conduit in which higher RV volumes and lower EF at baseline CMR were significantly associated with disease progression on a follow-up study performed at least 6 months later (median 2 years).
Our work expands upon the current knowledge of serial changes in ventricular measurements late after TOF repair in several ways. To date, the few published studies on this topic have been hampered by a modest number of patients, short intervals between sequential CMR examinations and lack of clearly defined criteria for what constitutes a significant change in ventricular parameters.7–10 Our study overcomes these shortcomings because it represents a large multi-institution cohort, which includes serial CMR studies that were analysed in a central core laboratory. The multicentre nature of our cohort enhances the generalisability of the findings while processing the CMR data in a core laboratory reduces measurement variability. Furthermore, our study design included predefined criteria for disease progression and non-progression, which minimises the possibility of misclassifying patient endpoints.
The results of this study have several clinical implications. Our findings support clinical guidelines that recommend serial CMR studies at intervals of approximately 3 years.4 ,6 This conclusion is based on the observation that this frequency appears to represent a statistically significant inflection point at which a greater proportion of patients with disease progression are detected as compared with annual or biennial CMR studies. Furthermore, in this study a screening interval of 3 years had the highest area under the ROC curve for detection of disease progression. Another clinically relevant observation is that presence of mild RV dilatation and normal function at baseline CMR does not provide assurance of stability of ventricular parameters at subsequent studies. Importantly, evidence of progressive ventricular dilation or dysfunction during any time interval between sequential CMR studies may signal ventricular decompensation leading to consideration of PVR. Therefore, in patients who are not on the verge of fulfilling criteria for PVR, do not have an RV-to-PA conduit, and have not demonstrated a substantial worsening of ventricular or clinical parameters on prior studies, a 3-year interval between CMR examinations appears to be appropriate. Those who do not fulfil these criteria may require more frequent evaluations.
Limitations
The retrospective nature of this study imposes several limitations such as exclusion of patients in whom certain CMR measurements could not be performed and inconsistent time intervals between CMR studies. However, an ideal study design in which every patient undergoes a yearly CMR study may be impractical. Furthermore, the observation that a 3-year interval between CMR examinations has the best balance between sensitivity and specificity for detection of disease progression must be validated by future studies. In addition, given that CMR was an inclusion requirement, the cohort does not represent all TOF patients since patients in whom CMR is contraindicated (eg, pacemakers/defibrillators), and those in whom quality data could not be obtained (eg, persistent arrhythmias, metallic artefacts and claustrophobia) were not included. It is also worth noting that our study may have underestimated the true prevalence of disease progression since patients who underwent PVR shortly after the first CMR were not included. Another notable limitation is the relatively small sample size of subgroups such as those with and without disease progression among patients with an RV-to-PA conduit. Finally, the results of this study may not apply to young children with repaired TOF because this group of patients was under-represented in this cohort (14% <12 years).
Conclusions
RV dilatation and dysfunction as well as LV dysfunction progress at a slow rate in the majority of adult patients with repaired TOF. However, in approximately 15% of the patients, important worsening in ventricular parameters occurs and is not predictable based on standard demographic, clinical, ECG, exercise and CMR parameters at baseline. Patients with an RV-to-PA conduit and RV dilatation, hypertrophy and borderline systolic function are at increased risk for disease progression. In patients who are not on the verge of fulfilling criteria for PVR, a CMR examination every 3 years appears to be an appropriate surveillance strategy.
Key messages
What is already known on this subject?
Although cardiac magnetic resonance (CMR) is commonly used for surveillance of RV dilation and dysfunction following tetralogy of Fallot (TOF) repair, neither the prevalence of progressive RV disease nor the optimal time interval between CMR evaluations is known.
What might this study add?
This study found substantial deterioration in RV size and/or function and/or LV function in 15% of patients during a median period of 2.2 years. None of the predefined clinical or laboratory parameters at baseline evaluation, including demographic, anatomic, surgical, ECG, exercise or CMR parameters, was predictive of subsequent deterioration in ventricular size and function. A screening interval of 3 years between CMR studies had the highest area under the receiver operator curve for detecting disease progression.
How might this impact on clinical practice?
Given that clinically important deterioration in right heart size and/or ventricular function in patients with repaired TOF cannot be readily predicted, this study suggests that a screening interval of up to 3 years may be suitable for detection of progressive disease. These findings will inform the practice of outpatient surveillance using CMR.
Acknowledgments
The authors would like to thank Sarah P. Evans, BS, and Kelsey Hickey, BA for their assistance with data processing.
References
Footnotes
Contributors RMW: study design, data acquisition (Toronto), analysis and interpretation, writing of manuscript and final approval of the manuscript; AMV: study design, data acquisition (Boston), manuscript editing and final approval of the manuscript; KG: study design, data analysis, manuscript editing and final approval of the manuscript; SVB-N: study design, responsible for the data from London, manuscript editing and final approval of the manuscript; GEA: data acquisition and final approval of the manuscript; JS: data acquisition and final approval of the manuscript; MAG: study design, manuscript editing and final approval of the manuscript; PJK: study design, data acquisition (London) and final approval of the manuscript; BM: study design, data acquisition (Amsterdam), manuscript editing and final approval of the manuscript; ZK: data acquisition and final approval of the manuscript; AJP: study design, manuscript editing and final approval of the manuscript; TG: responsible for all aspects of the project.
Funding RMW is supported by a Canadian Institutes of Health Research operating grant (MOP 119353). TG is a consultant to Medtronic. SVB-N is supported by an Intermediate Clinical Research Fellowship from the British Heart Foundation (FS/11/38/28864). Funding was also provided by the Higgins Family Noninvasive Research Fund at Boston Children's Hospital (TG, AMV, AJP), the Dunlevie Foundation (AMV, JS, GEA) and the Lerner Research award (AMV).
Competing interests None declared.
Ethics approval Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.